About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders.
A stoma has no sensory nerve endings and is insensitive to pain. Yet several complications can affect it, making accurate assessment crucial. These complications may occur during the immediate postoperative period, within 30 days after surgery, or later. Lifelong assessment by a healthcare provider with knowledge of ostomy surgeries and complications is important.
Critical limb ischemia may not increase mortality risk in patients with diabetes Diabetic patients with critical limb ischemia (CLI) who are assessed quickly and treated aggressively do not have an increased risk of long-term cardiac mortality, according to a study in Diabetes Care.
By Nancy Chatham, RN, MSN, ANP-BC, CCNS, CWOCN, CWS, and Lori Thomas, MS, OTR/L, CLT-LANA An estimated 7 million people in the United States have venous disease, which can cause leg edema and ulcers. Approximately 2 to 3 million Americans suffer from secondary lymphedema. Marked by abnormal accumulation of protein-rich fluid in the interstitium, secondary lymphedema eventually can cause fibrosis…
By T. Michael Britton, RN, NHA, WCC, DWC As wound care professionals, we’ve all experienced a time when we felt that our patient didn’t have the appropriate wound treatment orders. However, the physician, nurse practitioner, or other prescriber wouldn’t follow your recommendation. This situation is not only frustrating but can delay the healing process. This article explores why a prescriber…
by Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS What an honor it is to be the wound care “superhero”—the guru, the healer, the go-to person. Unfortunately, this honor may be accompanied by wound care overload—too much to do in too little time. Once someone is crowned the superhero specialist, others may try to transfer every aspect of wound and…
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders. A stoma has no sensory nerve endings and…
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA The ability to understand or “read” lower-extremity redness in your patient is essential to determining its cause and providing effective treatment. Redness can occur in multiple conditions—hemosiderin staining, lipodermatosclerosis, venous dermatitis, chronic inflammation, cellulitis, and dependent rubor. This article provides clues to help you differentiate these conditions and identify the specific cause of…
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Knowledge is exploding online, making it essential that you’re comfortable using the Internet. You can also go online to save time and find a job, among other tasks. (See Online value.) However, you also need to keep in mind that anyone can put information on the Internet. As the caption of…
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found that using hybrid 67Ga single-photon emission computed tomography and X-ray computed tomography (SPECT/CT) imaging combined with a bedside percutaneous bone puncture in patients with a positive scan is “accurate and safe” for diagnosing osteomyelitis in patients with diabetes who have a foot ulcer without signs of soft-tissue infection.
The new method, which avoids an invasive bone biopsy, has a sensitivity of 88% and a specificity of 93.6%. In the study of 55 patients, antibiotic treatment was avoided in 55% of suspected cases.
MRSA strains will likely continue to coexist in hospitals and communities
The strains of methicillin-resistant Staphylococcus aureus (MRSA) differ in the hospital and community settings, and both are likely to coexist in the future, according to a study in PLOS Pathogens.
C. difficile prevention actions fail to stop spread
Despite increasing activities to prevent the spread of Clostridium difficile, infection from C. difficile remains a problem in healthcare facilities, according to a survey of infection preventionists by the Association for Professionals in Infection Control and Epidemiology (APIC).
The survey found that 70% of preventionists have adopted additional interventions in their healthcare facilities since March 2010, but only 42% have seen a decline in C. difficile infection rates; 43% saw no decline.
A total of 1,087 APIC members completed the survey in January 2013. The survey also found that more than 92% of respondents have increased emphasis on environmental cleaning and equipment decontamination practices, but 64% said they rely on observation, rather than more accurate and reliable monitoring technologies, to assess cleaning effectiveness.
In addition, 60% of respondents have antimicrobial stewardship programs at their facilities, compared with 52% in 2010. Such programs promote the appropriate use of antibiotics, which can help reduce the risk of C. difficile infection.
Mast cells may not play significant role in wound healing
“Evidence that mast cells are not required for healing of splinted cutaneous excisional wounds in mice,” published in PLOS One, analyzed wound healing in three types of genetically mast-deficient mice and found they reepithelialized their wounds at rates similar to control mice. At the time of closure, the researchers found that scars in all the mice groups were similar in both “quality of collagen deposition and maturity of collagen fibers.” The findings fail to support the previously held belief that mast cells are important in wound healing.
Study identifies effective casting for diabetes-related plantar foot ulcers
Nonremovable casts that relieve pressure are more effective than removable casts or dressings alone for the treatment of plantar foot ulcers caused by diabetes, according to an analysis of clinical trials.
The authors of “Pressure-relieving interventions for treating diabetic foot ulcers,” published by The Cochrane Library, reviewed 14 randomized clinical trials that included 709 participants. Nonremovable pressure-relieving casts were compared to dressings alone, temporary therapeutic shoes, removable pressure-relieving devices, and surgical lengthening of the Achilles tendon.
The study also notes that when combined with Achilles tendon lengthening, nonremovable devices were more successful in one forefoot ulcer study than the use of a nonremovable cast alone.
Most studies were from the United States (five) and Italy (five), with Germany, the Netherlands, Australia, and India each contributing one study.
Prescriber preference drives use of antibiotics in long-term care
The study of 66,901 patients from 630 long-term care facilities found that 77.8%
received a course of antibiotics. The most common length (41%) was 7 days, but the length exceeded 7 days in 44.9% of patients. Patient characteristics were similar among short-, average-, and long-duration prescribers.
The study authors conclude: “Future trials should evaluate antibiotic stewardship interventions targeting prescriber preferences to systematically shorten average treatment durations to reduce the complications, costs, and resistance associated with antibiotic overuse.”
Electrophysical therapy may be helpful for diabetic foot ulcers
The authors of the study in International Wound Journal reviewed eight trials with a combined total of 325 patients. Five studies were on electrical stimulation, two on phototherapy, and one on ultrasound. Because of the small number of trials, the possibility of harmful effects can’t be ruled out, and the authors recommend “high-quality trials with larger sample sizes.”
Significant geographic variations in spending, mortality exist for diabetic patients with foot ulcers and amputations
The study in Journal of Diabetes and Its Complications found that higher spending wasn’t associated with a significant reduction in 1-year patient mortality. In addition, rates of hospital admission were associated with higher per capita spending and higher mortality rates for patients.
Home-based exercise program improves life for lymphedema patients
An individualized, home-based progressive resistance exercise program improves upper-limb volume and circumference and quality of life in postmastectomy patients with lymphedema, according to a study published in the Journal of Rehabilitation Research and Development.
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
The guidelines include recommendations for practice, education, policy, and future resource. Strategies for implementation are given, as well as several useful appendices, such as:
• Debridement Decision-Making Algorithm
• A Guide to Dressing Foot Wounds
• PEDIS: Diabetes Foot Ulcer Classification System
• Offloading Devices
• Optimal Treatment Modalities.
PREPARE is a useful and patient-friendly website designed to help prepare people to make complex medical decisions. The website was developed by clinical researchers from the San Francisco VA Medical Center; the University of California, San Francisco; and NCIRE—The Veterans Health Research Institute.
PREPARE uses videos to provide concrete examples of how to identify what is most important in life; how to communicate that with family, friends, and doctors; and how to make informed medical decisions when the time comes. Users can also download a PDF of a PREPARE pamphlet.
Free guides for infection prevention from APIC
Download two free implementation guides for infection prevention from the Association for Professionals in Infection Control and Epidemiology (APIC):
This revised guide contains strategies for prevention, considerations for specific patient populations, evolving practices, and how to incorporate current regulations.
Topics include:
• C. difficile in pediatrics and skilled nursing facilities
• pathogenesis and changing epidemiology of C. difficile infection diagnosis
• environmental control
• new and emerging technologies
• tools and examples to help apply preventative measures, such as hand hygiene monitoring, environmental cleaning, and isolation compliance.
This guide includes infection-prevention standards, regulations, and best practices, as well as instructions, examples, and tools to conduct surveillance and risk assessments.
One of the worst fears of a wound care clinician is inadvertently compressing a leg with critical limb ischemia—a condition marked by barely enough blood flow to sustain tissue life. Compression (as well as infection or injury) could lead to necrosis, the need for amputation, or even death. The gold standard of practice is to obtain an ankle-brachial index (ABI) before applying compression. However, recent research and expert opinion indicate an elevated or normal ABI is deceptive in patients with advanced diabetes. What’s worse, in the diabetic foot, skin may die from chronic capillary ischemia even when total blood perfusion is normal. For information on how to perform an ABI and interpret results, click on this link. (more…)
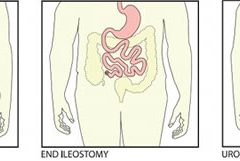
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Here are resources that can help you in your busy clinical practice by giving you information quickly.
Pressure ulcer resources
Instead of searching through Google or another search engine for pressure ulcer resources, start with this comprehensive list on the Centers for Medicare & Medicaid Services website.
Examples of resources included are:
“Preventing pressure ulcers in hospitals: A toolkit for improving quality of care.” This toolkit from the Agency for Healthcare Research and Quality (AHRQ) is designed to help hospitals in implementing pressure ulcer prevention strategies.
“On-time pressure ulcer healing project.” Another AHRQ initiative, this resource is designed for those working in long-term care facilities.
“Pressure ulcer prevention.” This table from the Institute for Healthcare Improvement lists possible mentors you can work with in the area of ulcer prevention.
“Shawnee Medical Center wound care quick reference guide.” This is a handy one-page reference guide that includes photographs and recommendations.
“How-to guide: Prevent pressure ulcers—pediatric supplement.” This guide, tailored for pediatrics, describes key evidence-based care components for preventing pressure ulcers and describes how to implement these interventions.
You can also access case studies from a variety of facilities around the United States.
The National Lymphedema Network is a nonprofit organization founded in 1988 to provide education and other information to healthcare professionals and patients with lymphedema, as well as the general public. The site includes an explanation of lymphedema that may be helpful for you to use in teaching your patients. It also includes access to some of the articles from the newsletter LymphLink.
Many patients with chronic wounds have diabetes. To ensure those patients receive the best possible care, you can refer to the 2013 Standards of Medical Care in Diabetes from the American Diabetes Association, which were published in the January issue of Diabetes Care.
The journal provides a summary of the revisions and an executive summary of the standards related to each area, including diagnosis, testing, prevention, monitoring, and pharmacologic and nonpharmacologic management.
The guidelines include valuable information related to neuropathy screening and treatment and foot care. Recommendations for foot care include performing an annual comprehensive foot examination to identify risk factors predictive of ulcers and amputations. The foot examination should include inspection, assessment of foot pulses, and testing for loss of protective sensation.
An Unna boot is a special dressing of inelastic gauze impregnated with zinc, glycerin, or calamine that becomes rigid when it dries. It is used for managing venous leg ulcers and lymphedema in patients who are ambulatory. When the patient walks, the rigid dressing restricts outward movement of the calf muscle, which directs the contraction force inward and improves the calf-muscle pumping action, thereby improving venous flow. An Unna boot does not provide compression and is contraindicated for arterial insufficiency. (more…)
If you’re keeping up on wound care, you know a lot of new things are coming to market with enough decent science behind them to make them reasonable options to consider in your practice. And as true-blooded Americans and citizens of the post-industrialized world, we want what’s newest, fastest, and best in class in everything. It’s just our nature.
But does it truly serve us to be eager to try new therapies even when the current treatment plan is successful? Perhaps. We know we must never close our eyes to new developments in our field that can lead to better outcomes. Knowing when and what to change can lead to better outcomes for the patient, the wound, and our collective pocketbook.
I’ve long maintained we can achieve excellent-quality wound care if we just stick to the basics the vast majority of the time. Why? Systemic, psychosocial, and local factors all affect wound healing—not just the dressing or cream. Our job is to provide the optimum environment possible for wound healing. That requires us to look at and support the whole body toward optimum health, not solely the wound.
The basics begin with identifying the cause of the wound and implementing interventions to reduce, control, or eliminate the cause. Next, we strive to manage local and psychosocial factors by choosing topical products that will maintain moisture balance, keep the wound warm, and protect it. If the wound doesn’t show progress toward healing within 2 weeks (or as expected, given the patient’s overall condition and ability to heal), we need to reevaluate the plan and begin making changes.
The best rule is to make one change at a time. That makes it much easier to determine what’s working and what isn’t. Once all the basics are in place and required changes have been made, if healing is still stalled or nonexistent, consider trying the available new products and specialty products.
Never close your clinical mind to advances in the field. To do that would be a disservice to your patients. But you should change the treatment plan only when a change is needed—not just for the sake of changing it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois