Nurses and therapists often wonder if their license permits them to perform sharp wound debridement. Scope of practice varies significantly from state to state, so it’s imperative to check your state for specific guidance, but we can address some of the challenges clinicians face in deciding whether they can perform this valuable service for patients.
Most of the wounds in the 154,644 patients were diabetic foot ulcers, venous leg ulcers, and pressure ulcers. The study authors note that debridement is a “key process” in wound bed preparation and starting the healing process.
The findings are congruent with previous studies and are based on an analysis of the largest wound data set to date. (more…)
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
Consider these solutions to three common mistakes. Stepping into a formal leadership role is exciting. Whether it’s your first supervisor or manager role or an interim position with the potential to become permanent, the new responsibilities can feel empowering and overwhelming. Many of your finely honed nursing skills will serve you well as a manager,...
Patient-centered care focused on self-sufficiency The Centers for Medicare and Medicaid Services (CMS) uses the term “home health” to describe a federal health insurance program that provides intermittent short-term care to help patients recover from illness and become as self-sufficient as possible at home. Professionals who participate in home health include nurses, physical therapists, occupational...
As nursing and academia have evolved, so too has the definition of faculty practice. It can include clinical practice, scholarship, clinical research, education, consultation, leadership and administration, preceptorship, policy advocacy, and quality improvement management. It also may refer to the clinical work undertaken by nursing faculty who maintain active roles in patient care, health services, […]
The United States continues to experience a shortage of frontline nurses, and a critical nurse faculty shortage impedes efforts to educate nurses to meet clinical workforce demands. In 2021, according to the American Association of Colleges of Nursing, U.S. nursing programs turned away 76,000 qualified prelicensure applicants due to a shortage of nursing faculty. Several...
Shared governance provides clinical nurses with a voice and opportunities to engage within an organization. It allows them to step into leadership roles to strengthen the inpatient, ambulatory, or direct patient care units in which they work.
USN nurses share their deployment experiences. Have you ever thought about a career as a U.S. Navy (USN) nurse? If so, you must consider that USN nurses hold two jobs—Naval officer and RN—and most are assigned to an operational platform for either their primary job responsibility or as a collateral role. USN nurses deploy with...
Nurses of color and those from other marginalized groups face several barriers to pursuing career advancement, including racial discrimination, few role models, and lack of support. However, exposure and mentorship can serve as a mechanism to address the mismatch between patient and nursing workforce demographics
I recently visited an 83-year-old patient in the hospital after EMTs rushed her to the ER with an infected leg wound. Her ordeal started inconspicuously when she bumped into the sharp edge of a table and developed a small cut. The patient’s wound didn’t close, but she ignored it until she woke up in pain one morning two weeks after first injuring her leg. Her daughter called 911 after noticing angry, red skin discoloration and pus – both signs of an infection. Our medical team treated her with IV antibiotics and cleared up the infection, but the wound did not fully close until at least a month later, well after she was discharged from the hospital.
How different the story is when children get a cut. They may scream initially, but within days, the scab falls off, revealing new skin. Why was healing so delayed in my 83-year-old patient compared to a healthy child?
The answer is age. Decades of life slow down healing for most tissues, and wounds in skin can offer a window into why this slowdown occurs.
Three stages of wound healing
I am physician who studies how aging predisposes patients to diseases like diabetes and whether behavioral changes such as intermittent fasting may slow down aging. In order to understand why the skin wound in my older patient healed so slowly, it is important to first understand how wounds heal under the ideal conditions of youth.
The first stage is inflammation, essentially the body’s attempt to clean the wound. During the inflammatory phase, immune cells called phagocytes move into the wound, kill any contaminating bacteria, and ingest and dispose of dead cells and debris.
Inflammation sets the stage for the regenerative phase, where several processes work in concert to regrow damaged skin. Replacement skin cells are born when cells at the edge of the wound divide, while fibroblast cells lay down a supportive scaffolding called the extracellular matrix. This holds the new cells together. Any damaged supporting structures of the skin, such as the blood vessels that supply critical oxygen and nutrients, also need to regrow. The second stage effectively closes the wound and restores a protective barrier against bacteria.
Once the wound is fully closed, the remodeling phase will rebuild the tissue in a stronger way. Jpbarrass via Wikimedia Commons
The regenerative phase is a relatively quick, but tenuous fix – new skin is fragile. The final remodeling phase plays out over a couple of years as the new skin is progressively strengthened by several parallel processes. The extracellular matrix, which was initially laid down in a haphazard fashion, is broken down and replaced in a more durable way. Any residual cells from prior phases that are no longer needed – such as immune cells or fibroblasts – become inactive or die. In addition to strengthening the new skin, these collective actions also account for the tendency of scars to visibly fade with time.
One major way aging can derail the orderly and efficient progression through the stages of healing is through the health problems that stem from diseases of old age.
Diabetes is one example of a disease that is strongly associated with older age. One of the many ways that diabetes negatively affects healing is by causing blood vessels to narrow. As a consequence of inadequate circulation, crucial nutrients and oxygen do not reach the wound in sufficient quantities to fuel the second regenerative phase.
Diabetes is just one of many age-related diseases that disrupts normal processes in the body such as wound healing.
When cells divide more slowly – or when they stop dividing altogether due to senescence – skin becomes thinner. The replacement of fat cells, which form a cushioning layer under the skin, also declines with age. The skin of older patients is therefore more prone to injury in the first place.
Once an older person’s skin is injured, the skin has a harder time healing properly as well. Aging and senescent immune cells cannot defend against bacteria, and the risk of serious skin infection rises. Then in the regenerative stage, slow rates of cell division translate into slow skin regrowth. My patient exhibited all of these negative effects of age – her thin, almost translucent skin ruptured from a minor bump, became infected and took nearly two months to fully regrow.
But senescent cells are more than just dysfunctional bystanders. For reasons that are not yet fully understood, senescent cells release toxic byproducts that damage surrounding tissue and drive inflammation – even when there’s no bacterial threat present. Some of these byproducts can even accelerate senescence in neighboring cells. This suggests that intrinsic aging of cells is in essence contagious and senescent cells actively fuel an uncontrolled cycle of inflammation and tissue damage that further impedes successful regeneration and healing.
A whole body problem
As the most outwardly visible tissue of the body, the skin provides a window into why people heal more slowly with age, but all tissues can be injured and are susceptible to the effects of aging. Injuries may be small, repetitive and build up over time – like the effect of smoking on the lungs. Or they may be discrete and dramatic – such as the death of heart cells with a heart attack. Different tissues may heal in different ways. Yet all tissues share a sensitivity to the repercussions of an aging immune system and a decline in the ability to regrow dead or damaged cells.
Understanding why healing slows down with age is important, but my patient asked a very practical question that physicians often face in one form or another: “Doctor, what can you do for me?”
Unfortunately, current treatment of wounds is fairly old-fashioned and often ineffective. Some of the options available include wound dressing changes, antibiotics when the wound is infected or treatment in a high oxygen chamber when circulation is bad due to diabetes.
There is hope, though, that medicine can do better and that progress in understanding the aging process will lead to new therapies. Neutralizing senescent cells in mice, for example, improves a variety of age-associated diseases. While it is way too early to say that researchers have discovered the fountain of youth, I am optimistic for a future when physicians will bend the aging curve and make skin and other organs heal faster and better.
Hansen’s disease, also called leprosy, is treatable today – and that’s partly thanks to a curious tree and the work of a pioneering young scientist in the 1920s. Centuries prior to her discovery, sufferers had no remedy for leprosy’s debilitating symptoms or its social stigma.
This young scientist, Alice Ball, laid fundamental groundwork for the first effective leprosy treatment globally. But her legacy still prompts conversations about the marginalization of women and people of color in science today.
Alice Augusta Ball, born in Seattle, Washington, in 1892, became the first woman and first African American to earn a master’s degree in science from the College of Hawaii in 1915, after completing her studies in pharmaceutical chemistry the year prior.
After she finished her master’s degree, the college hired her as a research chemist and instructor, and she became the first African American with that title in the chemistry department.
Doctors now understand that leprosy, also called Hansen’s disease, is minimally contagious. But in 1865, the fear and stigma associated with leprosy led authorities in Hawaii to implement a mandatory segregation policy, which ultimately isolated those with the disease on a remote peninsula on the island of Molokai. In 1910, over 600 leprosy sufferers were living in Molokai.
Doctors had attempted to use nearly every remedy imaginable to treat leprosy, even experimenting with dangerous substances such as arsenicand strychnine. But the lone consistently effective treatment was chaulmoogra oil.
Chaulmoogra oil is derived from the seeds of the chaulmoogra tree. Health practitioners in India and Burma had been using this oil for centuries as a treatment for various skin diseases. But there were limitations with the treatment, and it had only marginal effects on leprosy.
The oil is very thick and sticky, which makes it hard to rub into the skin. The drug is also notoriously bitter, and patients who ingested it would often start vomiting. Some physicians experimented with injections of the oil, but this produced painful pustules.
Dr. Isabel Kerr, a European missionary, administering to a patient a chaulmoogra oil treatment in 1915, prior to the invention of the Ball Method. George McGlashan Kerr, CC BY
The Ball Method
If researchers could harness chaulmoogra’s curative potential without the nasty side effects, the tree’s seeds could revolutionize leprosy treatment. So, Hollmann turned to Ball. In a 1922 article, Hollmann documents how the 23-year-old Ball discovered how to chemically adapt chaulmoogra into an injection that had none of the side effects.
The Ball Method, as Hollmann called her discovery, transformed chaulmoogra oil into the most effective treatment for leprosy until the introduction of sulfones in the late 1940s.
In 1920, the Ball Method successfully treated 78 patients in Honolulu. A year later, it treated 94 more, with the Public Health Service noting that the morale of all the patients drastically improved. For the first time, there was hope for a cure.
Ball’s death meant she didn’t have the opportunity to publish her research. Arthur Dean, chair of the College of Hawaii’s chemistry department, took over the project.
Dean mass-produced the treatment and published a series of articles on chaulmoogra oil. He renamed Ball’s method the “Dean Method,” and he never credited Ball for her work.
Ball’s other colleagues did attempt to protect Ball’s legacy. A 1920 article in the Journal of the American Medical Association praises the Ball Method, while Hollmann clearly credits Ball in his own 1922 article.
Ball is described at length in a 1922 article in volume 15, issue 5, of Current History, an academic publication on international affairs. That feature is excerpted in a June 1941 issue of Carter G. Woodson’s “Negro History Bulletin,” referring to Ball’s achievement and untimely death.
Joseph Dutton, a well-regarded religious volunteer at the leprosy settlements on Molokai, further referenced Ball’s work in a 1932 memoir broadly published for a popular audience.
Historians such as Paul Wermager later prompted a modern reckoning with Ball’s poor treatment by Dean and others, ensuring that Ball received proper credit for her work. Following Wermager’s and others’ work, the University of Hawaii honored Ball in 2000 with a bronze plaque, affixed to the last remaining chaulmoogra tree on campus.
In 2019, the London School of Hygiene and Tropical Medicine added Ball’s name to the outside of its building. Ball’s story was even featured in a 2020 short film, “The Ball Method.”
The Ball Method represents both a scientific achievement and a history of marginalization. A young woman of color pioneered a medical treatment for a highly stigmatizing disease that disproportionately affected an already disenfranchised Indigenous population.
In 2022, then-Gov. David Ige declared Feb. 28 Alice Augusta Ball Day in Hawaii. It was only fitting that the ceremony took place on the Mānoa campus in the shade of the chaulmoogra tree.
Debbie King barely gave it a second thought when she scraped her right shin climbing onto her friend’s pontoon for a day of boating in the Gulf of Mexico on Aug. 13.
Even though her friend immediately dressed the slight cut, her shin was red and sore when King awoke the next day. It must be a sunburn, she thought.
But three days later, the red and blistered area had grown. Her doctor took one look and sent King, 72, to the emergency room.
Doctors at HCA Florida Citrus Hospital in Inverness, Florida, rushed King into surgery after recognizing the infection as Vibrio vulnificus, a potentially fatal bacterium that kills healthy tissue around a wound. While King lay on the operating table, the surgeon told her husband she would likely die if they didn’t amputate.
Just four days after the scrape, King lost her leg then spent four days in intensive care.
“The flesh was gone; it was just bone,” she said of her leg.
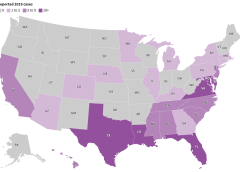
Cases of V. vulnificus are rare. Between 150 and 200 are reported to the Centers for Disease Control and Prevention every year, with about 20% resulting in death. Most are in states along the Gulf of Mexico, but, in 2019, 7% were on the Pacific Coast. Florida averages about 37 cases and 10 deaths a year.
But a rise in cases nationally and the spread of the disease to states farther north — into coastal communities in states such as Connecticut, New York, and North Carolina — have heightened concerns about the bacterium, which can result in amputations or extensive removal of tissue even in those who survive its infections. And warmer coastal waters caused by climate change, combined with a growing population of older adults, may result in infections doubling by 2060, a study in Scientific Reports warned earlier this year.
“Vibrio distributions are driven in large part by temperature,” said Tracy Mincer, an assistant professor at Florida Atlantic University. “The warmer waters are, the more favorable it is for them.”
The eastern United States has seen an eightfold increase in infections over a 30-year period through 2018 as the geographic range of infections shifted north by about 30 miles a year, according to the study, which was cited in a CDC health advisory last month.
The advisory was intended to make doctors more aware of the bacterium when treating infected wounds exposed to coastal waters. Infections can also arise from eating raw or undercooked seafood, particularly oysters, it warned. That can cause symptoms as common as diarrhea and as serious as bloodstream infections and severe blistered skin lesions.
New York and Connecticut this summer issued health warnings about the risk of infection as well. It’s not the first year either state has recorded cases.
“There’s very few cases but when they happen, they’re devastating,” said Paul A. Gulig, a professor in the Department of Molecular Genetics and Microbiology at the University of Florida College of Medicine.
‘An Accident of Nature’
Vibrio has more than 100 strains, including the bacterium that causes cholera, a disease that causes tens of thousands of deaths worldwide each year.
The V. vulnificus strain likes warm brackish waters close to shorelines where the salinity is not as high as in the open sea. Unlike some other Vibrio strains, it has no mechanism to spread between humans.
It’s found in oysters because the mollusks feed by filtering water, meaning the bacterium can become concentrated in oyster flesh. It can enter humans who swim in salty or brackish waters through the slightest cut in the skin. Infections are treated with antibiotics and, if needed, surgery.
“It’s almost an accident of nature,” Gulig said. “They have all these virulence factors that make them really destructive, but we’re not a part of this bug’s life cycle.”
Once inside the human body, the bacteria thrive.
Scientists don’t believe the bacteria eat flesh, despite how they’re often described. Rather, enzymes and toxins secreted by the bacterium as it multiplies break down the human tissue in the area below the skin, causing necrosis, or death of tissue cells.
The infection spreads like wildfire, Gulig said, making early detection critical.
“If you take a pen and mark where the edge of the redness is and then look at that two or four hours later, the redness would have moved,” Gulig said. “You can almost sit there and watch this spread.”
Researchers have conducted studies on the bacteria, but the small number of cases and deaths make it tough to secure funding, said Gulig. He said he switched his research focus to other areas because of the lack of money.
But growing interest in the bacteria has prompted talk about new research at his university’s Emerging Pathogens Institute.
Examining the bacteria’s genome sequence and comparing it with those of Vibrio strains that don’t attack human flesh could yield insights into potential drugs to interfere with that process, Gulig said.
Shock and Loss
Inside the operating room at HCA Florida Citrus, the only signs of King’s infection were on her shin. The surgeon opened that area and began cutting away a bright red mush of dead flesh.
Hoping to save as much of the leg as possible, the doctor first amputated below her knee.
But the bacteria had spread farther than doctors had hoped. A second amputation, this time 5 inches above the knee, had to be performed.
After surgery, King remained in critical care for four days with sepsis, a reaction to infection that can cause organs to fail.
Her son was there when she awakened. He was the one who told her she had lost her leg, but she was too woozy from medication to take it in.
It wasn’t until she was transferred to a rehab hospital in nearby Brooksville run by Encompass Health that the loss sank in.
A former radiation protection technician, King had always been self-reliant. The idea of needing a wheelchair, of being dependent on others — it felt like she had lost part of her identity.
One morning, she could just not stop crying. “It hit me like a ton of bricks,” she said.
Six different rehab staffers told her she needed to meet with the hospital’s consulting psychologist. She thought she didn’t need help, but she eventually gave in and met with Gerald Todoroff.
In four sessions with King, he said, he worked to redirect her perception of what happened. Amputation is not who you are but what you will learn to deal with, he told her. Your life can be as full as you wish.
“They were magic words that made me feel like a new person,” King said. “They went through me like music.”
Physical therapy moved her forward, too. She learned how to stand longer on her remaining leg, to use her wheelchair, and to maneuver in and out of a car.
Now, back in her Gulf Coast community of Homosassa, those skills have become routine. Her husband, Jim, a former oil company worker and carpenter, built an access ramp out of concrete and pressure-treated wood for their single-story home.
But she is determined to walk with the aid of a prosthetic leg. It’s the motivation for a one-hour regimen of physical therapy she does on her own every day in addition to twice-weekly sessions with a physical therapist.
Recovery still feels like a journey but one marked by progress. She has nicknamed her “stump” Peg. She’s now comfortable sharing before and after pictures of her leg.
And she’s made it her mission to talk about what happened so more people will learn about the danger.
“This is the most horrific thing that can happen to anybody,” she said. “But I’d sit back and think, ‘God put you here for a reason — you’ve got more things to do.’”
What to Know About ‘Flesh-Eating’ Bacterium Vibrio vulnificus
Infection Symptoms:
Diarrhea, often accompanied by stomach cramping, nausea, vomiting, and fever.
Wound infections cause redness, pain, swelling, warmth, discoloration, and discharge. They may spread to the rest of the body and cause fever.
Bloodstream infections cause fever, chills, dangerously low blood pressure, and blistering skin lesions.
To Protect Against Vibrio Infections:
Stay out of saltwater or brackish water if you have a wound or a recent surgery, piercing, or tattoo.
Cover wounds with a waterproof bandage if they could come into contact with seawater or raw or undercooked seafood and its juices.
Wash wounds and cuts thoroughly with soap and water after contact with saltwater, brackish water, raw seafood, or its juices.
Who Is Most at Risk:
Anyone can get a wound infection. People with liver disease, cancer, or diabetes, and those over 40 or with weakened immune systems, are more likely to get an infection and have severe complications.
This article was produced in partnership with the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Antibiotic overuse contributes to the problems of antibiotic resistance and healthcare acquired infections, such as Clostridium difficile. Antibiotic stewardship programs improve patient outcomes, reduce antimicrobial resistance, and save money. These programs are designed to ensure patients receive the right antibiotic, at the right dose, at the right time, and for the right duration. (more…)
One of the most amazing things about the human body is its ability to repair itself. Lacerations, punctures, abrasions all heal with little or no care. Chronic wounds, those that persist day after day, are a small subset of wounds but they compose a troublesome minority. They include, but are not limited to, diabetic foot ulcers (DFU), venous leg ulcers (VLU), and pressure ulcers (colloquially known as bedsores). These represent the body’s failure to fix itself. (more…)
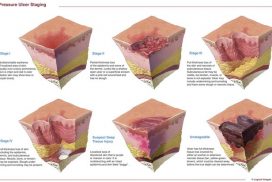
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Staging pressure ulcers can be challenging. Below are some common questions—and answers—about staging. Q. If a pressure ulcer heals (completely epithelialized over), but later reopens at the same site, how should it be staged?
How to apply silver nitrate
Topical application of silver nitrate is often used in wound care to help remove and debride hypergranulation tissue or calloused rolled edges in wounds...
Wound exudate types
BY: NANCY MORGAN, RN, BSN, MBA, WOCN, WCC, CWCMS, DWC What exactly is wound exudate? Also known as drainage, exudate...
What you need to know about hydrocolloid dressings
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each month, Apple Bites brings you a tool you can...
What’s causing your patient’s lower-extremity redness?
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA The ability to understand or “read” lower-extremity redness in your patient is essential...
How to assess wound exudate
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can...
Understanding stoma complications
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC About 1 million...
What you need to know about collagen wound dressings
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Description Collagen, the protein that gives the skin its tensile...
How dietary protein intake promotes wound healing
By Nancy Collins, PhD, RD, LD/N, FAPWCA, and Allison Schnitzer Nutrition is a critical factor in the wound healing process,...
By Matthew Steinhauser, University of Pittsburgh I recently visited an 83-year-old patient in the hospital after EMTs rushed her to the ER with an infected leg wound. Her ordeal started inconspicuously when she bumped...
BioLab Sciences, an innovator in regenerative medicine technologies, has announced the patent of MyOwn SkinTM, a new, non-evasive, regenerative tissue...
On December 28, 2017, the FDA gave approval for the Dermapace System, a shock wave device intended to be used...
About WoundCareAdvisor.com
GOAL
WoundCareAdvisor.com is a unique educational web destination that has been designed to be a trusted, timely and useful resource for healthcare professionals dealing with chronic wounds and ostomy management issues. Offerings on the side currently include
News
Peer-reviewed articles
Product information
Provider/patient education
Practical resources
Information on the site is continuously developed and updated to ensure that we are providing
Resources and information that is
Unique to the wound care field
Timely
Informative
Interactive
WoundCareAdvisor.com is also going to be growing! Future information will include:
A 39-year-old woman presents to the ED with leg pain and fever. She initially noted redness and pain above her knee 2 weeks ago and was evaluated at an outside hospital. She completed a 10-day course of oral antibiotics for cellulitis. Over the last two days, she has had progressive leg swelling of her entire right thigh. The pain is now so severe that she is having difficulty walking. Her past medical history is negative for diabetes mellitus, chronic liver disease, or alcohol and IV drug use.
On exam, she is febrile to 102.7 F, heart rate is 96 bpm, and blood pressure is 112/65. She has a 12 cm area of faint erythema on her right thigh and tenderness to palpation of her entire right leg with diffuse edema. There is no ecchymosis or bullae formation. (more…)