Collagen, the protein that gives the skin its tensile strength, plays a key role
in each phase of wound healing. It attracts cells, such as fibroblasts and keratinocytes, to the wound, which encourages debridement, angiogenesis, and reepithelialization. In addition, collagen provides a natural scaffold or substrate for new tissue growth. (more…)
By Janice M. Beitz, PhD, RN, CS, CNOR, CWOCN, CRNP
Quality patient education is essential for comprehensive health care and will become reimbursable under healthcare reform in 2014. However, it’s difficult to provide effective education when time for patient interactions is limited. You can enhance your instruction time—and make your teaching more memorable—by using the techniques of analogy and metaphor. (more…)
Pressure ulcers take a hefty toll in both human and economic terms. They can lengthen patient stays, cause pain and suffering, and increase care costs. The average estimated cost of treating a pressure ulcer is $50,000; this amount may include specialty beds, wound care supplies, nutritional support, and increased staff time to care for wounds. What’s more, national patient safety organizations and insurance payers have deemed pressure ulcers avoidable medical errors and no longer reimburse the cost of caring for pressure ulcers that develop during hospitalization.
Frequent debridement improves wound healing A study in JAMA Dermatology reports that frequent debridements speed wound healing. “The more frequent the debridement, the better the healing outcome,” concludes “Frequency of debridements and time to heal: A retrospective cohort study of 312 744 wounds.” The median number of debridements was two. Most of the wounds in the 154,644 patients were diabetic foot…
Here are some resources of value to your practice. National Guideline Clearinghouse The National Guideline Clearinghouse, supported by the Agency for Healthcare Research and Quality, summarizes many guidelines of interest to wound care, ostomy, and lymphedema clinicians. Here are some examples: Guideline for management of wounds in patients with lower-extremity neuropathic disease Pressure ulcer prevention and treatment protocol Lower limb…
By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS Imagine your physician has just told you that your rectal pain and bleeding are caused by invasive colon cancer and you need prompt surgery. She then informs you that surgery will reroute your feces to an opening on your abdominal wall.…
By Rose O. Sherman, EdD, RN, NEA-BC, FAAN Unfortunately, most clinicians can’t avoid having to work with difficult people. However we can learn how to be more effective in these situations, keeping in mind that learning to work with difficult people is both an art and a science. How difficult people differ from the rest of us We can all…
By Tamera L. Brown, MS, RN, ACNS-BC, CWON, and Jessica Kitterman, BSN, RN, CWOCN Pressure ulcers take a hefty toll in both human and economic terms. They can lengthen patient stays, cause pain and suffering, and increase care costs. The average estimated cost of treating a pressure ulcer is $50,000; this amount may include specialty beds, wound care supplies, nutritional…
By Gregory S. Kopp, RN, MN, MHA A new job can be stimulating, but it can also be stressful. Not only will you have new responsibilities, but you’ll also have a new setting, new leaders, and new colleagues. And the quicker you can figure out who’s who and what’s what—without stepping on anyone’s toes—the better off you’ll be. But establishing…
By Ronnel Alumia, BSN, RN, WCC, CWCN, OMS Achieving excellent wound care outcomes can be challenging, given the growing number of high-risk patients admitted to healthcare facilities today. Many of these patients have comorbidities, such as obesity, diabetes, renal disease, smoking, chronic obstructive pulmonary disease, and poor nutritional status. These conditions reduce wound-healing ability.
By Janice M. Beitz, PhD, RN, CS, CNOR, CWOCN, CRNP Quality patient education is essential for comprehensive health care and will become reimbursable under healthcare reform in 2014. However, it’s difficult to provide effective education when time for patient interactions is limited. You can enhance your instruction time—and make your teaching more memorable—by using the techniques of analogy and metaphor.
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN The first 24 hours after a patient’s admission are critical in preventing pressure ulcer development or preventing an existing ulcer from worsening. A skin inspection, risk assessment, and temporary care plan should all be implemented during this time frame. Essentially, it’s the burden of the care setting to prove to insurers, regulators,…
By: Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Why is it that the people who are the most caring toward others neglect their own needs? Have you noticed this? I’ve seen it time and time again. The healthcare worker who’s always the last to leave work, who always volunteers to work those extra shifts so patient care won’t be…
With so much focus on dressing choices, it’s easy to forget the importance of wound cleansing. Cleaning a wound removes loose debris and planktonic (free-floating) bacteria, provides protection to promote an optimal environment for healing, and facilitates wound assessment by optimizing visualization of the wound. You should clean a wound every time you change a dressing, unless it’s contraindicated.
Here’s a review of how to choose and use a wound cleanser so you can see if your practice is up to date. (more…)
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
The guidelines include recommendations for practice, education, policy, and future resource. Strategies for implementation are given, as well as several useful appendices, such as:
• Debridement Decision-Making Algorithm
• A Guide to Dressing Foot Wounds
• PEDIS: Diabetes Foot Ulcer Classification System
• Offloading Devices
• Optimal Treatment Modalities.
PREPARE is a useful and patient-friendly website designed to help prepare people to make complex medical decisions. The website was developed by clinical researchers from the San Francisco VA Medical Center; the University of California, San Francisco; and NCIRE—The Veterans Health Research Institute.
PREPARE uses videos to provide concrete examples of how to identify what is most important in life; how to communicate that with family, friends, and doctors; and how to make informed medical decisions when the time comes. Users can also download a PDF of a PREPARE pamphlet.
Free guides for infection prevention from APIC
Download two free implementation guides for infection prevention from the Association for Professionals in Infection Control and Epidemiology (APIC):
This revised guide contains strategies for prevention, considerations for specific patient populations, evolving practices, and how to incorporate current regulations.
Topics include:
• C. difficile in pediatrics and skilled nursing facilities
• pathogenesis and changing epidemiology of C. difficile infection diagnosis
• environmental control
• new and emerging technologies
• tools and examples to help apply preventative measures, such as hand hygiene monitoring, environmental cleaning, and isolation compliance.
This guide includes infection-prevention standards, regulations, and best practices, as well as instructions, examples, and tools to conduct surveillance and risk assessments.
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT
Every year, 1.9% of patients with diabetes develop foot ulcers. Of those, 15% to 20% undergo an amputation within 5 years of ulcer onset. During their lifetimes, an estimated 25% of diabetic patients develop a foot ulcer. This article discusses use of hyperbaric oxygen therapy (HBOT) in treating diabetic foot ulcers, presenting several case studies.
HBOT involves intermittent administration of 100% oxygen inhaled at a pressure greater than sea level. It may be given in a:
• multi-place chamber (used to treat multiple patients at the same time), compressed to depth by air as the patient breathes 100% oxygen through a face mask or hood (more…)
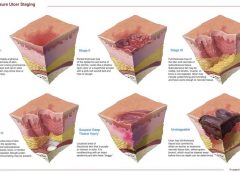
NPUAP releases new position statement on exposed cartilage as Stage IV ulcer
The National Pressure Ulcer Advisory Panel (NPUAP) has released a new position statement, “Pressure ulcers with exposed cartilage are Stage IV pressure ulcers,” which states that pressure ulcers with exposed cartilage should be classified as Stage IV.
NPUAP notes that although the presence of “visible or palpable cartilage at the base of a pressure ulcer” wasn’t included in Stage IV terminology, cartilage “serves the same anatomical function as bone,” so it fits into the current Stage IV definition, “Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often including undermining and tunneling.”
Medicare expenditures for diabetic foot care varies significantly by region
Medicare spending on patients with diabetes who have foot ulcers and lower extremity amputations varies significantly by region, according to a study in Journal of Diabetes and Its Complications, but more spending doesn’t significantly reduce 1-year mortality.
“Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations” examined data from 682,887 patients with foot ulcers and 151,752 patients with lower extremity amputations.
Macrovascular complications in patients with foot ulcers were associated with higher spending, and these complications in patients with amputations were more common in regions with higher mortality rates.
Rates of hospital admission were associated with higher spending and increased mortality rates for patients with foot ulcers and amputations.
“Geographic variation in Medicare spending and mortality rates for diabetic patients with foot ulcers and amputations is associated with regional differences in the utilization of inpatient services and the prevalence of macrovascular complications,” the study concludes.
Patients who develop pressure ulcers in hospital more likely to die
Medicare patients who develop pressure ulcers in the hospital are more likely to die during the hospital stay, have longer lengths of stay, and to be readmitted within 30 days after discharge, according to a study of 51,842 patients in the Journal of the American Geriatrics Society.
“Hospital-acquired pressure ulcers: results from the National Medicare Patient Safety Monitoring System Study” found that 4.5% of patients developed at least one new pressure ulcer during their hospitalization. Length of stay averaged 4.8 days for patients who didn’t develop a pressure ulcer, compared to 11.2 days for those with a new pressure ulcer.
Patients with diabetic foot ulcers may have higher risk of death
Patients with diabetes who have foot ulcers have a higher risk of cardiovascular disease and mortality, according to a meta-analysis in Diabetologia.
“The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis” notes that the more frequent occurrence of cardiovascular disease only partly explains the increased mortality rate. Other explanations may include the more advanced stage of diabetes associated with those who had foot ulcers.
A Drugs.com article about the study reported that “analysis of data from more than 17,000 diabetes patients in eight studies found that the more than 3,000 patients with a history of foot ulcers had an extra 58 deaths per 1,000 people each year than those without foot ulcers.”
The study authors emphasize the importance of screening patients with diabetes for foot ulcers so intervention can begin early, as well as lowering cardiovascular risk factors.
Access patient information on foot care from the American Diabetes Association.
Nurse’s innovation for ostomy patients could improve quality of life
An oncology nurse in Australia has developed StomaLife, an alternative to ostomy bags.
StomaLife is a ceramic appliance that eliminates the need for an ostomy bag. According to the StomaLife website, the appliance uses a magnetic implant technology that provides a “pushing force” from within the body outward in order to keep the site intact, while a second part is placed on the stoma site. A cotton gauze pad is used between the skin and the appliance to keep the site separated and to provide air circulation to the surrounding skin.
“The benefits of StomaLife to ostomy patients are continence all day, reduced skin irritation and infection, odour and sound control, leak prevention, waste material flow control and on-demand gas release,” says Saied Sabeti.
StomaLife still needs to be tested and is not yet being produced.
New laser-activated bio-adhesive polymer aims to replace sutures
The Journal of Visualized Experiments, a peer-reviewed video journal, has published “A chitosan based, laser activated thin film surgical adhesive, ‘SurgiLux’: preparation and demonstration.”
SurgiLux is a laser-activated, bio-adhesive polymer that is chitosan-based. Chitosan is a polymer derived from chitin, which is found in fungal cell walls or in exoskeletons of crustaceans and insects. This molecular component allows SurgiLux to form low-energy bonds between the polymer and the desired tissue when it absorbs light.
The technology may be able to replace traditional sutures in the clinical setting. SurgiLux polymer can achieve a uniform seal when activated by a laser and has antimicrobial properties, which help prevent a wound from becoming infected. It also maintains a barrier between the tissue and its surroundings.
SurgiLux has been tested both in vitro and in vivo on a variety of tissues, including nerve, intestine, dura mater, and cornea.
Palliative care raises patient satisfaction and reduces costs
Kaiser Permanente’s home-based palliative care program increased patient satisfaction and decreased emergency department visits, inpatient admissions, and costs, according to an innovation profile in the Agency for Healthcare Research and Quality’s Innovations Exchange.
“In-home palliative care allows more patients to die at home, leading to higher satisfaction and lower acute care utilization and costs” notes that the program uses an interdisciplinary team of providers to manage symptoms and pain, provide emotional and spiritual support, and educate patients and family members on an ongoing basis about changes in the patient’s condition.
Other components of the program include a 24-hour nurse call center, biweekly team meetings, and bereavement services to the family after the patient dies.
More research needed to determine efficacy of maggot debridement therapy
“The efficacy of maggot debridement therapy (MDT)—a review of comparative clinical trials” concludes that “poor quality of the data used for evaluating the efficacy of MDT highlights the need for more and better designed investigations.”
The authors of the article in International Wound Journal reviewed three randomized clinical trials and five nonrandomized clinical trials evaluating the efficacy of sterile Lucilia sericata applied on ulcers.
The studies found that MDT was “significantly more effective than hydrogel or a mixture of conventional therapy modalities, including hydrocolloid, hydrogel and saline moistened gauze,” but the designs of the study were “suboptimal.”
Use tool to select correct antimicrobial dressing
“Ensuring that the correct antimicrobial dressing is selected,” in Wounds International, emphasizes that dressing selection should be based on assessment of the microbial burden in the wound, the wound type, and the location and condition of the wound.
The article includes a checklist that may be helpful for deciding on the level of bacterial burden in a wound. The checklist is used to determine four levels of risk—colonized: at risk; localized infection; spreading infection; and systemic infection. Each level has a corresponding definition.
A table of antimicrobial dressings reviews the antimicrobial agent and dressing form, and the article ends with a case study.
Editor’s note: Part 1 of this series, published in the September-October issue, discussed lymphedema pathology and diagnosis. This article, Part 2, covers treatment.
Traditional treatment approaches
Traditionally, lymphedema treatment has been approached without a clear understanding of the underlying structure and function of lymphatic tissues. Ineffective traditional treatments include elevation, elastic garments, pneumatic pumps, surgery, diuretics, and benzopyrones (such as warfarin). Because many traditional treatments are still overused and some may be appropriate for limited use, it’s important for clinicians to understand these approaches.
Elevation
As a sole therapy for lymphedema, elevation of the affected part provides only short-lived results. Ever-increasing macromolecular wastes retain water against the effects of gravity. Increased interstitial colloid osmotic pressure must be addressed by interventions targeted at improving lymphatic function—not just a position change. Otherwise, lymphedema will progress. Furthermore, elevation alone is impractical, promotes deconditioning, and alters lifestyle for prolonged periods.
Elastic garments
Elastic garments prove inadequate because they attempt to treat lymphedema with compression alone. Medically correct garments are engineered with thoughtful attention to high-quality textiles and offer gradient support, which promotes proximal flow. However, without precise tissue stimulation leading to improved lymphangioactivity (lymph-vessel pulsation), macromolecular wastes can’t be removed.
Interstitial pressure increases caused by compression garments impede further fluid accumulation. When these garments are removed, the spontaneous girth increase causes an imprecise fit, and the garment rapidly leads to a countertherapeutic effect. Furthermore, compression garments don’t combat the osmotic forces generated by ever-increasing interstitial wastes. Except in patients diagnosed with stage 0 or stage 1 lymphedema, disease progression involving metaplasia ensues. Although elastic compression garments are a cornerstone of long-term management, they shouldn’t be used as a stand-alone treatment.
Pneumatic compression pump
Formerly, the pneumatic compression pump (PCP) was considered the standard of care for lymphedema. However, when inflated, the pump doesn’t increase the frequency of lymph-vessel contraction or enhance lymph capillary absorption. What’s more, accelerated fibrosis development and rapid tissue refilling occur when a PCP is removed. Also, PCP use disregards the ipsilateral territory of the excised regional nodes, effectively dumping fluid from the leg into the trunk. A PCP is appropriate only when nothing else is available, as it may worsen the patient’s condition.
Surgery
Surgical approaches to treating lymphedema involve either excisional (debulking) or microsurgical techniques. The most extensive surgical technique, the radical Charles procedure, completely debulks all involved tissue down to the muscle fascia. Split-thickness grafts are then harvested from excised skin and donor sites, and applied to the fascia to achieve so-called limb reduction.
Most debulking procedures have been applied to lower-extremity lymphedema and offer poor cosmetic results. Less radical surgeries favor long incisions, preserving the skin but excising subcutaneous edematous portions to reduce girth. Although less cosmetically alarming, these procedures effectively amputate the subcutaneous space where lymph vessels reside. Other surgical approaches are beyond the scope of this article.
Generally, surgery isn’t a good approach for any patient, as it’s linked to significant morbidity, such as skin necrosis, infection, and sensory changes. In the future, less invasive procedures may be available that yield significant improvement without these adverse effects.
Diuretics
Although diuretics are prescribed appropriately to address water-rich edemas of venous origin, they disregard the fact that lymphedema is a protein-rich edema. Long-term, high-dose diuretic therapy leads to treatment-resistant limbs, similar to those that have received intensive pneumatic compression.
Benzopyrones
Benzopyrones such as warfarin decrease swelling by combating protein accumulation in fluid. Such drugs have undergone clinical trials abroad. Their mechanism is to promote macrophage migration into interstitial fluid, as well as subsequent proteolysis. Due to significant risk of liver damage or failure, benzopyrones haven’t been approved for treating lymphedema.
Complete decongestive therapy: The current treatment approach
Currently, the gold standard for lymphedema treatment is complete decongestive therapy (CDT). Michael Foeldi and Etelka Foeldi, who originated this method, discovered a unique symbiotic relationship among five distinct modalities that addresses the challenges of lymphedema treatment. In 1989, CDT was brought to the United States by Robert Lerner and has become the mainstay of lymphedema treatment here.
CDT is a two-phase approach involving an intensive clinical effort followed by a semi-intensive home-care program geared toward autonomous management, stabilization, and continual improvement. It involves manual lymph drainage (MLD), compression bandaging, exercise, skin and nail hygiene, and self-care education. (See Phases of complete decongestive therapy by clicking the PDF icon above.)
Manual lymph drainage
A type of soft-tissue mobilization, MLD provides skin traction, stimulating superficial lymph vessels and nodes. Lymph capillaries contain large inter-endothelial inlets called swinging tips, akin to overlapping shingles. Each overlapping cell is tethered to the interstitial matrix by anchoring filaments, so that fluid increases cause immediate distention and lymph inflow. Manual skin traction using MLD promotes greater lymph fluid uptake by stretching these filamentous structures, opening the swinging tips.
MLD also provides extrinsic stimulation of the lymphangion (the segment of a lymph vessel between a distal and proximal valve), drawing fluid into the system at the capillary level and promoting flow at the vessel level toward regional lymph nodes. Usually, these segments contract and relax in a rhythmic fashion six times per minute. MLD triples this output to 18 or 20 times per minute, greatly enhancing systemic transport.
MLD requires intensive daily treatment sessions to strengthen collateral flow as a pathway to circumventing surgical or developmental lymphatic disruption. Treatment strategies further recruit more deeply situated lymphatics such as the thoracic duct, as well as lumbar trunks that empty at the juncture of the internal jugular and subclavian veins to improve global uptake. MLD thus stimulates deeper vessel angioactivity to help drain the superficial vessels that drain toward them.
Compression bandaging
Compression bandaging provides tissue support after MLD to prevent reflux, slow new fluid formation, and mechanically soften fibrotic areas. Bandaging techniques provide a high working pressure to harness the muscle and joint pumps as a propellant for lymph while resisting retrograde flow created by gravity and centrifugal forces during movement. Pure cotton materials coupled with specialized padding create a soft, castlike environment, which confines swollen tissues without constriction. By relying on high working pressure and low resting pressures to decrease limb swelling, this strategy achieves greater control over intensity (level of compression/pressure exerted), with little to no soft-tissue injury or discomfort.
The patient wears this bulky inelastic complex after each MLD treatment until the next day’s session to ensure limb-volume reduction in a stable, linear fashion. Once a plateau is reached, tissue stabilization and self-care education are the goals of additional sessions.
Exercise
Exercise always must be done with adequate support to counteract fluid formation. During the intensive CDT phase, limbs are bandaged to provide complete around-the-clock containment. Gentle exercises encourage blood flow into the muscle; during muscle contraction, this creates a favorable internal pressure that effectively squeezes the subcutaneous space between the bandage wall and muscle. Because every bandage strives to provide a gradient of support, fluid tends to drain proximally to the bandage—in most cases, to the trunk.
Skin and nail hygiene
Without intact, well-hydrated skin, cellulitic infections occur in many lymphedema patients whose immune response has been diminished by regional lymphadenectomy or inherited deficiencies. To prevent infection caused by avoidable external events, patients receive clear guidelines to reinforce appropriate behavior. As most cellulitis results from resident skin pathogens (streptococci and staphylococci), maintaining a low skin pH helps control colonization. Ways to avoid recurrent infections include maintaining an acid mantle on the skin using low-pH-formulated lotions and avoiding injury from daily tasks that may scratch, puncture, burn, or abrade the skin. Patients should receive lists of self-care precautions at the time of treatment.
Self-care education
Because lymphedema is a chronic condition, patients must receive self-care education for daily management to avoid lymphedema destabilization, which can lead to tissue saturation and subsequent skin changes. Therapists must provide patients with appropriate self-care tools and knowledge to maintain adequate treatment results. Teaching topics include how to apply and remove compression garments and bandages and how to exercise safely, preserve skin integrity, monitor for infection, and respond appropriately to infection and significant changes in limb mobility.
An underrecognized and mistreated problem
Lymphedema remains an underrecognized and mistreated condition, even though CDT yields safe, reliable results. Early detection, accurate staging, proper diagnosis, and appropriate treatment can slow the inevitable progression of lymphedema. Wound care specialists should adapt wound therapy to address not just the wound but the edematous environment responsible for delayed wound resolution.
Selected references
Al-Niaimi F, Cox N. Cellulitis and lymphedema: a vicious cycle. J Lymphoedema. 2009;4:38-42.
Browse N, Burnand KG, Mortimer PS. Diseases of the Lymphatics. London: Hodder Arnold; 2003.
Casley-Smith JR, Casley-Smith JR. Modern Treatment for Lymphoedema. 5th ed. The Lymphoedema Association of Australia; 1997.
Cooper R, White R. Cutaneous infections in lymphoedema. J Lymphoedema. 2009:4:44-8.
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. Consensus Document of the International Society of Lymphology. Lymphology. 2009 Jun;42(2):51-60.
Leduc A, Bastin R, Bourgeois P. Lymphatic reabsorption of proteins and pressotherapies. Progress in Lymphology XI. 1988:591-2.
National Lymphedema Network Medical Advisory Committee. Position Statement: Lymphedema Risk Reduction Practices. Revised May 2012. http://www.lymphnet.org/pdfDocs/nlnriskreduction.pdf. Accessed September 5, 2012.
Pappas CJ, O’Donnell TF Jr. Long-term results of compression treatment for lymphedema. J Vasc Surg. 1992 Oct;16(4):555-62.
Whittlinger H. Textbook of Dr. Vodder’s Manual Lymphatic Drainage. Vol 1. 7th ed. New York, NY: Thieme; 2003.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Staphylococcus aureus is one of the most feared human pathogens, causing a wide range of infections. Most wound care professionals can expect to frequently encounter patients with S. aureus infections. Soft-tissue infections caused by S. aureus include impetigo, cellulitis, and cutaneous abscesses, as well as such life-threatening processes as necrotizing fasciitis and pyomyositis (a hematogenous intramuscular abscess). Serious non-soft-tissue infections include septic arthritis, osteomyelitis, pneumonia, endocarditis, and sepsis.
Why is S. aureus such a nasty bug?
S. aureus produces various cellular and extracellular factors involved in the pathogenesis of infection. S. aureus protein A, an important surface protein, helps the organism resist phagocytosis. Also, S. aureus produces several cytotoxins and enzymes that contribute to infection spread and severity. In addition, some strains produce toxins (including toxic shock syndrome toxin-1) that function as superantigens—molecules that nonspecifically trigger release of large amounts of cytokines, leading to a sepsislike condition. Taken together, such factors combine to make S. aureus a dangerous pathogen.
MRSA emergence
When penicillin was introduced in the 1940s, virtually all S. aureus isolates were sensitive to that drug. But soon thereafter, S. aureus strains that produced a β-lactamase enzyme capable of inactivating penicillin became widespread. During the 1950s, outbreaks of penicillin-resistant S. aureus occurred in many U.S. hospitals. Introduction of penicillinase-resistant antibiotics, such as methicillin and oxacillin, temporarily restored the ability to treat all strains of this pathogen using penicillin antibiotics. The first strain of methicillin-resistant S. aureus (MRSA) was described in 1961 shortly after introduction of penicillinase-resistant antibiotics.
The mechanism of methicillin resistance involves a mutation in one of the bacterial cell-wall proteins to which penicillins must bind to kill the bacterium. This mutation renders the organism resistant to all penicillins and penems and almost all cephalosporins.
MRSA incidence has increased steadily to the point where it currently constitutes up to 60% of S. aureus isolates in many U.S. hospitals. These organisms commonly carry genetic material that makes them resistant to various non-β lactam antibiotics as well, leading some to suggest that the term MRSA should stand for multiply resistant S. aureus. S. aureus has continued to mutate in the face of persistent antibiotic pressure. Vancomycin-intermediate S. aureus (VISA) was described in 1997; vancomycin-resistant S. aureus (VRSA), in 2003. Fortunately, these two strains remain rare and haven’t become established pathogens. (See Strains of antibiotic-resistantS. aureus by clicking the PDF icon above.)
Healthcare- versus community-acquired MRSA
Although MRSA initially arose and spread within healthcare settings (chiefly acute-care hospitals), a community-based variant was described in 1998. Called community-
acquired MRSA (CA-MRSA), this variant differs from healthcare-associated MRSA (HCA-MRSA) in more ways than the acquisition site. CA-MRSA occurs predominately in otherwise healthy children and young adults.
It most commonly presents as recurrent cutaneous abscesses, although life-threatening infections (such as necrotizing fasciitis and pneumonia) also have occurred. The propensity to cause cutaneous abscesses isn’t fully understood but may relate partly to production of the Panton-Valentine toxin by many CA-MRSA isolates.
In contrast, HCA-MRSA afflicts mainly older patients, particularly those with chronic illnesses, including chronic wounds. It typically causes wound infections, urinary tract infections, pneumonia, and bacteremia.
Besides these epidemiologic and clinical differences, many CA-MRSA isolates derive from a single clone, known as clone USA 300, whereas HCA-MRSA is composed of multiple non-USA 300 clones. Finally, many CA-MRSA isolates are sensitive to non-β
lactam antibiotics, whereas most HCA-MRSA isolates resist multiple antibiotics. More recently, the distinction between CA-MRSA and HCA-MRSA has been blurred as evidence emerges that CA-MRSA now is being transmitted in healthcare settings as well as in the community.
S. aureus carrier state
Staphylococci are frequent colonizers of humans. Common colonization sites include the skin, anterior nares, axillae, and inguinal regions. Individuals can be colonized continuously or transiently, with nasal carriage rates varying from 20% to 40%. Most S. aureus infections result from the strain carried by the infected patient.
Three patterns of S. aureus carriage exist in humans:
• 20% of individuals are continuously colonized.
• 30% of individuals are intermittently colonized.
• 50% of individuals are never colonized.
The highest carriage rates occur in patients receiving frequent injections (such as insulin-dependent diabetics, hemodialysis patients, and I.V. drug users) and those with chronic skin conditions (for instance, psoriasis or eczema). In the general population, MRSA carriage rates have increased to 1% or 2%, with clinical consequences hinging on the colonizing strain (CA-MRSA versus HCA-MRSA) and host characteristics. The most consistent carriage site is the anterior nares, but many other sites may carry this pathogen, including the axillae, inguinal regions, and perirectal area.
MRSA treatment
Therapy for MRSA infection depends on the infection location and antibiotic sensitivity of the infecting strain.
• Cutaneous abscesses are treated by incision and drainage; antibiotics play a secondary role to adequate drainage.
• Therapy for necrotizing fasciitis caused by MRSA involves aggressive debridement with removal of all necrotic tissue, plus adequate antibiotic therapy. Typically, patients require serial debridement followed by subsequent careful wound care, often with eventual skin grafting.
• Pyomyositis treatment entails drainage of the muscle abscess (which sometimes can be done with percutaneous tube placement instead of open drainage), plus appropriate antibiotic therapy.
Vancomycin has been the mainstay of I.V. therapy for MRSA for decades, but some clinicians are concerned that its effectiveness may be declining due to slowly increasing minimum inhibitory concentrations (the minimum concentration of an
antibiotic needed to inhibit pathogen growth). Other parenteral options have emerged in the last few years. (See I.V. drugs used to treat MRSA by clicking the PDF icon above.) Several oral antibiotics also are available for MRSA treatment. (See Oral agents used to treat MRSA by clicking the PDF icon above.)
Knowing the antibiotic sensitivity pattern of the infecting MRSA strain is crucial to ensuring that the patient receives an appropriate antibiotic. Treatment duration for soft-
tissue infections usually ranges from 7 to 14 days, but bacteremia and bone or joint infections call for more prolonged therapy.
Efforts to eradicate MRSA carriage
Because the carrier state increases the risk of subsequent S. aureus infection, efforts have been made to eradicate carriage. Unfortunately, this has proven to be difficult. A commonly used regimen involves 5 days of twice-daily mupirocin nasal ointment with either chlorhexidine gluconate showers or immersion up to the neck in a dilute bleach solution. However, success in eliminating carriage is limited, although the bleach bath seems to improve eradication rates better than other modalities.
Controlling MRSA in hospitals
How best to control MRSA spread within hospitals is controversial. Some experts advocate an aggressive, “search and destroy” approach involving screening all patients for nasal carriage on admission and initiating contact precautions with subsequent decolonization efforts. Others focus on improving the overall level of hand hygiene and other general infection-control measures, arguing that nasal screening misses at least 20% of MRSA-colonized patients and thus gives an unwarranted sense of security.
Many hospitals use a mixed approach, screening patients suspected to be at high risk for MRSA carriage (such as those admitted from extended-care facilities or to the intensive care unit), while simultaneously trying to improve hand hygiene and general infection-control measures. Recent data suggest MRSA colonization and infection rates have stopped increasing and are beginning to decline.
MRSA is one of the most problematic pathogens encountered on a regular basis, and among the most dangerous pathogens we face. While some MRSA infections are relatively mild, many are serious or life-threatening. Severe soft-tissue infections, such as necrotizing fasciitis and pyomyositis, require surgical debridement or drainage, appropriate antibiotic therapy, and assistance from a wound-care professional to achieve optimal outcomes. n
Selected references
Calfee DP. The epidemiology, treatment and prevention of transmission of methicillin-resistant Staphylococcus aureus. J Infus Nurs. 2011 Nov-Dec;34(6):359-64.
DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010 May 1;375(9725): 1557-68.
Ippolito G, Leone S, Lauria FN, et al. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010 Oct;14 Suppl 4:S7-11.
Landrum ML, Neumann C, Cook C, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010. JAMA. July 4;308:50-9.
Lee AS, Huttner B, Harbarth S. Control of methicillin-resistant Staphylococcus aureus. Infect Dis Clin North Am. 2011 Mar;25(1):155-79.
Moellering RC Jr. MRSA: the first half century. J Antimicrob Chemother. 2012 Jan;67(1):4-11.
Otter JA, French GL. Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection. J Hosp Infect. 2011 Nov:79(3):189-93.
Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant pneumococci, and vancomycin-resistant enterococci. Mayo Clin Proc. 2011 Dec;86(12):1230-43.
Simor AE. Staphylococcal decolonization: an effective strategy for prevention of infection? Lancet Infect Dis. 2011 Dec;11(12):952-62.
Joseph G. Garner is director of the infectious disease division and hospital epidemiologist at the Hospital of Central Connecticut and a professor of medicine at the University of Connecticut.