Here is a round-up of resources that you may find helpful in your practice.
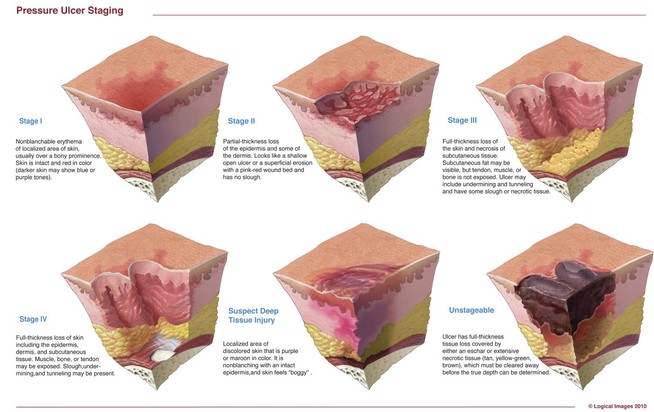
New illustrations for…

Electrical stimulation and pressure ulcer healing in SCI patients
A systematic review of eight clin…

Imagine you have a health condition that affects your life every day. Then imagine being told nothin…

Management of biofilm recommendations
The Journal of Wound Care has published “Recommendations for …

Moldable skin barrier effective for elderly patients with ostomy
A study in Gastroenterology Nursin…

Value of systematic reviews and meta-analyses in wound care
“Systematic reviews and meta-analyses…
Modified Braden risk score proposed
A study in Ostomy Wound Management states the risk classificati…
Mild compression diabetic socks safe and effective for lower extremity edema
Diabetic socks with mi…

By Erin Fazzari, MPT, CLT, CWS, DWC
Have you seen legs like these in your practice?
These le…
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson,…
Factors affecting medication adherence in patients with diabetes identified
Factors associated with…
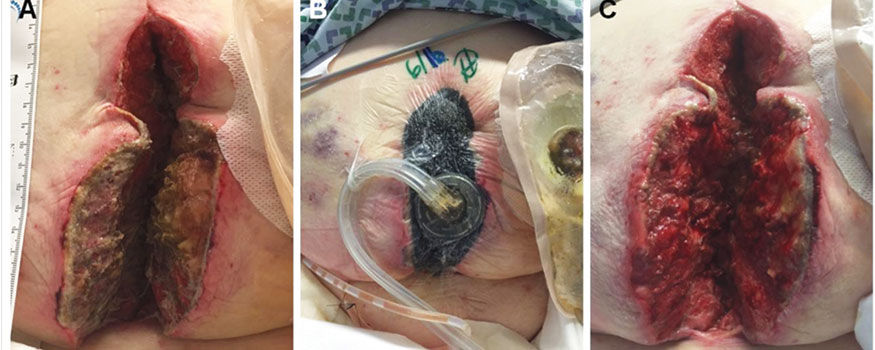
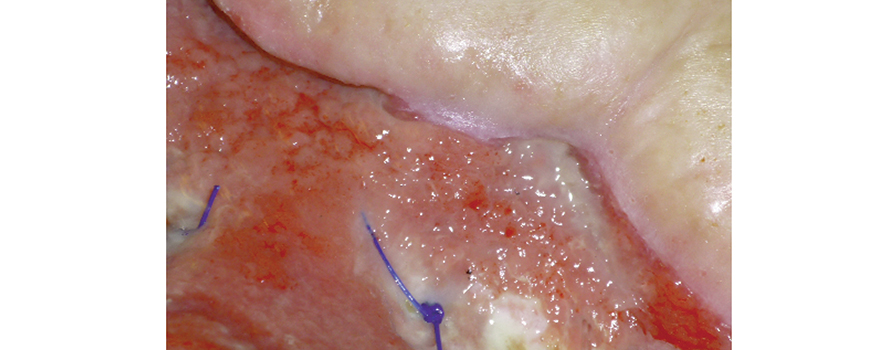
By Erin Fazzari, MPT, CLT, CWS, DWC
Have you seen legs like those shown in the images below in yo…
By Bill Richlen, PT, WCC, DWC, and Denise Richlen, PT, WCC, DCCT
How many times have you heard som…
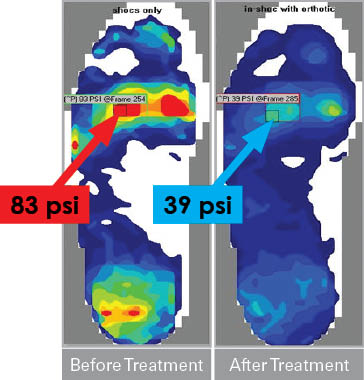
Guidelines for optimal off-loading to prevent diabetic foot ulcers
“The management of diabetic foo…
Diabetes carries high economic burden
According to a study published in Diabetes Care, the economic…
Radiation and lymphedema
Radiation therapy doesn’t increase the incidence of lymphedema in patients…
Wound photography may motivate patients
Having patients view photographs of their wounds can motiva…
Aspirin inhibits wound healing
A study in the Journal of Experimental Medicine describes how aspiri…
Incidence density best measure of pressure-ulcer prevention program
According to the National Press…

Take a few minutes to check out this potpourri of resources.
International Ostomy Association
The …

Low BMD common after ostomy
Low bone mineral density (BMD) is common in patients with inflammatory …
Antibiotics and conservative surgery yield similar outcomes in patients with diabetic foot osteomyel…
Hospital pressure-ulcer comparison data not accurate
Performance scores for rates of hospital-acqui…
Dermatologic difficulties: Skin problems in patients with chronic venous insufficiency and phlebolym…
Frequent debridement improves wound healing
A study in JAMA Dermatology reports that frequent debr…
Critical limb ischemia may not increase mortality risk in patients with diabetes
Diabetic patients …
By Nancy Chatham, RN, MSN, ANP-BC, CCNS, CWOCN, CWS, and Lori Thomas, MS, OTR/L, CLT-LANA
An esti…
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found t…
By: Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
At some point, most of us have encountered a bully—…
By Donald A. Wollheim, MD, WCC, DWC, FAPWCA
To begin appropriate treatment for chronic venous insuf…
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA
One of the worst fears of a wound care clinician is inadver…
Here are resources that can help you in your busy clinical practice by giving you informatio…
An Unna boot is a special dressing of inelastic gauze impregnated with zinc, glycerin, or calamine t…
By Donald A. Wollheim, MD, WCC, DWC, FAPWCA
Chronic venous insufficiency (CVI) is the most common ca…
Diabetes ‘ABC’ goals improve, but work remains
The number of people with diabetes who are meeting th…
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA
In a busy wound clinic, quick and accurate differential dia…
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA
A hot flush of embarrassment creates a bead of sweat on my …
By Steve Norton, CDT, CLT-LANA
Editor’s note: Part 1 of this series, published in the September-Octo…
New wound-swabbing technique detects more bacteria
The new Essen Rotary swabbing technique takes a f…
By Steve Norton, CDT, CLT-LANA
Lymphedema is characterized by regional immune dysfunction, distorted…
2012 guideline for diabetic foot infections released
Foot infections in patients with diabetes usual…
By Joan C. Borgatti, MEd, RN
The alarm clock goes off too early, and you jump-start the day with a c…