Are you using the wrong kind of medical tape on your patients? Although we strive to provide the safest care possible, some nurses may not realize that medical tape used to secure tubes and dressings can cause harm. The harm may stem from using the wrong product or using a product incorrectly, which can cause adhesive failure or skin injury. (more…)
Patients in your clinical practice who develop wounds should prompt a call for “all hands on deck” to manage the situation, but some personnel may be missing the boat. Physical therapists (PTs), occupational therapists (OTs), and speech-language pathologists (SLPs) should be on board your wound care ship so patients can receive care they need. But unfortunately, sometimes they aren’t. (more…)
What do the Los Angeles Lakers, Green Bay Packers, Montreal Canadiens, and New York Yankees have in common? All three have “three-peated”, meaning they have won three consecutive championships. This year, we at Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy (NAWCO), mark our own three-peat—our third annual “Best of the Best” issue. (more…)
Mild compression diabetic socks safe and effective for lower extremity edema
Diabetic socks with mild compression can reduce lower extremity edema in patients with diabetes without adversely affecting arterial circulation, according to a randomized control trial presented at the American Diabetes Association 75th Scientific Sessions Conference. (more…)
As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to support and direct the care of pediatric patients with pressure ulcers. This article describes efforts to reduce pressure ulcers in pediatric patients at Driscoll Children’s Hospital (DCH) in Corpus Christi, Texas.
By Erin Fazzari, MPT, CLT, CWS, DWC Have you seen legs like these in your practice? These legs show lymphedema and chronic wounds before treatment (left image) and after treatment (right image) with complex decongestive therapy (CDT)—the gold standard of lymphedema care. The patient benefited from multidisciplinary collaboration between wound care and lymphedema therapists.
By Todd Zortman, RN, WCC, and James Malec, PhD Pressure ulcers are a chronic healthcare burden for both patients and providers. Over 2.5 million patients in the United States are affected annually by pressure ulcers, with nearly 60,000 of those cases directly resulting in death. From a provider’s perspective, the cost of individual care ranges anywhere from $500 to $70,000…
By Janet Wolfson, PT, CWS, CLT-LANA After landing my dream job as the wound care coordinator at an inpatient rehabilitation facility (IRF), I found myself trying to determine how much healing could be achieved for our more challenging patients, given the constraints of reimbursement and what can be done in the typical 10 to 14 days of a patient stay.…
Leg revascularization fails to improve outcomes in nursing home patients Lower-extremity revascularization often fails to improve outcomes in nursing home patients, according to an article in JAMA Internal Medicine. “Functional outcomes after lower extremity revascularization in nursing home residents: A national cohort study” found that few patients are alive and ambulatory a year after surgery, and those who are alive…
Check out these resources for your practice. Be a nutrition champion One in three patients enters a hospital malnourished. Fight malnutrition by viewing six short videos from the Alliance to Advance Patient Nutrition, including “Rapidly Implement Nutrition Interventions” and “Recognize and Diagnose All Patients at Risk of Malnutrition.” The videos show how to collaborate with the care team to become…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of performing a comprehensive skin assessment. In the healthcare setting, a comprehensive skin assessment is a process in which the entire skin of a patient is examined for abnormalities. It requires looking…
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Pressure ulcers have been a health concern for a long time—since at least 5,000 years ago, when evidence of a pressure ulcer was found on an ancient Egyptian mummy. But not until 1975 did the staging classification system we’re familiar with begin. This system was designed to make things easier by…
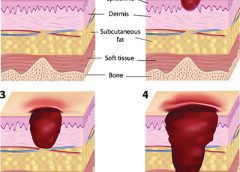
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular…
By Sharon Morrison, MAT, RN Michael had diabetes and a history of elevated blood glucose levels. A long-time drinker, he seemed to have no interest in giving up the habit. I met him while working as a diabetes nurse educator for the Boston Health Care for the Homeless Program, traveling from shelter to shelter to help persons with diabetes set…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to…
These legs show lymphedema and chronic wounds before treatment (left image) and after treatment (right image) with complex decongestive therapy (CDT)—the gold standard of lymphedema care. The patient benefited from multidisciplinary collaboration between wound care and lymphedema therapists. (more…)
Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular body part and failure to redistribute the pressure can lead to ischemia and therefore tissue damage.” Thus, immobility is frequently the root cause of pressure ulcer development. (more…)
Pressure ulcers are a chronic healthcare burden for both patients and providers. Over 2.5 million patients in the United States are affected annually by pressure ulcers, with nearly 60,000 of those cases directly resulting in death. From a provider’s perspective, the cost of individual care ranges anywhere from $500 to $70,000 per pressure ulcer, which translates to annual costs in the U.S. approaching $11 billion. (more…)
Michael had diabetes and a history of elevated blood glucose levels. A long-time drinker, he seemed to have no interest in giving up the habit. I met him while working as a diabetes nurse educator for the Boston Health Care for the Homeless Program, traveling from shelter to shelter to help persons with diabetes set goals to improve their health.
If our meeting had taken place a decade earlier, I might have given Michael information about diabetes and talked with him about his alcohol use. I would have encouraged him to stop drinking by explaining the problems alcohol can cause for people with diabetes. (more…)
After landing my dream job as the wound care coordinator at an inpatient rehabilitation facility (IRF), I found myself trying to determine how much healing could be achieved for our more challenging patients, given the constraints of reimbursement and what can be done in the typical 10 to 14 days of a patient stay.
Here’s an example of how I worked with our team to help one of these challenging patients. (more…)