By: Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA
Maggot therapy is the controlled, therapeutic application of maggots to a wound. Simple to use, it provides rapid, precise, safe, and powerful debridement. Many wound care professionals don’t provide maggot therapy (also called wound myiasis) because they lack training. But having maggot therapy technology available for patients adds to your capabilities as a wound care provider. (more…)
By Pamela Anderson, MS, RN, APN-BC, CCRN, and Terri Townsend, MA, RN, CCRN-CMC, CVRN-BC
Jan Smith, age 59, is admitted to the coronary intensive care unit with an acute inferior myocardial infarction (MI). Recently diagnosed with hypertension and hyperlipidemia, she smokes a pack and a half of cigarettes daily. She reports she has always been healthy and can’t believe she has had a heart attack. (Note: Name is fictitious.)
On physical exam, the cardiologist finds decreased femoral pulses bilaterally and recommends immediate cardiac catheterization. Fortunately, primary percutaneous coronary intervention (PCI) is readily available at this hospital. PCI is the preferred reperfusion method when it can be provided by skilled cardiologists in a timely manner.(more…)
Venous disease, which encompasses all conditions caused by or related to diseased or abnormal veins, affects about 15% of adults. When mild, it rarely poses a problem, but as it worsens, it can become crippling and chronic.
Chronic venous disease often is overlooked by primary and cardiovascular care providers, who underestimate its magnitude and impact. Chronic venous insufficiency (CVI) causes hypertension in the venous system of the legs, leading to various pathologies that involve pain, swelling, edema, skin changes, stasis dermatitis, and ulcers. An estimated 1% of the U.S. population suffers from venous stasis ulcers (VSUs). Causes of VSUs include inflammatory processes resulting in leukocyte activation, endothelial damage, platelet aggregation, and intracellular edema. Preventing VSUs is the most important aspect of CVI management. (more…)
By Nancy Collins, PhD, RD, LD/N, FAPWCA, and Allison Schnitzer
Nutrition is a critical factor in the wound healing process, with adequate protein intake essential to the successful healing of a wound. Patients with both chronic and acute wounds, such as postsurgical wounds or pressure ulcers, require an increased amount of protein to ensure complete and timely healing of their wounds.
Elderly patients with wounds pose a special challenge because of their decreased lean body mass and the likelihood of chronic illnesses and insufficient dietary protein intake. To promote a full recovery, wound care clinicians must address the increased protein needs of wound patients, especially elderly patients. (more…)
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
Xerosis, an abnormal dryness of the skin, is one of the most common skin conditions among patients with type 2 diabetes. While assessing for predictors of foot lesions in patients with diabetes, the authors of one study found that 82.1% of these patients had skin with dryness, cracks, or fissures. An unpublished survey of 105 consecutive patients with diabetes revealed that 75% had clinical manifestations of dry skin. (more…)
Assessing moisture and pressure risk in elderly patients continues to be a focus for clinicians in all settings, particularly long-term care. Ongoing research challenges our ideas about and practices for cleansing and protecting damaged skin. Until recently, most wound care clinicians have cleansed long-term care patients’ skin with mild soap and water. But several studies have shown pH-balanced cleansers are more efficient than soap and water for cleansing the skin of incontinent patients.
Various terms are used to describe skin breakdown related to moisture—incontinence-associated dermatitis, perineal dermatitis, diaper rash, intertriginal dermatitis, intertrigo, moisture-related skin damage, moisture-associated skin damage, and even periwound dermatitis. This article uses moisture-associated skin damage (MASD) because it encompasses many causes of skin breakdown related to moisture. Regardless of what we call the condition, we must do everything possible to prevent this painful and costly problem.
Skin assessment
Start with an overall assessment of the patient’s skin. Consider the texture and note dryness, flaking, redness, lesions, macerated areas, excoriation, denudement, and other color changes. (See Identifying pressure and moisture characteristics by clicking the PDF icon above.)
Assessing MASD risk
A patient’s risk of MASD can be assessed in several ways. Two of the most widely used pressure-ulcer risk scales, the Norton and Braden scales, address moisture risk. The Norton and Braden subscales should drive your plan for preventing skin breakdown related to moisture or pressure. The cause of breakdown (moisture, pressure, or shear/friction) must be identified, because treatment varies with the cause.
Both the Norton and Braden scales capture activity, mobility, and moisture scores. The Braden scale addresses sensory perception, whereas the Norton scale identifies mental condition. (See Subscales identifying pressure, shear, and moisture risk by clicking the PDF icon above.) Also, be aware that two scales have been published for perineal risk, but neither has been used widely.
You must differentiate pressure- and moisture-related conditions to determine correct treatment. Patients who are repositioned by caregivers are at risk for friction or shear. Also, know that agencies report pressure-ulcer prevalence. Care providers no longer classify mucous-membrane pressure areas in skin prevalence surveys; mucous membranes aren’t skin and don’t have the same tissue layers. Furthermore, don’t report skin denudement from moisture (unless pressure is present) in prevalence surveys.
When moisture causes skin breakdown
Skin has two major layers—epidermis and dermis. The epidermis itself has five layers: The outermost is the stratum corneum; it contains flattened, keratin protein–containing cells, which aid water absorption. These cells contain water-soluble compounds called natural moisturizing factor (NMF), which are surrounded by a lipid layer to keep NMF within the cell. When skin is exposed to moisture, its temperature decreases, the barrier function weakens, and skin is more susceptible to pressure and friction/shear injury. Also, when urea in urine breaks down into ammonia, an alkaline pH results, which may reactivate proteolytic and lipolytic enzymes in the stool. (See Picturing moisture and pressure effects by clicking the PDF icon above.)
Caring for moisture-related skin breakdown
The standard of care for moisture-related skin breakdown includes four major components: cleanse, moisturize, protect, and contain. Specific products used for each component vary with the facility’s product formulary.
Cleanse
Gently wash the area using a no-rinse cleanser with a pH below 7.0. Don’t rub the skin. Pat dry.
Moisturize
Use creams containing emollients or humectants. Humectants attract water to skin cells and help hold water in the cells; don’t use these products if the skin is overhydrated. Emollients slow water loss from skin and replace intracellular lipids.
Protect
Options for skin protectants include:
• liquid film-forming acrylate sprays or wipes
• ointments with a petroleum, zinc oxide, or dimethicone base
• skin pastes. Don’t remove these products totally at each cleansing, but do remove stool, urine, or drainage from the surface and apply additional paste afterward. Every other day, remove the paste down to the bare skin using a no-rinse cleanser or mineral oil.
Be sure to separate skinfolds and use products that wick moisture rather than trap it. These may include:
• commercial moisture-wicking products
• a light dusting with powder containing refined cornstarch or zinc oxide—not cornstarch from the kitchen or powder with talc as the only active ingredient
• abdominal pads.
Contain
To keep moisture away from skin, use absorbent underpads with wicking properties, condom catheters (for males), fecal incontinence collectors, fecal tubes (which require a healthcare provider order), or adult briefs with wicking or gel properties. Call a certified ostomy or wound care nurse for tips on applying and increasing wear time for fecal incontinence collectors.
If 4″ × 4″ gauze pads or ABD pads are saturated more frequently than every 2 hours, consider applying an ostomy or specially designed wound pouch to the area. Collecting drainage allows measurement and protects skin from the constant wetness of a saturated pad.
Don’t neglect the basics, for example, know that wet skin is more susceptible to breakdown. Turn the patient and change his or her position on schedule. Change linens and underpads when damp, and consider using a low-air-loss mattress or bed or mattress with microclimate technology.
Also, be aware that fungal rashes should be treated with appropriate medications. If the patient’s skin isn’t too moist, consider creams that absorb into the skin; a skin-protecting agent can be used as a barrier over the cream. Besides reviewing and using the standards of care, you may refer to the Incontinence-Associated Dermatitis Intervention Tool, which has categories related to skin damage. See the “Incontinence-Associated Dermatitis Intervention Tool” (IADIT).
Bottom line on skin breakdown
To help prevent skin breakdown related to moisture, assess patients’ skin appropriately, determine treatment using evidence-based guidelines, and implement an appropriate plan of care.
Selected references
Black JM, Gray M, Bliss DZ, et al. MASD part 2: incontinence-associated dermatitis and intertriginous dermatitis: a consensus. J Wound Ostomy Continence Nurs. 2011;38(4):359-70.
Borchert K, Bliss DZ, Savik K, Radosevich DM. The incontinence-associated dermatitis and its severity instrument: development and validation. J Wound Ostomy Continence Nurs. 2010;37(5):527-35.
Doughty D. Differential assessment of trunk wounds: pressure ulceration versus incontinence-associated dermatitis versus intertriginous dermatitis. Ostomy Wound Manage. 2012;58(4):20-2.
Doughty D, Junkin J, Kurz P, et al. Incontinence-associated dermatitis: consensus statements, evidence-based guidelines for prevention and treatment, and current challenges. J Wound Ostomy Continence Nurs. 2012;39(3):303-15.
Gray M, Beeckman D, Bliss DZ, et al. Incontinence-associated dermatitis: a comprehensive review and update. J Wound Ostomy Continence Nurs. 2012;
39(1):61-74.
Gray M, Black JM, Baharestani MM, et al. Moisture-associated skin damage: overview and pathophysiology. J Wound Ostomy Continence Nurs. 2011;38(3):233-41.
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention and treatment of pressure ulcers: clinical practice guideline.Washington, DC: National Pressure Ulcer Advisory Panel; 2009.
Wound, Ostomy and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers. Mt. Laurel, NJ: Wound, Ostomy and Continence Nurses Society; 2010.
Wound, Ostomy and Continence Nurses Society. Incontinence-Associated Dermatitis: Best Practice for Clinicians. Mt. Laurel, NJ: Wound, Ostomy and Continence Nurses Society; 2011.
Zulkowski K. Diagnosing and treating moisture-associated skin damage. Adv Skin Wound Care. 2012;25(5):231-6.
Patricia A. Slachta is an instructor at the Technical College of the Lowcountry in Beaufort, South Carolina.
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
Staphylococcus aureus is one of the most feared human pathogens, causing a wide range of infections. Most wound care professionals can expect to frequently encounter patients with S. aureus infections. Soft-tissue infections caused by S. aureus include impetigo, cellulitis, and cutaneous abscesses, as well as such life-threatening processes as necrotizing fasciitis and pyomyositis (a hematogenous intramuscular abscess). Serious non-soft-tissue infections include septic arthritis, osteomyelitis, pneumonia, endocarditis, and sepsis.
Why is S. aureus such a nasty bug?
S. aureus produces various cellular and extracellular factors involved in the pathogenesis of infection. S. aureus protein A, an important surface protein, helps the organism resist phagocytosis. Also, S. aureus produces several cytotoxins and enzymes that contribute to infection spread and severity. In addition, some strains produce toxins (including toxic shock syndrome toxin-1) that function as superantigens—molecules that nonspecifically trigger release of large amounts of cytokines, leading to a sepsislike condition. Taken together, such factors combine to make S. aureus a dangerous pathogen.
MRSA emergence
When penicillin was introduced in the 1940s, virtually all S. aureus isolates were sensitive to that drug. But soon thereafter, S. aureus strains that produced a β-lactamase enzyme capable of inactivating penicillin became widespread. During the 1950s, outbreaks of penicillin-resistant S. aureus occurred in many U.S. hospitals. Introduction of penicillinase-resistant antibiotics, such as methicillin and oxacillin, temporarily restored the ability to treat all strains of this pathogen using penicillin antibiotics. The first strain of methicillin-resistant S. aureus (MRSA) was described in 1961 shortly after introduction of penicillinase-resistant antibiotics.
The mechanism of methicillin resistance involves a mutation in one of the bacterial cell-wall proteins to which penicillins must bind to kill the bacterium. This mutation renders the organism resistant to all penicillins and penems and almost all cephalosporins.
MRSA incidence has increased steadily to the point where it currently constitutes up to 60% of S. aureus isolates in many U.S. hospitals. These organisms commonly carry genetic material that makes them resistant to various non-β lactam antibiotics as well, leading some to suggest that the term MRSA should stand for multiply resistant S. aureus. S. aureus has continued to mutate in the face of persistent antibiotic pressure. Vancomycin-intermediate S. aureus (VISA) was described in 1997; vancomycin-resistant S. aureus (VRSA), in 2003. Fortunately, these two strains remain rare and haven’t become established pathogens. (See Strains of antibiotic-resistantS. aureus by clicking the PDF icon above.)
Healthcare- versus community-acquired MRSA
Although MRSA initially arose and spread within healthcare settings (chiefly acute-care hospitals), a community-based variant was described in 1998. Called community-
acquired MRSA (CA-MRSA), this variant differs from healthcare-associated MRSA (HCA-MRSA) in more ways than the acquisition site. CA-MRSA occurs predominately in otherwise healthy children and young adults.
It most commonly presents as recurrent cutaneous abscesses, although life-threatening infections (such as necrotizing fasciitis and pneumonia) also have occurred. The propensity to cause cutaneous abscesses isn’t fully understood but may relate partly to production of the Panton-Valentine toxin by many CA-MRSA isolates.
In contrast, HCA-MRSA afflicts mainly older patients, particularly those with chronic illnesses, including chronic wounds. It typically causes wound infections, urinary tract infections, pneumonia, and bacteremia.
Besides these epidemiologic and clinical differences, many CA-MRSA isolates derive from a single clone, known as clone USA 300, whereas HCA-MRSA is composed of multiple non-USA 300 clones. Finally, many CA-MRSA isolates are sensitive to non-β
lactam antibiotics, whereas most HCA-MRSA isolates resist multiple antibiotics. More recently, the distinction between CA-MRSA and HCA-MRSA has been blurred as evidence emerges that CA-MRSA now is being transmitted in healthcare settings as well as in the community.
S. aureus carrier state
Staphylococci are frequent colonizers of humans. Common colonization sites include the skin, anterior nares, axillae, and inguinal regions. Individuals can be colonized continuously or transiently, with nasal carriage rates varying from 20% to 40%. Most S. aureus infections result from the strain carried by the infected patient.
Three patterns of S. aureus carriage exist in humans:
• 20% of individuals are continuously colonized.
• 30% of individuals are intermittently colonized.
• 50% of individuals are never colonized.
The highest carriage rates occur in patients receiving frequent injections (such as insulin-dependent diabetics, hemodialysis patients, and I.V. drug users) and those with chronic skin conditions (for instance, psoriasis or eczema). In the general population, MRSA carriage rates have increased to 1% or 2%, with clinical consequences hinging on the colonizing strain (CA-MRSA versus HCA-MRSA) and host characteristics. The most consistent carriage site is the anterior nares, but many other sites may carry this pathogen, including the axillae, inguinal regions, and perirectal area.
MRSA treatment
Therapy for MRSA infection depends on the infection location and antibiotic sensitivity of the infecting strain.
• Cutaneous abscesses are treated by incision and drainage; antibiotics play a secondary role to adequate drainage.
• Therapy for necrotizing fasciitis caused by MRSA involves aggressive debridement with removal of all necrotic tissue, plus adequate antibiotic therapy. Typically, patients require serial debridement followed by subsequent careful wound care, often with eventual skin grafting.
• Pyomyositis treatment entails drainage of the muscle abscess (which sometimes can be done with percutaneous tube placement instead of open drainage), plus appropriate antibiotic therapy.
Vancomycin has been the mainstay of I.V. therapy for MRSA for decades, but some clinicians are concerned that its effectiveness may be declining due to slowly increasing minimum inhibitory concentrations (the minimum concentration of an
antibiotic needed to inhibit pathogen growth). Other parenteral options have emerged in the last few years. (See I.V. drugs used to treat MRSA by clicking the PDF icon above.) Several oral antibiotics also are available for MRSA treatment. (See Oral agents used to treat MRSA by clicking the PDF icon above.)
Knowing the antibiotic sensitivity pattern of the infecting MRSA strain is crucial to ensuring that the patient receives an appropriate antibiotic. Treatment duration for soft-
tissue infections usually ranges from 7 to 14 days, but bacteremia and bone or joint infections call for more prolonged therapy.
Efforts to eradicate MRSA carriage
Because the carrier state increases the risk of subsequent S. aureus infection, efforts have been made to eradicate carriage. Unfortunately, this has proven to be difficult. A commonly used regimen involves 5 days of twice-daily mupirocin nasal ointment with either chlorhexidine gluconate showers or immersion up to the neck in a dilute bleach solution. However, success in eliminating carriage is limited, although the bleach bath seems to improve eradication rates better than other modalities.
Controlling MRSA in hospitals
How best to control MRSA spread within hospitals is controversial. Some experts advocate an aggressive, “search and destroy” approach involving screening all patients for nasal carriage on admission and initiating contact precautions with subsequent decolonization efforts. Others focus on improving the overall level of hand hygiene and other general infection-control measures, arguing that nasal screening misses at least 20% of MRSA-colonized patients and thus gives an unwarranted sense of security.
Many hospitals use a mixed approach, screening patients suspected to be at high risk for MRSA carriage (such as those admitted from extended-care facilities or to the intensive care unit), while simultaneously trying to improve hand hygiene and general infection-control measures. Recent data suggest MRSA colonization and infection rates have stopped increasing and are beginning to decline.
MRSA is one of the most problematic pathogens encountered on a regular basis, and among the most dangerous pathogens we face. While some MRSA infections are relatively mild, many are serious or life-threatening. Severe soft-tissue infections, such as necrotizing fasciitis and pyomyositis, require surgical debridement or drainage, appropriate antibiotic therapy, and assistance from a wound-care professional to achieve optimal outcomes. n
Selected references
Calfee DP. The epidemiology, treatment and prevention of transmission of methicillin-resistant Staphylococcus aureus. J Infus Nurs. 2011 Nov-Dec;34(6):359-64.
DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010 May 1;375(9725): 1557-68.
Ippolito G, Leone S, Lauria FN, et al. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010 Oct;14 Suppl 4:S7-11.
Landrum ML, Neumann C, Cook C, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010. JAMA. July 4;308:50-9.
Lee AS, Huttner B, Harbarth S. Control of methicillin-resistant Staphylococcus aureus. Infect Dis Clin North Am. 2011 Mar;25(1):155-79.
Moellering RC Jr. MRSA: the first half century. J Antimicrob Chemother. 2012 Jan;67(1):4-11.
Otter JA, French GL. Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection. J Hosp Infect. 2011 Nov:79(3):189-93.
Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant pneumococci, and vancomycin-resistant enterococci. Mayo Clin Proc. 2011 Dec;86(12):1230-43.
Simor AE. Staphylococcal decolonization: an effective strategy for prevention of infection? Lancet Infect Dis. 2011 Dec;11(12):952-62.
Joseph G. Garner is director of the infectious disease division and hospital epidemiologist at the Hospital of Central Connecticut and a professor of medicine at the University of Connecticut.
Every year, thousands of people of all ages have ostomy surgery in the United States. That means no matter where you work, you’re likely to care for patients with new ostomies and teach them to care for themselves. (See Why patients need ostomy surgery by clicking the PDF icon above.)
These patients present two challenges: staying up-to-date on ostomy equipment and procedures and having only 3 to 5 days after surgery to teach basic ostomy care to patients who are unlikely to be physically or emotionally ready to learn. This review and update of ostomy care should help you meet both challenges. Let’s start with the common types of stomas and ostomies.
Reviewing stoma types
The three common types of stomas are the end stoma, loop stoma, and double-barrel stoma. The patient’s surgeon decides on the most appropriate type based on the disease or injury, the amount of intestine available, and the patient’s health status.
To create an end stoma, the most common type, a surgeon creates a small opening in the abdominal wall, then resects the intestine and pulls it through the opening. Next, the surgeon turns the end of the intestine onto itself—somewhat like cuffing a sock—and sutures the stoma to the skin. Next to the stoma, the surgeon may create a mucous fistula, which secretes mucus from the nonfunctioning portion of the intestine.
A loop stoma is usually created for a temporary ostomy. The surgeon creates a small opening in the abdominal wall and pulls a loop of intestine through it. With an external rod or bridge placed under the loop to keep it from slipping back into the peritoneal cavity, the surgeon cuts the top of the loop to form the apex of the stoma. Next, the surgeon everts the intestine around the opening and sutures the stoma edges to the skin. After a few days, the rod is removed, and the stoma stays above skin level on its own. Double-barrel stomas aren’t common in adults, but they are used frequently in neonates. For this type, a surgeon cuts through the bowel to create two separate end stomas, one to evacuate stool and the other to evacuate mucus. The two stomas can be placed next to each other, so one pouching system can be used for both. If the stomas are further apart, the patient may need two pouches. If mucus secretions are slight, you may be able to apply a nonadherent dressing after gently cleaning the stoma and peristomal skin, instead of using a pouch.
An ideal stoma protrudes above the skin surface and has a flat peristomal skin surface that allows the ostomy barrier to adhere to it. (See Characteristics of an ideal stoma by clicking the PDF icon above.) A healthy stoma is red and moist and looks like gum tissue. In fact, the entire alimentary canal from mouth to anus has the same type of tissue. Keep in mind that while cleaning a stoma, you’ll commonly see a small amount of bleeding, just as your gums may bleed when you brush your teeth too vigorously. If you note excessive bleeding, report it immediately.
Reviewing types of ostomies
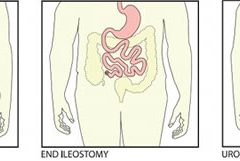
The three most common types of ostomies you’ll see are a colostomy, an ileostomy, and a urostomy.
A surgeon creates a colostomy by making an opening in the large intestine and connecting it to the stoma. The location of the surgical opening will affect the consistency of the stool exiting the body through the stoma: The lower the opening, the firmer the consistency. A colostomy produces flatus because of the high bacterial content in the large intestine. A colostomy can be temporary or permanent, depending on the diagnosis and the patient’s ability to heal.
To create an ileostomy, a surgeon makes an opening in the small intestine and forms a stoma. Patients with ileostomies are prone to dehydration because a large amount of enzymatic fluid is discharged through the ileostomy instead of being absorbed in the disconnected large intestine. Teach your patient to be alert for the signs and symptoms
of dehydration—thirst; decreased urination; darker, concentrated urine; warm, flushed skin; fever; and malaise. Also, warn the patient to keep enzymatic effluent off the skin because it can quickly cause skin breakdown. As with a colostomy, an ileostomy may be temporary or permanent.
To create a urostomy, a surgeon removes the diseased bladder and uses a portion of resected small intestine to create a conduit. The ureters, which were connected to the bladder, are sutured into the resected small intestine so urine can exit the body through the stoma. Urostomies are permanent.
Choosing the right pouching system
An ostomy pouching system has two parts: an adhesive barrier that attaches to the skin around the stoma and a pouch connected to the barrier that collects effluent. Determining the right ostomy pouching system for your patients will depend on their needs and preferences. Let’s look at some of the important choices.
A pouching system may come in one or two pieces. With one-piece systems, the barrier (also called the wafer, flange, or baseplate) and pouch come as a single unit. (See One- and two-piece ostomy pouching systems by clicking the PDF icon above.) One-piece systems are easier to apply and more flexible. Plus, they’re flatter and thus more discreet.
With two-piece systems, the barrier and pouch are separate components that must be attached. Depending on the product, the patient may need to press the pouch onto the barrier or use a locking ring mechanism or an adhesive coupling system. Two-piece systems allow the patient to remove the pouch without removing the barrier. Also, a patient can apply a smaller pouch, such as a stoma cap or close-ended pouch, before exercise or intimate relations.
Today, ostomy pouching systems offer many options that weren’t available just a few years ago—options such as built-in, varying levels of convexity and integrated closures. Skin-friendly barriers now eliminate the need for accessory products, such as skin prep, ostomy powder, and stoma paste. By knowing the new options, you can help simplify the pouch application process for your patient and increase patient satisfaction.
Selecting barriers
Barriers may be cut-to-fit or precut. Cut-to-fit barriers are used during the postoperative period while the stoma size is changing and for oval or irregularly shaped stomas. Precut sizes are convenient for round stomas after they stabilize.
The choice of a barrier also depends on abdominal contours and the effluent consistency. A standard-wear barrier is appropriate for thicker output. An extended-wear barrier is better for loose or watery output and for problematic ostomies.
Convex barriers can be used to push down the peristomal skin and help the stoma project into the pouch. These barriers help ensure that the effluent goes into the pouch and not between the skin and the barrier, causing leakage.
For ostomies that are difficult to manage and frequently leak, you may select an ostomy belt. This device helps secure a convex pouching system by increasing its pressure. The plastic hooks at the end of the belt attach to the belt loops of the pouching system. Depending on the manufacturer, the belt loops may be on the barrier or the pouch.
Selecting pouches
Pouches can be transparent or opaque. Transparent pouches allow you to see the stoma postoperatively and allow patients to watch as they place the pouch over the stoma. Opaque pouches, of course, have the advantage of concealing the effluent.
Some pouches have filters. Colostomy patients usually prefer filtered pouches because they eliminate the need to burp the pouch to remove gas. Ileostomy output is usually watery, so the charcoal filters may get wet and quit working.
The appropriate type of pouch closure also varies, depending on the type of output and the patient’s needs and preferences. A patient with a colostomy or ileostomy needs a drainable pouch. Newer clamps and integrated closures can make closing the pouch easier for the patient.
Close-ended pouches are available for patients who empty their pouch once or twice a day. Reimbursement guidelines for Medicare, which most insurance companies follow, allow 60 close-ended pouches a month. Thus, someone who empties once or twice a day will have enough pouches.
Patients with urostomies use pouches with spigots on the end to allow for urine drainage.
Urostomy pouches can be connected to a continuous urinary drainage bag at bedtime or to a leg bag during the day for those in a wheelchair.
Dealing with complications
Report the following postoperative complications to the surgeon and the ostomy clinician caring for the patient:
• allergic reaction
• candidiasis
• contact dermatitis
• folliculitis
• ischemic or necrotic stoma
• mechanical irritation
• mucocutaneous separation
• parastomal hernia
• prolapse.
Many complications result from surgical technique or the patient’s disease status, but complications also result from an incorrect fit or an ostomy that frequently leaks. To determine why and where leakage occurred, examine the back of the barrier. If leakage results from a flush or recessed stoma or an irregular surface around the stoma, the patient may need a convex barrier. Or the patient may need a convex barrier and an ostomy belt.
Remember that a firm abdomen requires a soft, flexible barrier that conforms to the abdominal contours. A soft belly, on the other hand, may need the rigidity of a convex barrier to help the stoma empty into the pouch.
For weepy, extremely denuded skin, apply ostomy powder, brush off the excess, and dab an alcohol-free skin sealant, such as No-Sting by 3M, on the area. Allow the area to air-dry before applying the barrier.
Discharge planning and patient teaching
Because the postoperative length of stay is short, start preparing for discharge and teaching the pouch-change procedure at your first hospital encounter with the patient. Teaching the patient at each encounter creates a continuum of care throughout hospitalization and recovery. If possible, include the caregiver. (See Teaching your patient to change an ostomy pouch by clicking the PDF icon above.) Before discharge, give the patient two or three ostomy pouches to take home, step-by-step printed instructions on applying pouches, a list of supplies the patient will need, and a list of ostomy product suppliers in the area.
Also, teach the patient about complications, activity, diet, and drug therapy and provide the names of local support groups. (See Finding support by clicking the PDF icon above.)
Complications at home
Tell the patient to call the physician if any of the following occurs: fever, increased pain or discomfort, diarrhea, dehydration, or signs and symptoms of infection at the surgical site. The patient should also call the physician if there’s no output from the stoma for more than 24 hours.
Patients with urostomies who develop the following signs and symptoms may have a urinary tract infection: fever, chills, abdominal or retroperitoneal pain, and bloody, cloudy, or foul-smelling urine. Clear urine with mucus shreds is normal.
Increasing activity
Explain that after surgery the patient should feel a little bit stronger every day. Teach the patient to alternate rest and activity periods and to increase the activity period a little each day while building endurance. Refer the patient to the physician for clearance to resume exercise and sexual relations.
Dietary considerations
After ostomy surgery, your patient will start on a clear liquid diet and progress to a normal, preoperative diet. The patient should reintroduce one food at a time to help determine if it’s well tolerated. High-fiber foods should be introduced slowly.
Tell your patient to expect his or her body to tolerate the food as it did before surgery: if onions caused gas before surgery, they will do so after surgery, too, but the stoma will expel the gas. Make the patient aware of other gas-forming foods, such as hard-boiled eggs, spicy foods, fish, dried beans, carbonated beverages, and beer.
Tell the patient to chew food well and to drink plenty of liquids, which will prevent blockage. Explain the importance of hydration to avoid constipation, dehydration, and urinary tract infection. To prevent dehydration, ileostomy patients who are not on fluid restriction should drink 64 ounces of fluid a day. Teach these patients to replace fluids by drinking a glass of water every time they empty their pouches.
Drug therapy
Tell the patient to adhere to the prescribed regimen and to call the physician before using any new drugs. Instruct patients with ileostomies not to take laxatives because they may become dehydrated. These patients should tell their pharmacist that they have an ileostomy, so the proper form of prescription drugs can be ordered. Extended-release tablets will not break down in time and may be found in the pouch.
Rewarding work
Keeping up with the changes in ostomy equipment and care and teaching new ostomy patients the skills they need can be challenging. But helping these patients regain the confidence and learn the skills they need to improve their quality of life makes the rewards much greater than the challenges.
Selected references
Colwell J. Principles in stoma management. In: Colwell JC, Goldberg MT, Carmel JE, eds. Fecal and Urinary Diversions Management Principles. St. Louis, MO: Mosby; 2004:240-262.
Discharge Planning for a Patient with a New Ostomy: Best Practice for Clinicians. Glenview, IL: Wound, Ostomy and Continence Nurses Society; 2004.
Hampton BG, Bryant RA. Ostomies and Continent Diversions: Nursing Management. St. Louis, MO: Mosby; 1992.
McCann E. Common ostomy problems. In: Milne C, Corbett L, Dubuc D. Wound, Ostomy, and Continence Nursing Secrets: Questions and Answers Reveal the Secrets to Successful WOC Care. Philadelphia, PA: Hanley & Belfus, Inc; 2004.
The Sarah Cole Hirsh Institute for Best Nursing Practices Based on Evidence. State of the evidence review hospital to home: Planning the transitions. 2000; Cleveland, OH.
Goranka Paula Bak is an Ostomy Sales Territory Manager for Coloplast Corporation.
By Nancy Chatham, MSN, RN, ANP-BC, CWOCN, CWS, and Carrie Carls, BSN, RN, CWOCN, CHRN
Moisture-related skin breakdown has been called many things-perineal dermatitis, irritant dermatitis, contact dermatitis, heat rash, and anything else caregivers could think of to describe the damage occurring when moisture from urine or stool is left on the skin. At a 2005 consensus conference, attendees chose the term incontinence-associated dermatitis (IAD).
IAD can be painful, hard to properly identify, complicated to treat, and costly. It’s part of a larger group of moisture-associated skin damage that also includes intertrigo and periwound maceration. IAD prevalence and incidence vary widely with the care setting and study design. Appropriate diagnosis, prompt treatment, and management of the irritant source are crucial to long-term treatment.
Causes
IAD stems from the effects of urine, stool, and containment devices on the skin. The skin’s pH contributes to its barrier functions and defenses against bacteria and fungus; ideal pH is 5.0 to 5.9. Urine pH ranges from 4.5 to 8.0; the higher range is alkaline and contributes to skin damage.
Skin moisture isn’t necessarily damaging. But when moisture that contains irritating substances, such as alkaline urine, contacts the skin for a prolonged period, damage can occur. Urine on the skin alters the normal skin flora and increases permeability of the stratum corneum, weakening the skin and making it more susceptible to friction and erosion. Fecal incontinence leads to active fecal enzymes on the skin, which contribute to skin damage. Fecal bacteria can penetrate the skin, increasing the risk of secondary infection. Wet skin has a lower temperature than dry skin; wet skin under a pressure load has less blood flow than dry skin.
Containment devices, otherwise known as adult diapers or briefs, are multilayer disposable garments containing a superabsorbent polymer. The polymer is designed to wick and trap moisture in the containment device. This ultimately affects the skin by trapping heat and moisture, which may cause redness and inflammation that can progress to skin erosion. This trapping can lead to increased pressure against the skin, especially if the device has absorbed liquid and remains in contact with the skin.
Categorizing IAD
IAD is categorized as mild, moderate, or severe. (See Picturing IAD by clicking the PDF icon above.)
Screening for IAD
Screen the patient’s skin for persistent redness, inflammation, rash, pain, and itching at least daily. To differentiate IAD from pressure ulcers, keep in mind that:
IAD can occur wherever urine or stool contacts the skin. In contrast, pressure ulcers arise over bony prominences in the absence of moisture.
With IAD, affected skin is red or bright red. With a pressure ulcer, skin may take on a bluish purple, red, yellow, or black discoloration.
The skin-damage pattern in IAD usually is diffuse. With a pressure ulcer, edges are well defined.
The depth of IAD-related skin damage usually is partial-thickness without necrotic tissue. With a pressure ulcer, skin damage depth may vary.
Preventing IAD
The three essentials of IAD prevention are to cleanse, moisturize, and protect.
Cleanse the skin with a mild soap that’s balanced to skin pH and contains surfactants that lift stool and urine from the skin. Clean the skin routinely and at the time of soiling. Use warm (not hot) water, and avoid excess force and friction to avoid further skin damage.
Moisturize the skin daily and as needed. Moisturizers may be applied alone or
incorporated into a cleanser. Typically, they contain an emollient such as lanolin to replace lost lipids in the stratum corneum.
To protect the skin, apply a moisture-barrier cream or spray if the patent has significant urinary or fecal incontinence (or both). The barrier may be zinc-based, petrolatum-based, dimethicone-based, an acrylic polymer, or another type. Consider using an algorithm developed by wound and skin care specialists that’s customized for skin care products your facility uses. (See Skin care algorithm by clicking the PDF icon above.)
If the treatment protocol fails, the patient should be referred to an appropriate skin care specialist promptly.
To help prevent urine or stool from contacting the patient’s skin, consider using a male external catheter, a female urinary pouch, a fecal pouch, or a bowel management system. Avoid containment devices. If the patient has a containment pad, make sure it’s highly absorbent and not layered, to decrease pressure under the patient.
Managing IAD
A comprehensive multidisciplinary approach to IAD is essential to the success of any skin care protocol. Identify skin care champions within your facility and educate them on IAD. Incorporating administrators, physicians, nursing staff, therapists, and care assistants makes implementation of protocols and algorithms within an institution seamless.
Administrators support the skin care program in the facility, including authorizing a budget so product purchases can be made. The certified wound clinician is the team expert regarding skin care, incontinence, prevention, and product recommendation. The physician oversees protocol development and evaluates and prescribes additional treatment when a patients fails to respond to treatment algorithms. Nursing staff identify patients at risk, incorporate the algorithm into the patient’s plan of care, and direct care
assistants. Therapists address function, strength, and endurance issues to improve the patient’s self-care abilities in activities of daily living to manage or prevent episodes of incontinence.
In severe inflammation, topical dressings, such as alginates and foam dressings, may be used along with topical corticosteroids. In complex IAD, antifungals or antibiotics may be required if a secondary fungal or bacterial infection is suspected.
Additional diagnostic tests may be done to identify and treat secondary infections. These tests may include skin scraping, potassium hydroxide test or Gram’s stain for fungal components, or a swab culture and sensitivity for bacterial infections. If your patient has a suspected secondary fungal or bacterial infection, use appropriate treatments for the full course of recommended therapy. In severe secondary fungal infection, an oral agent may be added to topical therapy. If cost is a concern, consider using a pharmacy knowledgeable about compounding for topical combination therapies.
Referrals and education
For assessment and treatment of under-lying incontinence, refer the patient to a continence specialist if appropriate. Teach the patient strategies for managing incontinence through dietary measures, toileting programs, pelvic-floor muscle training, clothing modification, and mobility aids.
Selected references
Beguin A, Malaquin-Pavan E, Guihaire C, et al., Improving diaper design to address incontinence associated dermatitis. BMC Geriatrics. 2010;10:86. http://www.biomedcentral.com/1471-2318/10/86. Accessed March 15, 2012.
Black JM, Gray M, Bliss DZ, et al. MASD part 2: incontinence-associated dermatitis and intertriginous dermatitis. J Wound Ostomy Continence Nurs. 2011; 38(4):359-370.
Bliss DZ, Zehrer C, Savik K, et al. An economic evaluation of four skin damage prevention regimens in nursing home residents with incontinence: economics of skin damage prevention. J Wound Ostomy Continence Nurs. 2007;34(2):143-152.
Denat Y, Khorshid L. The effect of 2 different care products on incontinence-associated dermatitis in patients with fecal incontinence. J Wound Ostomy Continence Nurs. 2011;38(2):171-176.
Doughty DB. Urinary and Fecal Incontinence: Current Management Concepts. 3rd ed. St. Louis, MO: Mosby Elsevier; 2006.
Gray, M. Optimal management of incontinence-associated dermatitis in the elderly. Am J Clin Dermatol. 2010;11(3):201-210.
Gray M, Beeckman D, Bliss DZ, et al. Incontinence-associated dermatitis: a comprehensive review and update. J Wound Ostomy Continence Nurs. 2012;39(1):61-74
Gray M, Bliss DZ, Doughty DB, et al. Incontinence-associated dermatitis: a consensus. J Wound Ostomy Continence Nurs. 2007;34(1):45-54.
Gray M, Bohacek L, Weir D, et al. Moisture vs pressure: making sense out of perineal wounds. J Wound Ostomy Continence Nurs. 2007;34(2):134-42.
Junkin J, Lerner-Selekof JL. Prevalence of incontinence and associated skin injury in the acute care inpatient. J Wound Ostomy Continence Nurs. 2007;34(3):260-269.
Landefeld CS, Bowers BJ, Feld AD, et al. National Institutes of Health state-of-the-science conference statement: prevention of fecal and urinary incontinence in adults. Ann Intern Med. 2008;148(6):449-458.
Langemo D, Hanson D, Hunter S, et al. Incontinence and incontinence-associated dermatitis. Adv Skin Wound Care. 2011;24(3):126-142.
Nancy Chatham is an advanced practice nurse at Passavant Physician Associates in Jacksonville, Illinois. Carrie Carls is the nursing director of advanced wound healing and hyperbaric medicine at Passavant Area Hospital in Jacksonville, Illinois.