
Long-Term Outcome of Pediatric Traumatic Wound Repair: Suture Versus Tissue Adhesive
Summary
This project is an observational trial investigating wound cosmetic appearance after repair…

Breaking silos: Effective wound healing means treatment across the continuum
Around 6.5 million patients in the U.S. suffer from chronic wounds, such as pressure injuries or ulc…

NYU docs use machine learning
Lymphedema causes unsightly swelling in the arms and legs. But researchers Mei Fu and Yao Wang have …

One Doctor Exploring Wound Care on Earth and in Space
In laboratories all across the globe, scientists are uncovering new and exciting breakthroughs in th…
Management of Patients With Venous Leg Ulcers
It is well documented that the prevalence of venous leg ulcers (VLUs) is increasing, coinciding with…

Reduction of 50% in Diabetic Foot Ulcers With Stem Cells
MUNICH — Local injection of mesenchymal stem cells derived from autologous bone marrow shows promise…

Better Skin Grafts – take only one layer
Research shows that a skin-graft harvesting system aids chronic wound recovery and reduces care cost…
Skin substitutes: Understanding product differences
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wo…

Frequently asked questions about support surfaces
The National Pressure Ulcer Advisory Panel (NPUAP) describes support surfaces as “specialized device…

Herpes zoster: Understanding the disease, its treatment, and prevention
Herpes zoster (HZ, also called shingles) is a painful condition that produces a maculopapular and ve…

Lymphedema and lipedema: What every wound care clinician should know
Imagine you have a health condition that affects your life every day. Then imagine being told nothin…

Clinician Resources
Wound patient’s bill of rights
The Association for Advancement of Wound Care has developed the “Wou…
Instill instead: Negative pressure wound therapy with instillation for complex wounds
Negative pressure wound therapy (NPWT) uses negative pressure to draw wound edges together, remove e…

Doing it cheaply vs. doing what’s best for patients
Sad but true: Much of what we do as healthcare professionals is based on reimbursement. For nearly a…

Clinical Notes: biofilm, bariatric surgery, statins and more
Management of biofilm recommendations
The Journal of Wound Care has published “Recommendations for …

Wise use of antibiotics in patients with wound infections
Antibiotic resistance is a pressing public health threat not only in the United States, but worldwid…
Causes, prevention, and treatment of epibole
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue.…

Clinical Notes: Moldable Skin Barrier, hypoglycemia, diabetic food ulcers
Moldable skin barrier effective for elderly patients with ostomy
A study in Gastroenterology Nursin…

Clinician Resources: human trafficking, npuap, caregiver, ostomy, HIV
Check out the following resources, all designed to help you in your clinical practice.
Human traffi…

How to apply silver nitrate
Topical application of silver nitrate is often used in wound care to help remove and debride hypergr…

No more skin tears
Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement yo…

Clinical Notes: ostomy, pressure ulcer, burn treatment
Self-management ostomy program improves HRQOL
A five-session ostomy self-care program with a curric…

Buzz Report: Latest trends, Part 1
We all lead busy lives, with demanding work schedules and home responsibilities that can thwart our …

Don’t go it alone
A fundamental rule of wound care is to treat the “whole” patient, not just the “hole” in the patient…

Clincal Notes: Analysis, Osteomyelitis, sickle cell, maggot
Value of systematic reviews and meta-analyses in wound care
“Systematic reviews and meta-analyses…

Restorative nursing programs help prevent pressure ulcers
Immobility affects all our body systems, including our skin. According to the National Pressure Ulce…

Clinician Resources: Ulcer Prevention, CAUTI, Negative Bacteria
Start the New Year off right by checking out these resources.
Pressure ulcer prevention education…
Clinician Resources: NPUAP, Pressure Ulcer Treatment, NIOSH
The resources below will help you address issues in your practice.
NPUAP position statement on ha…
Providing evidence-based care for patients with lower-extremity cellulitis
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson,…

Ankle-brachial index: A dirty word?
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Silence, roving eyes, fidgeting, excuses, a quick subj…
Palliative wound care: Part 2
This approach brings patient-centered care to life.
By Gail Rogers Hebert, MS, RN, CWCN, WCC, DWC,…

Using maggots in wound care: Part 2
By Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA
Note From the Editor…

Using maggots in wound care: Part 1
By: Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA
Maggot therapy is t…
Clinician Resources: Patient Safety, Ostomy, Wound Management
This issue’s resources include patient tools and new guidelines.
Improving patient safety
Research…
Guidelines for safe negative-pressure wound therapy
By Ron Rock MSN, RN, ACNS-BC
Since its introduction almost 20 years ago, negative-pressure wound …

Clinician Resources: Intl Ostomy Assoc., Substance Use Disorder
Take a few minutes to check out this potpourri of resources.
International Ostomy Association
The …
“This is how we’ve always done it” isn’t good enough
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Have you ever faced responsibility for a patient-car…

When and how to culture a chronic wound
By Marcia Spear, DNP, ACNP-BC, CWS, CPSN
Chronic wound infections are a significant healthcare bu…
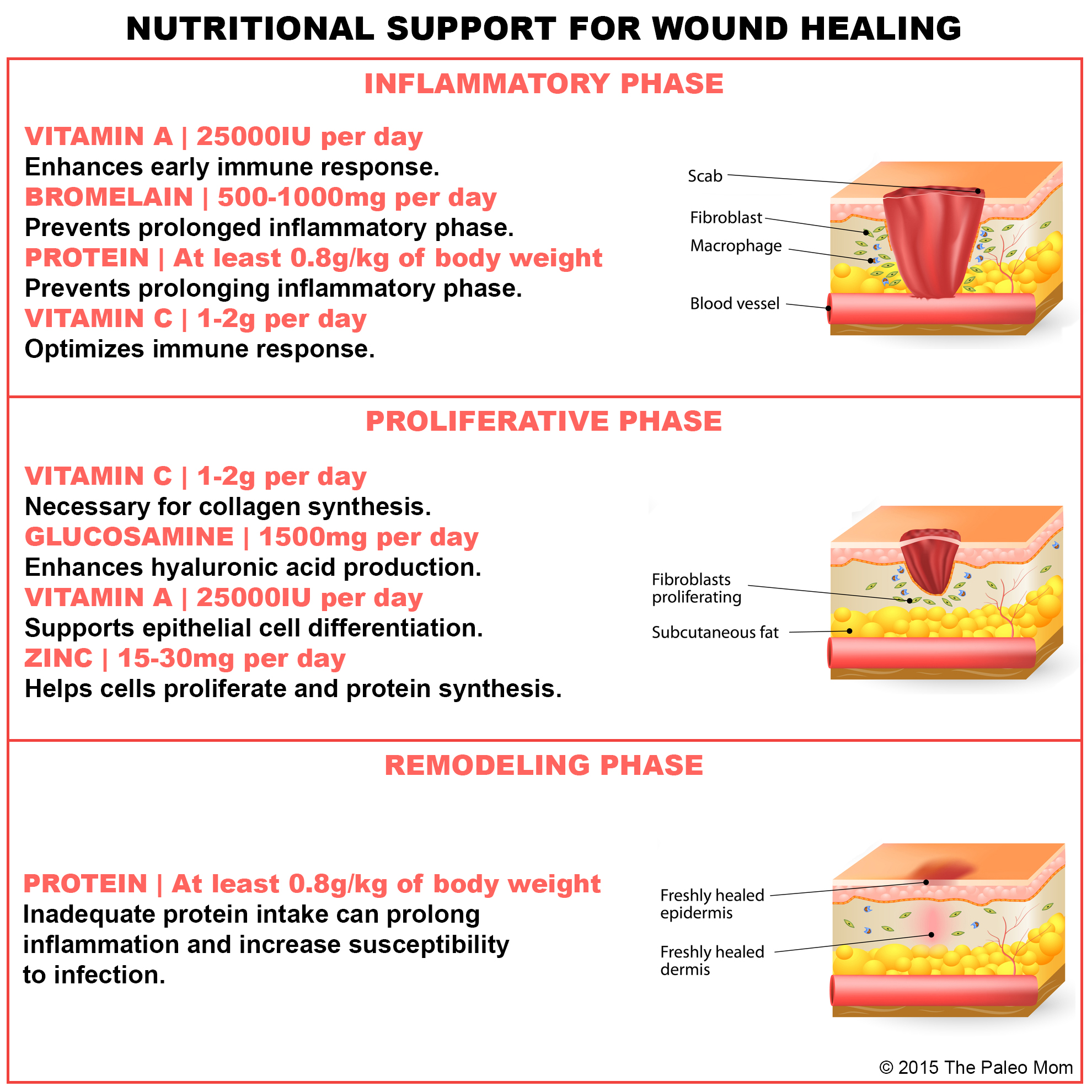
How dietary protein intake promotes wound healing
By Nancy Collins, PhD, RD, LD/N, FAPWCA, and Allison Schnitzer
Nutrition is a critical factor in …
From the Editor – Wound care superhero
by Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
What an honor it is to be the wound care “superhe…

Understanding stoma complications
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC
Abou…
Hyperbaric oxygen therapy for treatment of diabetic foot ulcers
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT
Every year, 1…
Lymphedema 101 – Part 2: Treatment
By Steve Norton, CDT, CLT-LANA
Editor’s note: Part 1 of this series, published in the September-Octo…
Ask the treatment expert: Should treatment nurses be certified?
Click here to read this article.…
Discovery Promises Unique Medicine for Treatment of Chronic and Diabetic Wounds
Click here to read this article.…








