Click here to read this article.
Read MoreSearch Results for: Protein re
Leprosy cases are rising in the US – what is the ancient disease and why is it spreading now?

By Robert A. Schwartz, Rutgers University
The word “leprosy” conjures images of biblical plagues, but the disease is still with us today. Caused by infectious bacteria, some 200,000 new cases are reported each year, according to the World Health Organization. In the United States, leprosy has been entrenched for more than a century in parts of the South where people came into contact with armadillos, the principle proven linkage from animal to humans. However, the more recent outbreaks in the Southeast, especially Florida, have not been associated with animal exposure.
The Conversation talked with Robert A. Schwartz, professor and head of dermatology at Rutgers New Jersey Medical School, to explain what researchers know about the disease.
What is leprosy and why is it resurfacing in the US?
Leprosy is caused by two different but similar bacteria — Mycobacterium leprae and Mycobacterium lepromatosis — the latter having just been identified in 2008. Leprosy, also known as Hansen’s disease, is avoidable. Transmission among the most vulnerable in society, including migrant and impoverished populations, remains a pressing issue.
This age-old neglected tropical disease, which is still present in more than 120 countries, is now a growing challenge in parts of North America.
Leprosy is beginning to occur regularly within parts of the southeastern United States. Most recently, Florida has seen a heightened incidence of leprosy, accounting for many of the newly diagnosed cases in the U.S.
The surge in new cases in central Florida highlights the urgent need for health care providers to report them immediately. Contact tracing is critical to identifying sources and reducing transmission.
Traditional risk factors include zoonotic exposure and having recently lived in leprosy-endemic countries. Brazil, India and Indonesia have each noted more than 10,000 new cases since 2019, according to the World Health Organization data, and more than a dozen countries have reported between 1,000 to 10,000 new cases over the same time period.
Why was leprosy stigmatized in biblical times?
Evidence suggests that leprosy has plagued civilization since at least the second millennium B.C.
From that time until the mid-20th century, limited treatments were available, so the bacteria could infiltrate the body and cause prominent physical deformities such as disfigured hands and feet. Advanced cases of leprosy cause facial features resembling that of a lion in humans.
Many mutilating and distressing skin disorders such as skin cancers and deep fungal infections were also confused with leprosy by the general public.
Fear of contagion has led to tremendous stigmatization and social exclusion. It was such a serious concern that the Kingdom of Jerusalem had a specialized hospital to care for those suffering from leprosy.
How infectious is leprosy?
Research shows that prolonged in-person contact via respiratory droplets is the primary mode of transmission, rather than through normal, everyday contact such as embracing, shaking hands or sitting near a person with leprosy. People with leprosy generally do not transmit the disease once they begin treatment.
Armadillos represent the only known zoonotic reservoir of leprosy-causing bacteria that threaten humans. These small mammals are common in Central and South America and in parts of Texas, Louisiana, Missouri and other states, where they are sometimes kept as pets or farmed as meat. Eating armadillo meat is not a clear cause of leprosy, but capturing and raising armadillos, along with preparing its meat, are risk factors.
The transmission mechanism between zoonotic reservoirs and susceptible individuals is unknown, but it is strongly suspected that direct contact with an infected armadillo poses a significant risk of developing leprosy. However, many cases reported in the U.S. have demonstrated an absence of either zoonotic exposure or person-to-person transmission outside of North America, suggesting that transmission may be happening where the infected person lives. But in many cases, the source remains an enigma.
Some people’s genetics might make them more susceptible to leprosy infections, or their immune systems are less capable of resisting the disease.
Stigma and discrimination have prevented people from seeking treatment, and as a result, “concealed” cases contribute to transmission.
How do you recognize it?
Leprosy primarily affects the skin and peripheral nervous system, causing physical deformity and desensitizing one’s ability to feel pain on affected skin.
It may begin with loss of sensation on whitish patches of skin or reddened skin. As the bacteria spread in the skin, they can cause the skin to thicken with or without nodules. If this occurs on a person’s face, it may rarely produce a smooth, attractive-appearing facial contour known as lepra bonita, or “pretty leprosy.” The disease can progress to causing eyebrow loss, enlarged nerves in the neck, nasal deformities and nerve damage.
The onset of symptoms can sometimes take as long as 20 years because the infectious bacteria have a lengthy incubation period and proliferate slowly in the human body. So presumably many people are infected long before they know that they are.
Fortunately, worldwide efforts to screen for leprosy are being enhanced thanks to organizations like the Order of Saint Lazarus, which was originally founded in the 11th century to combat leprosy, and the Armauer Hansen Research Institute, which conducts immunologic, epidemiological and translational research in Ethiopia. The nongovernmental organization Bombay Leprosy Project in India does the same.
How treatable is it?
Leprosy is not only preventable but treatable. Defying stigma and advancing early diagnosis via proactive measures are critical to the mission of controlling and eradicating it worldwide.
Notably, the World Health Organization and other agencies provide multi-drug therapy at no cost to patients.
In addition, vaccine technology to combat leprosy is in the clinical trials stage and could become available in coming years. In studies involving nine-banded armadillos, this protein-based vaccine delayed or diminished leprous nerve damage and kept bacteria at bay. Researchers believe that the vaccine can be produced in a low-cost, highly efficient manner, with the long-term prospect of eradicating leprosy.
If health care professionals, biomedical researchers and lawmakers do not markedly enhance their efforts to eliminate leprosy worldwide, the disease will continue to spread and could become a far more serious problem in areas that have been largely free of leprosy for decades.
The World Health Organization launched a plan in 2021 for achieving zero leprosy.![]()
Robert A. Schwartz, Professor and Head of Dermatology, Rutgers New Jersey Medical School, Rutgers University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Read MoreSilk wound dressing helps eliminate scar tissue formation
Researchers from Huazhong University of Science and Technology, China have developed a new type of wound dressing, based on a silk protein sericin hydrogel, that can achieve skin regeneration with little to no scar tissue formation. Testing has shown the hydrogel is able to block bacteria from entering the wound, promoting accelerated healing.
Read MoreFish Skin for Human Wounds: Iceland’s Pioneering Treatment

The FDA-approved skin substitute reduces inflammation and transforms chronic wounds into acute injuries.
Six hours north of Reykjavik, along a narrow road tracing windswept fjords, is the Icelandic town of Isafjordur, home of 3,000 people and the midnight sun. On a blustery May afternoon, snow still fills the couloirs that loom over the docks, where the Pall Palsson, a 583-ton trawler, has just returned from a three-day trip. Below the rust-spotted deck, neat boxes are packed with freshly caught fish and ice. “If you take all the skins from that trawler,” says Fertram Sigurjonsson, the chairman and chief executive officer of Kerecis Ltd., gesturing over the catch, “we would be able to treat one in five wounds in the world.” (more…)
Read MoreSkin substitutes: Understanding product differences
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make.
Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled procedures and herbal treatments to heal wounds, including xenografts (skin from another species). The practice of applying allografts (human cadaver skin) to wounds was first documented in 1503. In 1871, autologous skin grafting (skin harvested from the the person with the wound) was tried. Next came epithelial- cell seeding, which involves scraping off the superficial epithelium of healthy skin and transplanting the cells onto the wound. (more…)
Read MoreHerpes zoster: Understanding the disease, its treatment, and prevention

Herpes zoster (HZ, also called shingles) is a painful condition that produces a maculopapular and vesicular rash. Usually, the rash appears along a single dermatome (band) around one side of the body or face.
In most cases, pain, tingling, burning, or itching occurs a few days before the rash. Next, blisters form, scabbing over in 7 to 10 days. In rare cases, the rash is widespread, resembling varicella zoster (VZ, or chickenpox) rash. Pain can range from mild to severe and may be dull, burning, or gnawing. It may last weeks, months, or even years after the blisters heal. Shingles on the face may impair vision or hearing. (more…)
Read MoreLymphedema and lipedema: What every wound care clinician should know

Imagine you have a health condition that affects your life every day. Then imagine being told nothing can be done about it; you’ll just have to live with it. Or worse yet, your physician tells you the problem is “you’re just fat.”
Many people with lymphedema or lipedema have no idea their condition has a name or that many other people suffer from the same thing. Although lymphedema and lipedema can’t be cured, proper management and resources can help patients cope. This article improves your grasp of these conditions, describes how to recognize and manage them, and explains how to support your patients.
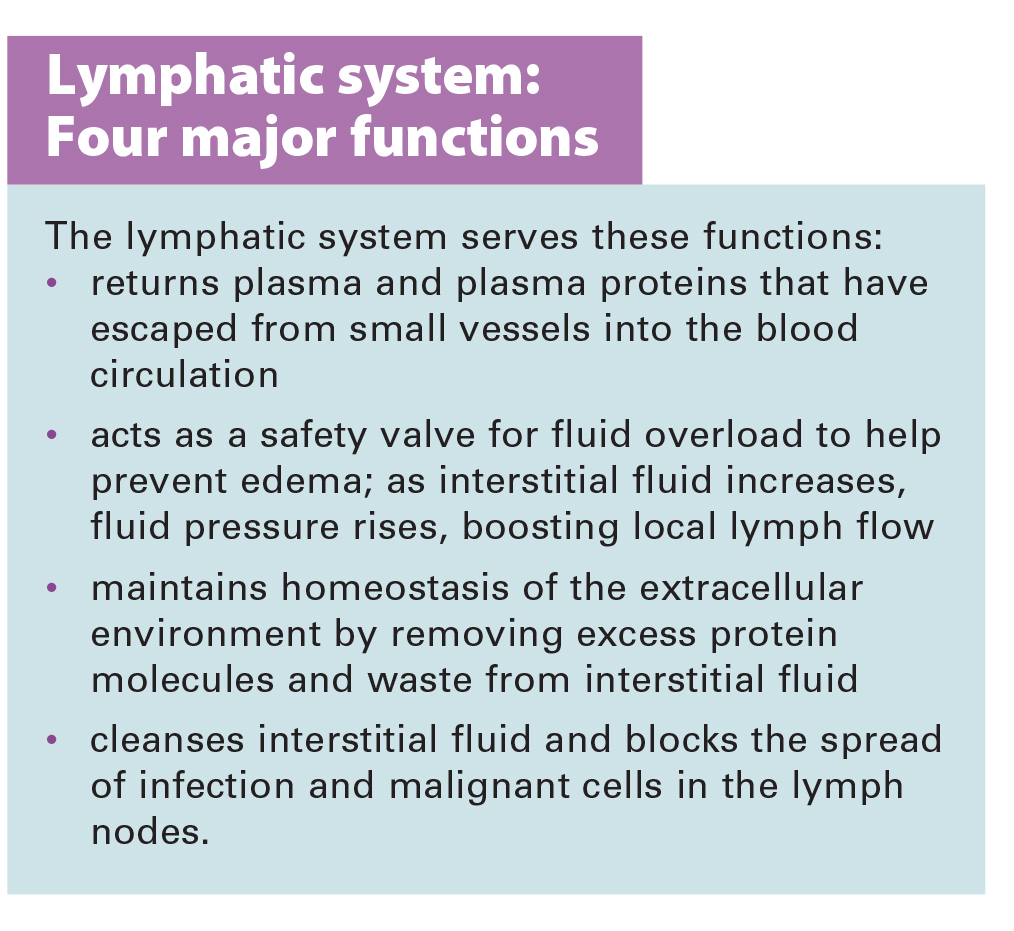
To understand lymphedema and lipedema, first you need to understand how the lymphatic system functions. It makes lymph, then moves it from tissues to the bloodstream. It also plays a major role in the immune system, aiding immune defense. In addition, it helps maintain normal fluid balance by promoting fluid movement from the interstitial tissues back to the venous circulation. (See Lymphatic system: Four major functions.)
{kind=link}
If the lymphatic system is impaired from a primary (hereditary or congenital) condition or a secondary problem, lymphedema can result. In this chronic, potentially progressive, and incurable condition, protein-rich fluid accumulates in the interstitial tissues.
Lymphedema basics
Lymphedema occurs in four stages.
Stage 0. During this stage (also called the subclinical or latency stage), transport capacity of the lymphatic system decreases but remains sufficient to manage normal lymphatic loads. Signs and symptomsaren’t evident and can be measured only by sensitive instruments, such as bioimpedance spectroscopy and optoelectronic volumetry. Without such instruments to quantify volume changes, diagnosis may rest on subjective complaints.
In this stage, limited functional reserve of the lymphatic system leads to a fragile balance between subnormal transport capacity and lymphatic loads. Added stress on the lymphatic system (as from extended heat or cold exposure, injury, or infection) may cause progression to stage 1.
Providing appropriate patient information and education, especially after surgery, can dramatically reduce the risk that lymphedema will progress to a more serious stage.
Stage 1. Considered the spontaneously reversible stage, stage 1 is marked by softtissue pliability without fibrotic changes. Pitting can be induced easily. In early stage 1, limb swelling may recede over – night. With proper management, the patient can expect the extremity to decrease to a normal size compared to that of the uninvolved limb. Otherwise, lymphedema is likely to progress to stage 2.
Stage 1 lymphedema may be hard to distinguish from edemas from other causes. Clinicians must rely on the patient history and monitor for swelling resolution with conventional management, such as compression and elevation, or note if swelling persists despite these standard interventions.
Stage 2. Sometimes called the spontaneously irreversible stage, stage 2 is identified mainly from tissue proliferation and subsequent fibrosis (called lymphostatic fibrosis). The fluid component can be removed spontaneously, but removal of the increased tissue proliferation (initially irreversible) takes more time. Tissue proliferation stems from long-standing accumulation of protein-rich fluid; over time, the tissue hardens and pitting is hard to induce. In many cases, swelling volume increases, exacerbating the already compromised local immune defense.
Consequently, infections (particularly cellulitis) are common; these, in turn, increase the volume of the affected area. Proper treatment can reduce volume.
With proper care (complete decongestive therapy [CDT]), lymphedema can stabilize during stage 2. But patients with chronic or recurrent infections are likely to progress to stage 3.
Stage 3. Also called lymphostatic elephantiasis, this stage is marked by further fluid volume increases and progression of tissue changes. Lymphostatic fibrosis becomes firmer and other skin alterations may occur, including papillomas, cysts, fistulas, hyperkeratosis, fungal infections, and ulcers. Pitting may be present. Natural skinfolds deepen (especially those of the dorsum of the wrist or ankle) and, in many cases, cellulitis recurs.
If lymphedema management starts during this stage, reduction can still occur. Even in extreme cases, with proper care and patient adherence to treatment, lymphostatic elephantiasis can be reduced so the leg is a normal or near-normal size.
Assessment and diagnosis
A thorough physical examination is the gold standard for diagnosing lymphedema. A complete patient history, body-systems review, inspection, and palpation can help determine if edema is lymphedema.
Clinically, the only test with proven reliability and validity in diagnosing lymphedema is the Stemmer sign. Fibrotic changes associated with lymphedema can lead to thickened skin over the proximal phalanges of the toes or fingers. If you can’t tent or pinch the skin on the involved extremity, lymphedema is present (a positive Stemmer sign). However, a negative finding (soft, pliable tissue) doesn’t rule out lymphedema because the condition may be in an early stage, before tissue proliferation and fibrosis have set in.
Management
Although incurable, lymphedema can be managed successfully through CDT. This approach involves proper identification of lymphedema, manual lymph drainage, skin and nail care, patient education, compression, and exercise.
CDT has two phases:
• Phase I, the intensive phase, continues until the extremity has decongested or reached a plateau. The clinician provides treatments and educates the patient about all aspects of CDT to prepare him or her for phase II. Phase I can last several weeks to several months depending on lymphedema severity.
• Phase II, the maintenance phase, begins once the extremity has decongested or plateaued. This phase still focuses on CDT, but now the patient, not the clinician, is responsible for all care. The goal is to reduce limb size while enabling the patient to become self-sufficient in managing lymphedema. Although CDT can bring significant improvements in limb size, skin quality, and function, patients must remember that phase II continues lifelong. Be sure to provide education about ongoing self-management strategies.
Lipedema: The disease they call “fat”
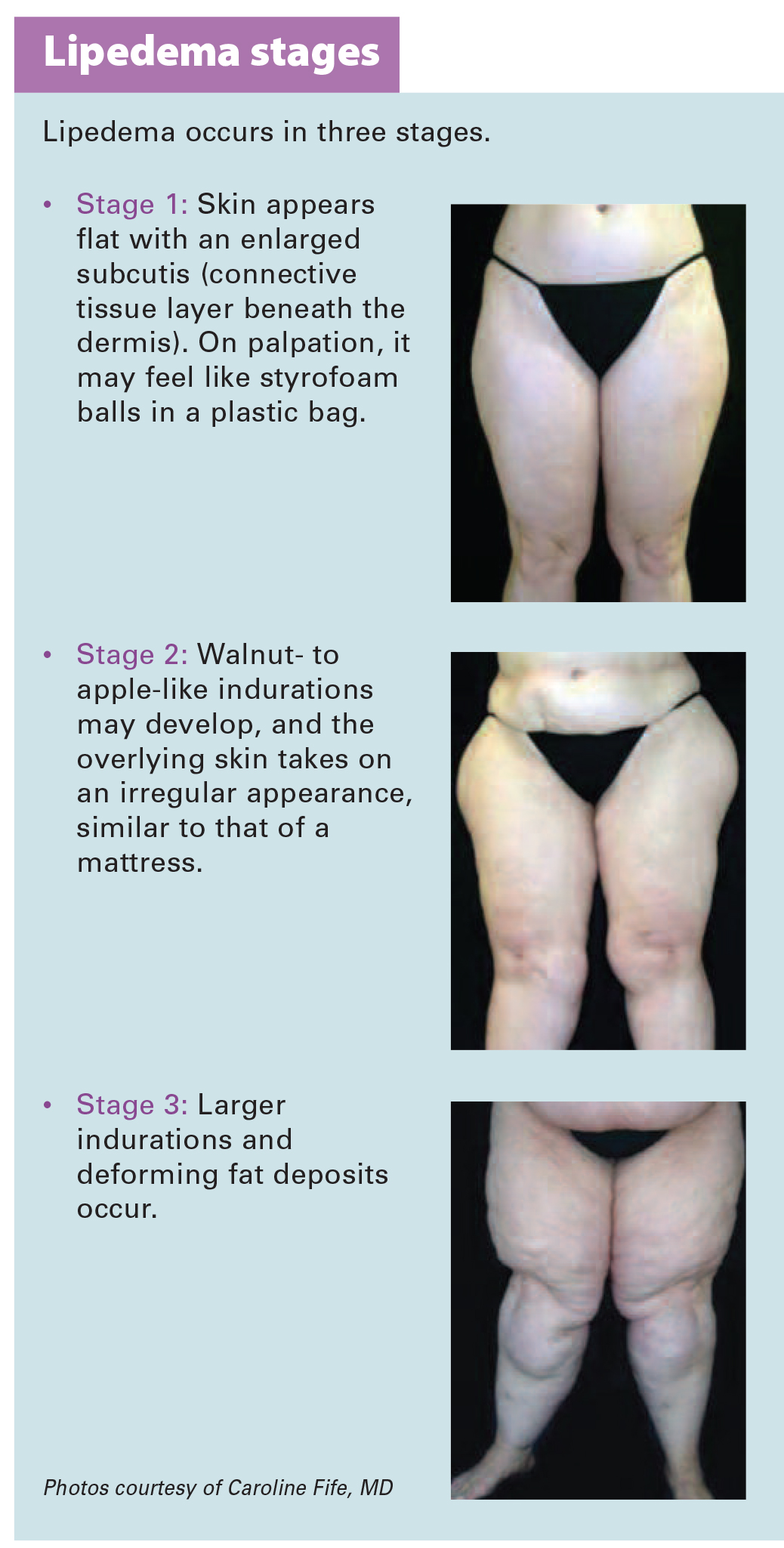
Lipedema is a painful disorder of fat deposition. Pathologic deposition of fatty tissue (usually below the waist) leads to progressive leg enlargement. Like lymphedema, lipedema is incurable but manageable. Unless managed properly, lipedema can reduce mobility, interfere with activities of daily living, and lead to secondary lymphedema. (See Lipedema stages.)
{kind=link}
Lipedema commonly is misdiagnosed as lymphedema. However, lymphedema involves protein-rich fluid, whereas lip edema is a genetically mediated fat disorder. Because lipedema resists diet and exercise, it can lead to psychosocial complications. Lipedema occurs almost exclusively in women; typically, onset occurs between puberty and age 30. One unpublished epidemiologic study puts lip edema incidence in females at 11%. Some patients have a combination of lipedema and lymphedema. (See Viewing lipolymphedema.)
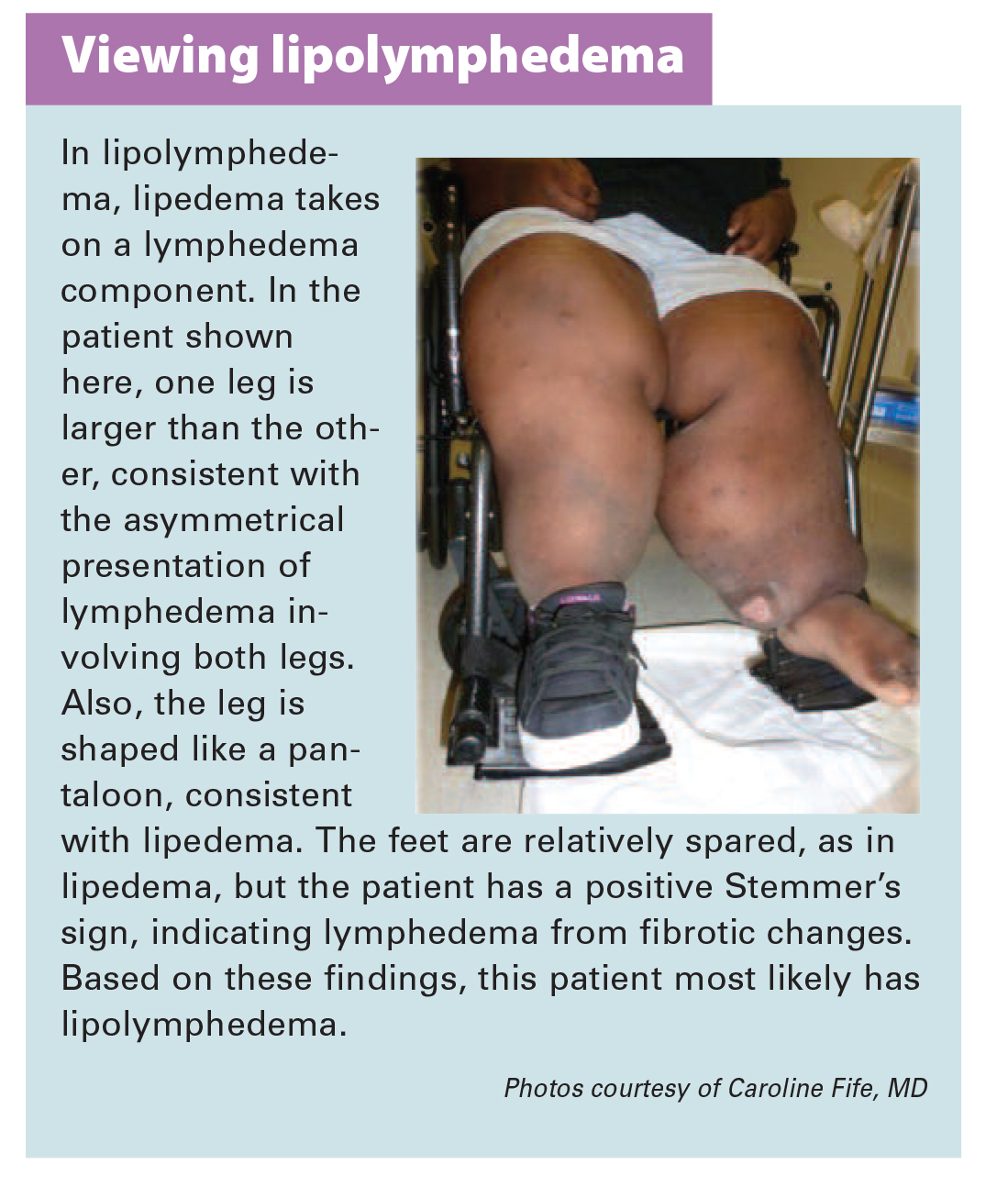{kind=link}
Assessment and diagnosis
As with lymphedema, lipedema diagnosis rests on clinical presentation. Lipedema characteristics include bilateral and symmetrical involvement, absence of pitting (because lipedema isn’t a fluid disorder), soft and pliable skin, and filling of the retromalleolar sulcus (called the fat pad sign.)
Key signs and symptoms include:
• feeling of heaviness in the legs (aching dysesthesia)
• easy bruising
• sensitivity to touch (called “painful fat syndrome”)
• orthostatic edema
• oatmeal-like changes to skin texture.
Nearly half of lipedema patients are overweight or obese, but many appear of normal weight from the waist up. Essentially, the upper and lower extremities don’t match. The lower extremities typically show fatty deposits extending from the iliac crest to the ankles, sparing the feet. (See Lipedema patterns.)
Management
Lipedema is best managed through weight control, as additional weight gain through adipose tissue tends to deposit in the legs. For patients with concomitant lymphedema (lipolymphedema), modified CDT helps reduce and manage lymphatic compromise. To address excess fat deposition, newer “wet” liposuction techniques have proven beneficial. These techniques gently detach adipose cells from the tissue, helping to preserve connective tissue and lymphatic vessels.
Know what to look for
In both lymphedema and lipedema, early identification and proper diagnosis are key. (See Differentiating lymphedema and lipedema.) A thorough history and physical exam will likely lead to an accurate diagnosis, if clinicians know what to look for. Proper diagnosis and treatment can prevent expensive and ineffective interventions, which can negatively affect both the patient’s condition and psychological well being.
Heather Hettrick is an associate professor at Nova Southeastern University, Department of Physical Therapy in Fort Lauderdale, Florida.
Selected references
Fat Disorders Research Society. Lipedema description.
Fife CE, Maus EA, Carter MJ. Lipedema: a frequently misdiagnosed and misunderstood fatty deposition syndrome. Adv Skin Wound Care. 2010;23(2):81-92
Herbst KL. Rare adipose disorders (RADS) masquerading as obesity. Acta Pharmacol Sin. 2012;33(2):155-72.
National Lymphedema Network. Position papers.
Schmeller W, Hueppe M, Meier-Vollrath I. Tumescent liposuction in lipoedema yields good long-term results. Br J Dermatol. 2012;166(1):161-8.
Zuther J. A closer look at lipedema and the effects on the lymphatic system. December 13, 2012. lymphedemablog.com/2012/12/13/a-closer-look-at-lipedema-and-the-effects-on-the-lymphatic-system/
Zuther J. Stages of lymphedema. October 3, 2012.
Read MoreInstill instead: Negative pressure wound therapy with instillation for complex wounds

Negative pressure wound therapy (NPWT) uses negative pressure to draw wound edges together, remove edema and infectious material, and promote perfusion and granulation tissue development. The tissue stretch and compression created by negative pressure during NPWT promotes tissue perfusion and granulation tissue development through angiogenesis, cellular proliferation, fibroblast migration, increased production of wound healing proteins, and reduction of wound area. NPWT has been used to improve healing in a variety of wounds, including traumatic injuries, surgical wounds, pressure ulcers, diabetic foot ulcers, and venous stasis ulcers. (more…)
Read MoreNutritional considerations in patients with pressure ulcers

Optimizing nutritional status is a key strategy both in preventing and managing pressure ulcers. In patients across all care settings, compromised nutrition— as from poor intake, undesired weight loss, and malnutrition—increases the risk of pressure ulcers. It contributes to altered immune function, impaired collagen synthesis, and decreased tensile strength. In many cases, malnutrition also contributes to wound chronicity and increases the risk for delayed and impaired wound healing. In patients with chronic wounds, such as pressure ulcers, a chronic inflammatory state can induce catabolic metabolism, malnutrition, and dehydration. (more…)
Read MoreA collaborative approach to wound care and lymphedema therapy: Part 1
Role of rehab in wound care
By Bill Richlen, PT, WCC, DWC, and Denise Richlen, PT, WCC, DCCT
How many times have you heard someone say, “I didn’t know PTs did wound care”? Statements like this aren’t uncommon. The role of physical therapists (PTs), occupational therapists, and speech therapists in wound care is commonly misunderstood by and even a mystery to many clinicians. Sometimes the therapists themselves are confused about reimbursement or what their role on the wound care team can be. (more…)
Read MoreMore from The Buzz Report: A wound care clinician’s best friend
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Keeping clinicians up to date on clinical knowledge is one of the main goals of the Wild On Wounds (WOW) conference,held each September in Las Vegas. Each year, I present the opening session of this conference, called “The Buzz Report,”which focuses on the latest-breaking wound care news—what’s new, what’s now, and what’s coming up. I discuss innovative new products, practice guidelines, resources, and tools from the last 12 months in skin, wound, and ostomy management. (more…)
Read More