Submit your manuscript electronically as an MS Word file. Follow these guidelines:
At the top of the first page of the document, place the article title, your initials (not your name), and the date.
DO NOT include extra hard returns between lines or paragraphs, extra spaces between words, or any special coding.
Send a separate cover letter that includes your name; credentials; position; address; home, cell, and work telephone numbers; email address; and your employer’s name, city, and state.
If your manuscript contains clinical information and we believe it has publication potential, we will send it out for blind peer review (neither you nor the reviewers will know who wrote the article). All manuscripts also receive an internal editorial review. After the review, we’ll let you know whether the manuscript has been accepted, accepted pending revisions, or declined.
If we accept your manuscript for publication, we’ll ask you to sign an agreement that gives HealthCom Media (publisher of Wound Care Advisor) the rights to your article so that it can be published. Each author must sign a separate agreement.
Your article will go through our in-house editorial process, where professional editors ensure consistency with our editorial style. You will have a chance to review the edited version before it’s published.
We will email you if we decide not to publish your manuscript.
Thank you for considering publishing in Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy, the official. If you have any questions, please email: Cynthia Saver, RN, MS, at [email protected] or [email protected].
Optimizing nutritional status is a key strategy both in preventing and managing pressure ulcers. In patients across all care settings, compromised nutrition— as from poor intake, undesired weight loss, and malnutrition—increases the risk of pressure ulcers. It contributes to altered immune function, impaired collagen synthesis, and decreased tensile strength. In many cases, malnutrition also contributes to wound chronicity and increases the risk for delayed and impaired wound healing. In patients with chronic wounds, such as pressure ulcers, a chronic inflammatory state can induce catabolic metabolism, malnutrition, and dehydration. (more…)
Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement you’d feel.
What if you had to live through this experience repeatedly? That’s what many elderly people go through, suffering with skin tears through no fault of their own. Some go on to develop complications.
A skin tear is a traumatic wound caused by shear, friction, or blunt-force trauma that results in a partial- or full-thickness injury. Skin tears are painful because the precipitating injury commonly involves the dermis, which is rich with nerve endings. (more…)
Keeping clinicians up-to-date on clinical knowledge is one of the main goals of the Wild on Wounds (WOW) conference held each September in Las Vegas. Every year, I present the opening session, called “The Buzz Report,” which focuses on the latest-breaking wound care news—what’s new, what’s now, and what’s coming up. I discuss new products, practice guidelines, resources, and tools from the last 12 months in skin, wound, and ostomy management.
In the January issue, I discussed some of the updates from my 2015 Buzz Report. Now I’d like to share a few more, along with some of my favorite resources. (more…)
We all lead busy lives, with demanding work schedules and home responsibilities that can thwart our best intentions. Although we know it’s our responsibility to stay abreast of changes in our field, we may feel overwhelmed when we try to make that happen.
Keeping clinicians up-to-date on clinical knowledge is one of the main goals of the Wild On Wounds (WOW) conference, held each September in Las Vegas. Each year, I present the opening session of this conference, called “The Buzz Report,” which focuses on the latest-breaking wound care news—what’s new, what’s now, what’s coming up. I discuss innovative new products, practice guidelines, resources, and tools from the last 12 months in skin, wound, and ostomy management. This article highlights the hottest topics from my 2015 Buzz Report. (more…)
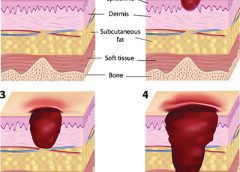
Having the proper support surface for beds and wheelchairs is imperative in preventing pressure ulcers. “Pressure” ulcers are named that for a reason—pressure is the primary cause of interruption of blood flow to the tissue. Unfortunately, guidelines for support surface selection tend to make recommendations for the type of surface to use after a pressure ulcer has developed. Another factor that complicates matters is the development of deep-tissue injuries. These injuries start at the bone level, which means that often, tissue damage is extensive before we see visible signs and realize that the support surface we chose might not have been effective enough. (more…)
A study in Ostomy Wound Management states the risk classification of patients using Braden Scale scores should comprise three (rather than five) levels: high risk, with a total score ≤11; moderate risk, with a total score of 12 to 16; and mild risk, with a total score ≥17.
The retrospective analysis of consecutively admitted patients at risk for pressure ulcer to an acute-care facility included 2,625 patients, with an age range from 1 month to 98 years; 3.1% developed a pressure ulcer. (more…)
As healthcare clinicians, our world is full of tasks to be completed. Some are new, but many are tasks we repeat every day and thus have become routine—things we could almost do in our sleep.
But what’s routine for us may not be routine for our patients. For some patients, these routine tasks of ours may be their first encounter with a healthcare situation. (more…)
Are you using the wrong kind of medical tape on your patients? Although we strive to provide the safest care possible, some nurses may not realize that medical tape used to secure tubes and dressings can cause harm. The harm may stem from using the wrong product or using a product incorrectly, which can cause adhesive failure or skin injury. (more…)
Patients in your clinical practice who develop wounds should prompt a call for “all hands on deck” to manage the situation, but some personnel may be missing the boat. Physical therapists (PTs), occupational therapists (OTs), and speech-language pathologists (SLPs) should be on board your wound care ship so patients can receive care they need. But unfortunately, sometimes they aren’t. (more…)
As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to support and direct the care of pediatric patients with pressure ulcers. This article describes efforts to reduce pressure ulcers in pediatric patients at Driscoll Children’s Hospital (DCH) in Corpus Christi, Texas.
By Erin Fazzari, MPT, CLT, CWS, DWC Have you seen legs like these in your practice? These legs show lymphedema and chronic wounds before treatment (left image) and after treatment (right image) with complex decongestive therapy (CDT)—the gold standard of lymphedema care. The patient benefited from multidisciplinary collaboration between wound care and lymphedema therapists.
By Todd Zortman, RN, WCC, and James Malec, PhD Pressure ulcers are a chronic healthcare burden for both patients and providers. Over 2.5 million patients in the United States are affected annually by pressure ulcers, with nearly 60,000 of those cases directly resulting in death. From a provider’s perspective, the cost of individual care ranges anywhere from $500 to $70,000…
By Janet Wolfson, PT, CWS, CLT-LANA After landing my dream job as the wound care coordinator at an inpatient rehabilitation facility (IRF), I found myself trying to determine how much healing could be achieved for our more challenging patients, given the constraints of reimbursement and what can be done in the typical 10 to 14 days of a patient stay.…
Leg revascularization fails to improve outcomes in nursing home patients Lower-extremity revascularization often fails to improve outcomes in nursing home patients, according to an article in JAMA Internal Medicine. “Functional outcomes after lower extremity revascularization in nursing home residents: A national cohort study” found that few patients are alive and ambulatory a year after surgery, and those who are alive…
Check out these resources for your practice. Be a nutrition champion One in three patients enters a hospital malnourished. Fight malnutrition by viewing six short videos from the Alliance to Advance Patient Nutrition, including “Rapidly Implement Nutrition Interventions” and “Recognize and Diagnose All Patients at Risk of Malnutrition.” The videos show how to collaborate with the care team to become…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of performing a comprehensive skin assessment. In the healthcare setting, a comprehensive skin assessment is a process in which the entire skin of a patient is examined for abnormalities. It requires looking…
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Pressure ulcers have been a health concern for a long time—since at least 5,000 years ago, when evidence of a pressure ulcer was found on an ancient Egyptian mummy. But not until 1975 did the staging classification system we’re familiar with begin. This system was designed to make things easier by…
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular…
By Sharon Morrison, MAT, RN Michael had diabetes and a history of elevated blood glucose levels. A long-time drinker, he seemed to have no interest in giving up the habit. I met him while working as a diabetes nurse educator for the Boston Health Care for the Homeless Program, traveling from shelter to shelter to help persons with diabetes set…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to…
These legs show lymphedema and chronic wounds before treatment (left image) and after treatment (right image) with complex decongestive therapy (CDT)—the gold standard of lymphedema care. The patient benefited from multidisciplinary collaboration between wound care and lymphedema therapists. (more…)