Having patients view photographs of their wounds can motivate them to become more involved in managing those wounds, according to a study in International Wound Journal, particularly when wounds are in difficult-to-see locations. (more…)
Changes in healthcare policy and reimbursement are pushing treatment from the hospital to the community. This shift is likely to result in a higher number of complex wounds being treated in the home, which can create stress for patients and families. Education plays a key role in reducing this stress. This article focuses on education for family members or friends who are caregivers for the patient. (more…)
Each issue, Apple Bites brings you a tool you can apply in your daily practice.
Transparent film dressings are thin sheets of transparent polyurethane (polymer) coated with an adhesive. These dressings are available in a variety of sizes and shapes. (more…)
Since its introduction almost 20 years ago, negative-pressure wound therapy (NPWT) has become a leading technology in the care and management of acute, chronic, dehisced, traumatic wounds; pressure ulcers; diabetic ulcers; orthopedic trauma; skin flaps; and grafts. NPWT applies controlled suction to a wound using a suction pump that delivers intermittent, continuous, or variable negative pressure evenly through a wound filler (foam or gauze). Drainage tubing adheres to an occlusive transparent dressing; drainage is removed through the tubing into a collection canister. NWPT increases local vascularity and oxygenation of the wound bed and reduces edema by removing wound fluid, exudate, and bacteria. (more…)
Each issue, Apple Bites brings you a tool you can apply in your daily practice.
Exudate (drainage), a liquid produced by the body in response to tissue damage, is present in wounds as they heal. It consists of fluid that has leaked out of blood vessels and closely resembles blood plasma. Exudate can result also from conditions that cause edema, such as inflammation, immobility, limb dependence, and venous and lymphatic insufficiency. (more…)
Venous disease, which encompasses all conditions caused by or related to diseased or abnormal veins, affects about 15% of adults. When mild, it rarely poses a problem, but as it worsens, it can become crippling and chronic.
Chronic venous disease often is overlooked by primary and cardiovascular care providers, who underestimate its magnitude and impact. Chronic venous insufficiency (CVI) causes hypertension in the venous system of the legs, leading to various pathologies that involve pain, swelling, edema, skin changes, stasis dermatitis, and ulcers. An estimated 1% of the U.S. population suffers from venous stasis ulcers (VSUs). Causes of VSUs include inflammatory processes resulting in leukocyte activation, endothelial damage, platelet aggregation, and intracellular edema. Preventing VSUs is the most important aspect of CVI management. (more…)
Each issue, Apple Bites brings you a tool you can apply in your daily practice.
Description
Hydrated polymer (hydrogel) dressings, originally developed in the 1950s, contain 90% water in a gel base, which helps regulate fluid exchange from the wound surface. Hydrogel dressing are usually clear or translucent and vary in viscosity or thickness. They’re available in three forms: (more…)
Collagen, the protein that gives the skin its tensile strength, plays a key role
in each phase of wound healing. It attracts cells, such as fibroblasts and keratinocytes, to the wound, which encourages debridement, angiogenesis, and reepithelialization. In addition, collagen provides a natural scaffold or substrate for new tissue growth. (more…)
Colleen Jackson recently was promoted to a manager position on her unit. At first, she was thrilled with the opportunity to advance her leadership skills, but now she’s having second thoughts. She doesn’t feel confident in her new role and worries how her team views her. She confesses to her manager, “I keep thinking someone will figure out how much I really don’t know and question whether I should’ve been given the position. Sometimes I feel like an imposter. When I mention this to my friends, they tell me to ‘fake it until you make it.’ But I’m not so sure about that!”
Colleen isn’t alone in feeling like an imposter. In imposter syndrome, a person doesn’t feel good enough, is unsure of what she’s doing, and feels she can’t live up to others’ expectations. She may be afraid she’ll be found out as an imposter at any moment. The syndrome is most common among women leaders who feel they don’t deserve the success they’ve achieved despite external evidence of their competence. It’s more likely in perfectionists who constantly compare themselves to others.
Certain situations, such as taking on a new role, can lead to imposter syndrome. For instance, Colleen may think that because she was seen as qualified for her new role, others expect her to immediately have expert knowledge. If, like Colleen, you feel you don’t deserve the career success you’ve had, you may experience deep feelings of inauthenticity and fear you’ll be found out as a fake. (See Inside the imposter syndrome.)
In small doses, feelings of inadequacy may not be a bad thing, because they remind us to work on building our competency. But people with imposter syndrome feel a level of self-doubt that can lead to overwork and a paralyzing fear of failure. The fear of being unmasked causes incredible stress. Colleen and others like her may have unrealistic expectations of themselves in a new role—expectations that can compromise their success.
Overcoming imposter syndrome
For people with imposter syndrome, the response to their success may rest too heavily on others’ approval, recognition, and opinions. A wise mentor once told me we can easily overestimate how much time others spend thinking about us and our behaviors. Most people, she observed, are self-absorbed. This is important to consider, because the idea that Colleen is an imposter probably has never crossed her team members’ minds.
Imposter syndrome can create performance anxiety and lead to perfectionism, burnout, and depression. So learning how to manage these feelings is important. Cathy Robinson-Walker, MBA, MCC, who coaches nurse leaders, provides advice to help cope with imposter syndrome. Her recommendations include the six actions steps below.
Discuss your feelings with a trusted mentor.
Sharing your insecurities with someone you trust and respect can help you separate what’s real from your perceptions of insecurity. A trusted mentor might inform Colleen she’s making good progress as a beginning leader and that no one expects her to be an expert at this point. The mentor can provide guidance about specific areas where Colleen might need additional growth and how to best go about this.
Pay attention to your own self-talk and consider whether your thoughts are empowering or disabling.
Do you often say to yourself, “I achieved this only because I work harder than anyone else, not because I’m more competent”? Valerie Young, author of The Secret Thoughts of Successful Women: Why Capable People Suffer from the Impostor Syndrome and How to Thrive in Spite of It, makes a strong case that your internal script is a well-rehearsed pattern that serves as a key to feelings of being an imposter. She cautions that individuals with imposter syndrome may sabotage themselves as a way of holding back, due to feelings of being a fraud.
Instead, choose a different script and talk yourself down during times of self-doubt. Instead of thinking, “I’m the wrong person for this job,” retrain yourself to say, “I have a lot to offer in this position.”
Make of list your strengths.
Take the time to make a written list your strengths and what you contribute. Ask others for input, and refer to the list in times of self-doubt. If you’re in a new role, remember that you were chosen for a reason. In Colleen’s case, her supervisor saw her leadership potential. Also realize that most people overestimate their abilities; people with imposter syndrome underestimate theirs.
Accept that perfection is unrealistic and costly.
Trying to be perfect and feeling you need to “know it all” is unrealistic and can be costly on a personal level. Perfectionists typically believe anything short of a flawless performance all the time is unacceptable. But none of us can live a mistake-free life; we all make errors. Those with imposter syndrome hold themselves to impossibly high standards and feel shame, insecurity, and low self-esteem when they don’t meet their own expectations. But progress, not perfection, is what really matters.
Know you’ll need to develop your competencies at certain times in your career.
Throughout your career, you’ll go through periods when you’re on a steep learning curve and will need to further develop your competencies. You may feel like a novice and have to work hard to build new competencies.
Be honest about what you know and don’t know, and seek advice from experts on your unit or in your organization. The simple act of saying, “This is new for me, and I’m working hard to learn this role” can be empowering. Colleen, for instance, might be surprised at others’ reactions to hearing this from her. They might perceive her as a more authentic leader.
Be willing to be uncomfortable and move through your fear.
In Fear of Flying, author Erica Jong urges readers engaging in new experiences to feel the fear and do it anyway. Fear is a useful emotion, as long as it doesn’t escalate to the level of paralyzing behaviors. Practice and preparation can help ease new leaders’ fears. The fear of new challenges will never truly go away, but it can be managed.
Building competence leads to competency
People with imposter syndrome generally are intelligent, thoughtful, and capable but lack self-confidence. Over time, clinicians like Colleen will grow out of feeling like an imposter as they build their competency and become more comfortable in their roles. Eleanor Roosevelt said, “I believe that anyone can conquer fear by doing the things he fears to do, provided he keeps doing them until he gets a record of successful experience behind him.” If you feel like an imposter, this is good advice to ponder.
Selected references
Clance PR, Imes S. The imposter phenomenon in high achieving women: dynamics and therapeutic intervention. Psycho Theor, Res and Prac.1978;15(3):241-7.
Jong E. Fear of Flying. Austin, TX: Holt, Reinhart & Winston; 1973.
Robinson-Walker C. The imposter syndrome. Nurs Leader. 2011;9(4):12-13.
Young V. The Secret Thoughts of Successful Women: Why Capable People Suffer from the Impostor Syndrome and How to Thrive in Spite of It. New York: Crown Business; 2011.
Rose O. Sherman is an associate professor of nursing and director of the Nursing Leadership Institute at the Christine E. Lynn College of Nursing at Florida Atlantic University in Boca Raton. You can read her blog at www.emergingrnleader.com.
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
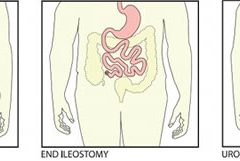
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Chronic venous insufficiency (CVI) is the most common cause of lower extremity wounds. The venous tree is defective, incapable of moving all the blood from the lower extremity back to the heart. This causes pooling of blood and intravascular fluid at the lowest gravitational point of the body—the ankle.
This article has two parts. Part 1 enhances your understanding of the disease and its clinical presentation. Part 2, which will appear in a later issue, explores the differential diagnosis of similar common diseases, the role that coexisting peripheral artery disease (PAD) may play, disease classification of venous insufficiency, and a general approach to therapy.
The most common form of lower extremity vascular disease, CVI affects 6 to 7 million people in the United States. Incidence increases with age and other risk factors. One study of 600 patients with CVI ulcers revealed that 50% had these ulcers for 7 to 9 months, 8% to 34% had them for more than 5 years, and 75% had recurrent ulcers.
Thrombotic complications of CVI include thrombophlebitis, which may range from superficial to extensive. If the thrombophlebitis extends up toward the common femoral vein leaving the leg, proximal ligation may be needed to prevent clot extension or embolization.
Understanding normal anatomy and physiology
Lower extremity veins flow horizontally from the superficial veins to the perforating veins and then into the deep veins. Normally, overall venous blood flows vertically against gravity from the foot and ankle upward toward the inferior vena cava (IVC). This antigravity flow toward the IVC results from muscular contraction around nonobstructed veins and one-way valves that close as blood passes them. These valves prevent abnormal backward blood flow toward the foot and ankle region.
The lower extremities have four types of veins. Superficial veins are located within the subcutaneous tissue between the dermis and muscular fascia. Examples are the greater and lesser (smaller) saphenous veins. Perforating veins connect the superficial veins to the deep veins of the leg. The deep veins are located below the muscular fascia. The communicating veins connect veins within the same system.
The greater saphenous vein is on the leg’s medial (inner) side. It originates from the dorsal veins on top of the foot and eventually drains into the common femoral vein in the groin region. By way of perforating veins, the greater saphenous vein drains into the deep venous system of both the calf and thigh.
The lesser saphenous vein is situated on the lateral (outer) side of the leg and originates from the lateral foot veins. As it ascends, it drains into the deep system at the popliteal vein behind the knee. Communicating veins connect the greater saphenous vein medially and the lesser saphenous vein laterally.
Intramuscular veins are the deep veins within the muscle itself, while the intermuscular veins are located between the muscle groups. The intermuscular veins are more important than other veins in development of chronic venous disease. Below the knee, the intermuscular veins are paired and take on the name of the artery they accompany—for example, paired anterior tibial, paired posterior tibial, and paired peroneal veins. Eventually, these veins form the popliteal vein behind the knee, which ultimately drains into the femoral vein of the groin.
As the common femoral vein travels below the inguinal ligament of the groin, it’s called the external iliac vein. Eventually, it becomes the common iliac vein, which drains directly into the IVC.
Pathophysiology
Abnormally elevated venous pressure stems from the leg’s inability to adequately drain blood from the leg toward the heart. Blood drainage from the leg requires the muscular pumping action of the leg onto the veins, which pump blood from the leg toward the heart as well as from the superficial veins toward the deep veins. Functioning one-way valves within the veins close when blood passes them, preventing blood from flowing backward toward the ankle. This process resembles what happens when you climb a ladder with intact rungs: As you step up from one rung to the next, you’re able to ascend.
CVI and the “broken rung” analogy
If the one-way valves are damaged or incompetent, the “broken rung” situation occurs. Think how hard it would be to climb a ladder with broken rungs: You might be able to ascend the ladder, but probably you would fall downward off the ladder due to the defective, broken rungs.
Normally, one-way valves ensure that blood flows from the lower leg toward the IVC and that the superficial venous system flows toward the deep venous system. The venous system must be patent (open) so blood flowing from the leg can flow upward toward the IVC. Blockage of a vein may result from an acute thrombosis (clot) in the superficial or deep systems. With time, blood may be rerouted around an obstructed vein. If the acute thrombosis involves one or more of the one-way valves, as the obstructing thrombosis opens up within the vein’s lumen, permanent valvular damage may occur, leading to post-thrombotic syndrome—a form of CVI.
CVI may result from an abnormality of any or all of the processes needed to drain blood from the leg—poor pumping action of the leg muscles, damage to the one-way valves, and blockage in the venous system. CVI commonly causes venous hypertension due to reversal of blood flow in the leg. Such abnormal flow may cause one or more of the following local effects:
leg swelling
tissue anoxia, inflammation, or necrosis
subcutaneous fibrosis
Compromised flow of venous blood or lymphatic fluid from the extremity.
“Water balloon” analogy
The effect of elevated venous pressure or hypertension is worst at the lowest gravitational point (around the ankle). Pooling of blood and intravascular fluid around the ankle causes a “water balloon” effect. A balloon inflated with water has a thin, easily traumatized wall. When it bursts, a large volume of fluid drains out. Due to its thicker wall, a collapsed balloon that contains less fluid is more difficult to break than one distended with water.
In a leg with CVI, subcutaneous fluid that builds up requires a weaker force to break the skin and ulcerate than does a nondistended leg with less fluid. This principle is the basis for compression therapy in treating and preventing CVI ulcers.
Effects of elevated venous pressure or hypertension
Increased pressure in the venous system causes:
abnormally high pressure in the superficial veins—60 to 90 mm Hg, compared to the normal pressure of 20 to 30 mm Hg
dilation and distortion of leg veins, because blood refluxes abnormally away from the heart and toward the lower leg and may move from the deep venous system into the superficial veins.
Abnormal vein swelling from elevated pressure in itself may impair an already abnormally functioning one-way valve. For instance, the valve may become more displaced due to the increase in intraluminal fluid, which may in turn worsen hypertension and cause an increase in leg swelling. Increased pressure from swollen veins also may dilate the capillary beds that drain into the veins; this may cause leakage of fluid and red blood cells from capillaries into the interstitial space, exacerbating leg swelling. Also, increased venous pressure may cause fibrinogen to leak from the intravascular plasma into the interstitial space. This leakage may create a fibrin cuff around the capillary bed, which may decrease the amount of oxygen entering the epidermis, increase tissue hypoxia, trigger leukocyte activation, increase capillary permeability, and cause local inflammation. These changes may lead to ulceration, lipodermatosclerosis, or both.
Visible changes may include dilated superficial veins, hemosiderin staining due to blood leakage from the venous tree, atrophie blanche, and lipodermatosclerosis. (See CVI glossary by clicking the PDF icon above.) Both atrophie blanche and lipodermatosclerosis result from local tissue scarring secondary to an inflammatory reaction of the leg distended with fluid.
Lipodermatosclerosis refers to scarring of subcutaneous tissue in severe venous insufficiency. Induration is associated with inflammation, which can cause the skin to bind to the subcutaneous tissue, causing narrowing of leg circumference. Lymphatic flow from the leg also may become compromised and inhibited in severe venous hypertension, causing additional leg swelling.
Patient history
In a patient with known or suspected CVI, a thorough history may lead to a working diagnosis. Be sure to ask the patient these questions:
Do you have pain?
Is your pain worse toward the end of the day?
Is the pain relieved with leg elevation at night?
Is it relieved with leg elevation during the day?
Do you have leg pain that awakens you at night?
How would you describe the pain?
Does the skin on your leg feel tight or irritated?
Have you noticed visible changes of your leg?
Do you have a leg ulcer?
Also determine if the patient has comorbidities that may exacerbate CVI, including PAD, renal failure, venous thrombosis, lymphedema, diabetes mellitus, heart failure, or malnutrition. (See CVI risk factors by clicking the PDF icon above .)
Common CVI symptoms
Approximately 20% of CVI patients have symptoms of the disease without physical findings. These symptoms may include:
tired, “heavy” legs that feel worse toward the end of the day
discomfort that worsens on standing
legs that feel best in the morning after sleeping or after the legs have been
elevated during the day.
Although patients may report leg discomfort, the history indicates that it doesn’t awaken them at night. Be aware that discomfort from CVI differs from that caused by PAD. With PAD, patients may report pain on exercise (claudication), pain with elevation (nocturnal pain), or constant pain (resting pain).
Signs of CVI (with or without ulcers) include:
leg swelling (seen in 25% to 75% of patients)
skin changes (such as hemosiderin staining or dermatitis)
telangiectasia, reticular veins, or both; while these are the most common signs, they represent an overall less severe finding
varicose veins with or without bleeding, occurring in one-third of patients with CVI.
Venous ulcers
Venous ulcers are the most common type of lower extremity ulcer. They’re commonly found on the medial aspect of the lower extremity, from the ankle to the more proximal calf area. Usually, they arise along the course of the greater saphenous vein, but also may be lateral and may occur at multiple locations. They aren’t found above the knee or on the forefoot. Venous ulcers are shallower than arterial ulcers and have considerable exudate consistent with drainage from a ruptured water balloon. They may extend completely around the leg.
CVI: From a heavy sensation to visible changes
In patients with CVI, blood flows within a lower extremity in an abnormal, reverse direction, causing build-up of blood and intravascular fluid around the ankle. Initially, this may cause only a sensation of heavy legs toward the end of the day, with no visible changes. Eventually, it may lead to venous ulcers or other visible changes. This abnormal blood flow results from dysfunction of the normal mechanisms that drain blood from the leg against gravity into the IVC.
Sardina D. Skin and Wound Management Course; Seminar Workbook. Wound Care Education Institute; 2011:92-112.
Donald A. Wollheim is a practicing wound care physician in southeastern Wisconsin. He also is an instructor for Wound Care Education Institute and Madison College. He serves on the Editorial Board for Wound Care Advisor.