As a wound care expert, you’re probably consulted for every eruption, scrape, and opening in a patie…

General characteristics
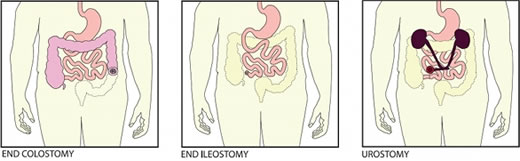
Document if the diversion is an intestinal or urinary ostomy, whether it’s …

Here is a round-up of resources that you may find helpful in your practice.
New illustrations for…

Electrical stimulation and pressure ulcer healing in SCI patients
A systematic review of eight clin…

This issue marks the fourth anniversary of the “Best of the Best” issue of Wound Care Advisor, the o…

It’s been a stressful day at work—nothing new. One confused patient pulled off her ostomy bag, you’r…

Sad but true: Much of what we do as healthcare professionals is based on reimbursement. For nearly a…

Management of biofilm recommendations
The Journal of Wound Care has published “Recommendations for …

According to the National Cancer Institute, an estimated 1.6 million new cases of cancer will have b…
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue.…

For an ostomy pouching system to adhere properly, the skin around the stoma must be dry and intact. …

Moldable skin barrier effective for elderly patients with ostomy
A study in Gastroenterology Nursin…

Check out the following resources, all designed to help you in your clinical practice.
Human traffi…

Self-management ostomy program improves HRQOL
A five-session ostomy self-care program with a curric…

Being positive in a negative situation is not naïve. It’s leadership.
— Ralph S. Marston, Jr., au…

We all lead busy lives, with demanding work schedules and home responsibilities that can thwart our …

At the 2015 Wild on Wounds conference, the interactive workshop “Are You Ready for an Outp…

Value of systematic reviews and meta-analyses in wound care
“Systematic reviews and meta-analyses…

Immobility affects all our body systems, including our skin. According to the National Pressure Ulce…

Start the New Year off right by checking out these resources.
Pressure ulcer prevention education…
Modified Braden risk score proposed
A study in Ostomy Wound Management states the risk classificati…

By Gail R. Hebert, MS, RN CWCN, DWC, WCC, OMS
How would you react if you heard a 600-lb patient w…
By Leanne Richbourg, MSN, RN, APRN-BC, CWON-AP, CCCN, GCNS-BC
Restorative proctocolectomy with il…
End your year by checking out these resources for your practice.
Sentinel event alert f…
By: Donna Sardina, RN, MHA, WCC, CWCMS
What do the Los Angeles Lakers, Green Bay Packers, Montrea…
Mild compression diabetic socks safe and effective for lower extremity edema
Diabetic socks with mi…
Angelini Pharma Inc.
BIOPAD: 100% equine Type-1 collagen primary wound dressing
EXSEPT PLUS: ele…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN
As wound care clinicians, we are trained—and expected—t…

Leg revascularization fails to improve outcomes in nursing home patients
Lower-extremity revascular…
By Beth Hoffmire Heideman, MSN, RN
No one wants an ostomy, but sometimes it’s required to save a pa…
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson,…
Learn about resources useful to your practice.
Nutrition and pressure ulcers
Advances in Skin &…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS
Each issue, Apple Bites brings you a tool you can…
Here is a list of valuable ostomy resources, some suggested by our colleagues who follow Wound Care …
This issue’s resources include patient tools and new guidelines.
Improving patient safety
Research…

Take a few minutes to check out this potpourri of resources.
International Ostomy Association
The …

By Connie Johnson, BSN, RN, WCC, LLE, OMS, DAPWCA
No matter where you work or who your distributo…

By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS…
By Jackie Doubleman, BSN, RN, CWOCN
Most patients are distressed to learn they need ostomy surger…
By Goranka Paula Bak, BSN, RN, ET, CWOCN
Before discharge, a new ostomy patient and caregiver have …
By Goranka Paula Bak, BSN, RN, ET, CWOCN
Every year, thousands of people of all ages have ostomy sur…