What caused Mr. M’s pressure ulcer?
A court case answers the question as to whether a pressure ulcer was preventable
By Nancy J. Brent, MS, RN, JD
Pressure ulcers are a major health risk for every adult patient. Risk factors include sepsis, hypotension, and age 70 or older. These risk factors became all too real when Mr. M developed pressure ulcers after being admitted to a Texas hospital.
Background
Mr. M, age 81, presented at a medical center’s emergency department on January 2 complaining of abdominal pain. After undergoing an assessment, he was diagnosed with gallstones and admitted to the hospital. The next day, he had gallbladder surgery. He subsequently developed a bowel obstruction and had to undergo two more surgeries for this condition over the next 10 days.
On January 13, he was transferred to the intensive care unit (ICU) because of multiple serious medical conditions, including respiratory distress syndrome (necessitating ventilatory support), septic shock, a “blood infection” that caused his blood pressure to drop, and multiorgan failure. His primary physician discontinued tube feedings out of concern they might exacerbate his renal failure; he wrote a do-not-resuscitate order and ordered sedation.
Mr. M was unable to turn or position himself in any way. While in the ICU, he developed a “skin tear” on the tailbone (coccyx) that progressed to a serious pressure ulcer. On February 6, his condition improved enough to allow his transfer to a rehabilitation hospital, where he developed pressure ulcers on his heels. He was transferred to another hospital; the ulcer on his coccyx healed by August. He remained in that hospital for 1 year before being discharged home.
Despite healing of the pressure ulcer on his coccyx, the wound area remained hard and painful, and Mr. M experienced “daily discomfort” there. Also, he was unable to do many of the things he’d been able to do before his hospitalization.
Mr. M files a medical malpractice suit
Mr. M sued the medical center, alleging the hospital was negligent by failing to prevent the pressure ulcer from forming through the use of known “pressure relief” methods, and that the hospital failed to provide proper care and treatment of the wound once it was discovered.
At trial, the medical center lawyers argued that Mr. M’s grave condition caused the pressure ulcer to develop. The jury returned a verdict for Mr. M, finding that the medical center’s negligence proximately caused the injuries he sustained. It awarded him $35,000 for medical expenses; $135,000 for past physical pain and mental anguish; $25,000 for future physical pain and mental anguish; $25,000 for past physical impairment; and $25,000 for future physical impairment. The medical center appealed the decision.
Medical center appeals the verdict
Several issues were raised by the medical center on appeal. Of particular interest to nurses and wound care practitioners was the “cause in fact” or the “proximate cause” of Mr. M’s pressure ulcer on the coccyx. Because an expert witness must establish proximate cause based on a reasonable degree of medical certainty, Mr. M’s case became a battle of the experts regarding the care he received, or lack of care, relative to development of the pressure ulcer.
Expert witness testimony for Mr. M
The first nurse expert to testify was Mr. M’s highly qualified expert. She testified about the various acceptable ways to provide pressure relief, including turning the patient or, if the patient can’t be turned, repositioning. The latter requires use of foam wedges or pillows to elevate a particular body part. The nurse expert testified that if a patient can’t be turned or repositioned, that fact must be documented along with the reason for inability to carry out this nursing care.
Proper assessment of the pressure ulcer is required so that other team members can “see” the wound; the clinician who assesses the wound should draw a picture of exactly what he or she saw when documenting the note in the patient’s chart. The nurse expert testified that the assessment should include the color, duration, and depth of the pressure ulcer; presence or absence of infection; and whether the tissue was dead or perfused.
After reviewing the medical center’s policies and protocols on pressure relief, which required nurses to provide pressure relief every 2 hours, and the depositions of the nurses who’d cared for Mr. M, the nurse expert testified there was no documentation showing Mr. M received any pressure relief from January 13 to January 16. She said she could only conclude that the nurses failed to turn or reposition him during those days. The only notation made about his skin condition was when nurses discovered the “skin tear” on January 14. After this discovery, the physician wasn’t notified of it until January 19. On that date, the physician ordered a wound care consult, but the actual consultation didn’t occur until 3 days later. Even with the wound consultant’s specific, written orders to care for the wound, only one notation existed showing that the orders were followed. Also, the wound care orders weren’t entered into Mr. M’s care plan until January 28. Additionally, in their depositions, the nurses caring for Mr. M couldn’t recall changing the dressing as ordered.
Therefore, in the nurse expert’s opinion, the pressure ulcer on Mr. M’s coccyx was caused directly by failure of the ICU nurses to provide pressure relief from January 14 to January 16 and that providing the wound care that was ordered would have prevented the ulcer from getting worse and would have healed the ulcer.
Although a physician serving as a second expert for Mr. M also testified that pressure relief should have been provided, he couldn’t say that development of the pressure ulcer was unpreventable.
Expert witness testimony for the medical center
Not surprisingly, the medical center’s expert witnesses, two of whom were physicians, testified that because of Mr. M’s general medical condition, he would have developed the pressure ulcer even if hospital policies and protocols had been followed. The hospital’s nurse expert witness stated that Mr. M’s pressure ulcer was not preventable because of his medical condition, regardless of whether or not he was turned. In her opinion, the active range of motion his nurses put him through was enough to reperfuse the area.
Appellate court’s decision
The appellate court upheld the trial court jury’s verdict, stating that evidence presented at the trial was legally and factually sufficient to support that verdict.
Take-away points
Mr. M’s case undoubtedly was complicated by his age and general medical condition, as well as disagreement among expert witnesses as to the cause of the pressure ulcer on his coccyx. Even so, the appellate court held that the evidence at trial (specifically that presented by Mr. M’s nurse expert witness) was sufficient legally and factually to support the verdict in favor of Mr. M.
This case illustrates many areas of importance for nurses in terms of formation and care of pressure ulcers. They include the following:
• Risk factors supporting potential formation of pressure ulcers can’t be overlooked or underestimated by nursing staff.
• A plan to prevent pressure ulcers should be initiated on admission for every patient who is immobile or has other risk factors for pressure ulcers.
• Documentation of every aspect of nursing care that’s initiated and continued to prevent pressure ulcers from forming must be carried out as ordered and pursuant to hospital policy and protocol.
• Care plans, communications with other health team members, and carrying out of orders must be done as soon as possible.
• Assessment and documentation of pressure ulcers should include enough detail so other health team members can visualize what the nurse entering the documentation has seen.
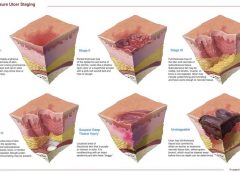
• The nurse should assess and stage the pressure ulcer at each dressing change.
• One’s expert witness must be credentialed, educated, and experienced in would care prevention and treatment, because his or her testimony can win or lose a case.
Nursing remains at the forefront of protecting and safeguarding patients from pressure ulcers. Although not every ulcer can be prevented, the goal is to prevent as many ulcers as possible. If a pressure ulcer does occur, caregivers’ essential focus must be on healing or preventing further deterioration and infection.
Selected references
Columbia Medical Center Subsidiary, L.P., d/b/a/
North Central Medical Center, Appellant, v. John Meier, Appellee. 198 S.W. 3d 408 (Ct. Appeals 2006).
Lyder CH, Ayello EA. Pressure ulcers: A Patient Safety Issue. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook For Nurses. Rockville, MD: Agency For Healthcare Research and Quality. April 2008. www.ncbi.nlm.nih.gov/books/
NBK2650/. Accessed November 1, 2012.
Nancy J. Brent is an attorney in Wilmette, Illinois. The information in this article is for educational purposes only and doesn’t constitute legal advice.
Read More