Factors affecting medication adherence in patients with diabetes identified
Factors associated with better adherence to antidiabetic medications taken by patients with diabetes include older age, male sex, higher education, higher income, use of mail-order vs. retail pharmacies, primary care vs. nonendocrinology specialist prescribers, higher daily total pill burden, and lower out-of-pocket costs. (more…)
Below are resources you may find helpful to your practice.
AHRQ’s Safety Program for Nursing Homes: On-Time Prevention
The Agency for Healthcare Research and Quality (AHRQ) has established “AHRQ’s Safety Program for Nursing Homes: On-Time Prevention,” designed to improve long-term care by turning daily documentation into useful information that enhances clinical care planning.
On-Time uses electronic medical records to develop weekly reports that identify residents at risk for common adverse events in nursing homes to help clinical staff intervene early. Facilitators help the team integrate these reports into clinical decision making to improve care planning.
For each adverse event, the website provides a description of the reports and suggested meetings and huddles where the reports may be used, the functional specifications for programming the reports, description of implementation tools, and a 2-day training curriculum for facilitators.
Sleep times guidelines
The National Sleep Foundation has issued new recommendations for appropriate sleep durations. Check below to see if your patients—and you—are getting enough sleep:
The free app includes treatment videos and coupons to help patients save on wound care treatment supplies. The app is available for download on iTunes.
In 2014, more than 8,000 new articles related to wound healing were added to the PubMed online database and hundreds of new patents for topical wound formulations were filed. Staying up-to-date with the latest and greatest findings and products can be challenging. We all lead busy lives, and our demanding work schedules and home responsibilities can thwart our best intentions. Although we know it’s our responsibility to stay abreast of changes in our field, we may feel overwhelmed trying to make that happen. (more…)
Each issue, Apple Bites brings you a tool you can apply in your daily practice.
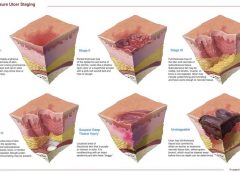
Measurement of wounds is an important component of wound assessment and provides baseline measurements, enables monitoring of healing rates, and helps distinguish among wounds that are static, deteriorating, or improving. All alterations in skin integrity, including those caused by ulcers, venous ulcers, arterial ulcers, neuropathic ulcers, incision lines, grafts, donor sites, abscesses, and rashes should be measured when they’re discovered and at intervals thereafter, based on institutional policy. (more…)
By Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA
Note From the Editor: This is the second of two articles on maggot therapy. The first article appeared in our July/August 2014 issue, Read part 1 here.
Whether your practice is an acute-care setting, a clinic, home care, or elsewhere, maggot debridement therapy (MDT) can prove to be a useful tool in wound care. But setting up any new program can meet resistance—and if you seek to establish a maggot therapy program, expect to meet significant resistance. By arming yourself in advance, you can achieve your goal more easily. This article covers all the bases to help you get your maggot therapy program off the ground. (more…)
By: Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA
Maggot therapy is the controlled, therapeutic application of maggots to a wound. Simple to use, it provides rapid, precise, safe, and powerful debridement. Many wound care professionals don’t provide maggot therapy (also called wound myiasis) because they lack training. But having maggot therapy technology available for patients adds to your capabilities as a wound care provider. (more…)
The ability to understand or “read” lower-extremity redness in your patient is essential to determining its cause and providing effective treatment. Redness can occur in multiple conditions—hemosiderin staining, lipodermatosclerosis, venous dermatitis, chronic inflammation, cellulitis, and dependent rubor. This article provides clues to help you differentiate these conditions and identify the specific cause of your patient’s lower-extremity redness. (more…)
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)
New wound-swabbing technique detects more bacteria
The new Essen Rotary swabbing technique takes a few seconds longer to perform than traditional techniques, but improves bacterial count accuracy in patients with chronic leg ulcers, according to a study published by Wounds International.
“Evaluation of the Essen Rotary as a new technique for bacterial swabs: Results of a prospective controlled clinical investigation in 50 patients with chronic leg ulcers” reports that Essen Rotary detected significantly more bacteria compared to standard techniques and was the only one to identify five patients with methicillin-resistant Staphylococcus aureus (MRSA), compared to three detected by other techniques.
The Essen Rotary technique samples a larger surface area of the wound, which is beneficial for detecting MRSA.
“The Essen Rotary may become the new gold standard in routinely taken bacteriological swabs especially for MRSA screenings in patients with chronic leg ulcers,” the study authors write.
Reducing HbA1c by less than 1% cuts cardiovascular risk by 45% in patients with type 2 diabetes
A study presented at the American Diabetes Association 72nd Scientific Sessions found lowering HbA1c an average of 0.8% (from a mean of 7.8% to 7.0%, the treatment target) reduced the risk of cardiovascular death by 45% in patients with type
2 diabetes.
The absolute risk of mortality from a cardiovascular event was 9.9 events per 1,000 person-years in patients with decreasing HbA1c compared to 17.8 events in patients with stable or increasing HbA1c.
“HbA1c reduction and risk of cardiovascular diseases in type 2 diabetes: An observational study from the Swedish NDR” examined data from 18,035 patients in the Swedish National Diabetes Register.
CMS revises hospital, nursing home comparison websites
The Centers for Medicare & Medicaid Services (CMS) has enhanced two websites designed to help the public make informed choices about their health care. Hospital Compare and Nursing Home Compare now have better navigation and new comparison tools. The two sites include data on quality measures, such as frequency of hospital-acquired infections, and allow the user to compare hospitals on these measures.
Improvements include easy-to-use maps for locating hospitals, a new search function that enables the user to input the name of a hospital, and glossaries that are easier to understand. It’s now also possible to access the data on the sites through mobile applications.
CMS maintains the websites, which are helpful for anyone who wants to compare facilities, not just patients on Medicare or Medicaid.
For more information, read the article in Healthcare IT News.
IOM releases report on accelerating new drug and diagnostics development
The Institute of Medicine (IOM) released “Accelerating the development of new drugs and diagnostics: Maximizing the impact of the Cures Acceleration Network—Workshop Summary.” The report is a summary of a forum that brought together members of federal government agencies, the private sector, academia, and advocacy groups to explore options and opportunities in the implementation of Cures Acceleration Network (CAN). The newly developed CAN has the potential to stimulate widespread changes in the National Institutes of Health and drug development in general.
Focus on individualized care—not just reducing swelling—in lymphedema patients
As a result of two extensive literature reviews, a researcher at the University of Missouri found that emphasizing quality of life—not just reducing swelling—is important for patients with lymphedema. Many providers and insurance companies base treatment on the degree of edema, but the volume of fluid doesn’t always correspond with the patients’ discomfort. Instead, an individualized plan of care should be developed.
The researchers found that Complete Decongestive Therapy (CDT), a comprehensive approach for treating lymphedema that includes skin and nail care, exercise, manual lymphatic drainage, and compression, may be the best form of specialized lymphedema management. For more information about CDT, watch for the November/December issue of Wound Care Advisor.
Plague case in Oregon draws national attention
An article about a case of the plague in Oregon has appeared on Huffington Post. A welder contracted the disease as a result of unsuccessfully removing a mouse from a stray cat’s mouth. Part of his hands have, in the words of the article, “darkened to the color of charcoal.” Later tests confirmed the cat had the plague.
Plague cases are rare in the United States. According to the Centers for Disease Control and Prevention, an average of 7 human cases are reported each year, with a range of 1 to 17 cases. Antibiotics have significantly reduced morality. About half of cases occur in people ages 12 to 45.
Use of negative pressure wound therapy with skin grafts
“Optimal use of negative pressure wound therapy for skin grafts,” published by International Wound Journal, reviews expert opinion and scientific evidence related to the use of negative pressure wound therapy with reticulated open-cell foam for securing split-thickness skin grafts.
The article covers wound preparation, treatment criteria and goals, economic value, and case studies. The authors conclude that the therapy has many benefits, but note that future studies are needed “to better measure the expanding treatment goals associated with graft care, including increased patient satisfaction, increased patience compliance and improved clinical outcomes.”
Mechanism for halting healing of venous ulcers identified
Researchers have identified that aberrantly expressed microRNAs inhibit healing of chronic venous ulcers, according to a study in The Journal of Biological Chemistry.
Six microRNAs were plentiful in 10 patients with chronic venous ulcers. The microRNAs target genes important in healing the ulcers. In an article about the study, one of the researchers said, “The more we know about the molecular mechanisms that contribute to [the development of venous ulcers], the more we can rationally develop both diagnostic tools and new therapies.”
Hemodialysis-related foot ulcers not limited to patients with diabetes
Both patients with diabetes and those without are at risk for hemodialysis-related foot ulcers, according to a study published by International Wound Journal.
Researchers assessed 57 patients for ulcer risk factors (peripheral neuropathy, peripheral arterial disease, and foot pathology, such as claw toes, hallux valgus, prominent metatarsal heads, corns, callosities, and nail pathologies) at baseline, and noted mortality 3 years later.
In all, 79% of patients had foot pathology at baseline, and 18% of patients without diabetes had peripheral neuropathy. Peripheral arterial disease was present in 45% of diabetic and 30% of nondiabetic patients. Nearly half (49%) of patients had two or more risk factors. Only 12% of patients had no risk factors. The presence of peripheral arterial disease and peripheral neuropathy increased risk of mortality.
The authors of “Prevalence of risk factors for foot ulceration in a general haemodialysis population” state that the high prevalence of risk factors in nondiabetic patients indicates that they are at risk for developing foot ulcers.
Study identifies risk factors for mortality from MRSA bacteremia
A study in Emerging Infectious Diseases found that older age, living in a nursing home, severe bacteremia, and organ impairment increase the risk of death from methicillin-resistant Staphylococcus aureus (MRSA) bacteremia.
Consultation with a specialist in infectious disease lowers the risk of death, and MRSA strain types weren’t associated with mortality.
“Predicting risk for death from MRSA bacteremia” studied 699 incidents of blood infection from 603 patients who had MRSA bacteremia.
Venous leg ulcers are the most common cause of lower extremity ulcers, affecting 1% of the U.S. population (approximately 3 million people). Annual treatment costs for venous disease in this country range from $1.9 to $3.5 billion.
The gold standard for venous ulcer treatment includes moist wound healing and compression therapy. But before compression wraps are applied, we must determine if adequate arterial blood flow exists—or consequences could be life-threatening.
Raise your hand if you know what ABI is. Now raise your hand if you routinely obtain ABIs for patients. I’ve been asking these questions at wound care seminars around the country for the last 10 years, and the answers are always the same:
Between 50% and 95% of the audience know what an ABI is, but only 1% to 2% say they perform the ABI test. My next question is “Why not?”
The ABI (ankle brachial index) is a noninvasive screening test performed with a handheld vascular Doppler and a blood pressure cuff. This simple test helps determine if you can safely apply compression therapy, aids diagnosis of peripheral arterial disease, and even helps monitor the efficacy of therapeutic interventions.
Numerous standard practice guidelines from various organizations recommend obtaining ABIs to determine arterial blood flow. These organizations include the American College of Cardiology, American Heart Association, American Diabetes Association, Society for Vascular Nursing, Wound Ostomy Continence Nurses, Society for Vascular Medicine, U.S. Preventive Services Task Force, and World Union of Wound Healing Societies.
Instructions for most compression therapy products include indications for Doppler ABI readings above 0.8. So if you don’t get an ABI reading, how can you safely apply these products? A report by Allie and colleagues found that more than 50% of lower extremity amputations occur without previous vascular testing of any type, including ABI.
So why aren’t more practitioners obtaining ABIs? The leading answer: “We don’t have a Doppler.” I understand the dilemma of not having equipment or the funds to get the equipment. But do we want to tell a patient who has just lost her leg, “Oh, sorry. We didn’t have a Doppler”?
It’s our responsibility and duty as WCCs, wound care experts, and health care clinicians to ensure we provide the highest standard of care for patients with venous leg ulcers. So communicate with management, explaining what you need and why you need it. Work with your medical supply company for an extended payment plan. Hold a fundraiser. Consider using the alternative Lanarkshire Oximetry Index procedure. Or send the patient to a wound clinic or other healthcare provider who can perform the test.
It’s time to step it up and take greater accountability—and to no longer use the excuse “We don’t have a Doppler.”
Donna Sardina, RN, MHA, WCC, CWCMS, DWC Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Selected references
Allie DE, Hebert CJ, Lirtzman MD, et al. Critical limb ischemia: a global epidemic. A critical analysis of current treatment unmasks the clinical and economic costs of CLI. EuroIntervention. 2005; 1(1):75-84. http://www.ncbi.nlm.nih.gov/pubmed/
19758881. Accessed June 4, 2012.
Lazarus GS, Cooper DM, Knighton DR, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch Dermatol. 1994; 130(4):489-493. http://www.ncbi.nlm.nih.gov/pubmed/8166487. Accessed June 4, 2012.
Olin JW, Allie DE, Belkin M, et al. ACCF/AHA/ACR/SCAI/SIR/SVM/SVN/SVS 2010 performance measures for adults with peripheral artery disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures, the American College of Radiology, the Society for Cardiac Angiography and Interventions, the Society for Interventional Radiology, the Society for Vascular Medicine, the Society for Vascular Nursing, and the Society for Vascular Surgery (Writing Committee to Develop Performance Measures for Peripheral Artery Disease). J Am Coll Cardiol. 2010;56(25):2147-2181. http://content.onlinejacc
.org/cgi/content/full/j.jacc.2010.08.606. Accessed June 4, 2012.
O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev. 2010;(1):CD003557. http://www.ncbi.nlm.nih.gov/pubmed/20091548. Accessed June 4, 2012.
Rooke TW, Hirsch AT, Misra S, et al; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society for Vascular Medicine; Society for Vascular Surgery. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58(19):2020-2045. http://
content.onlinejacc.org/cgi/content/full/j.jacc.2011.08.023v1. Accessed June 4, 2012.
Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insufficiency and venous leg ulceration. J Am Acad Dermatol. 2001;44(3):401-421. http://www.ncbi.nlm.nih.gov/pubmed/11209109. Accessed June 4, 2012.
World Union of Wound Healing Societies. Principles of best practice:. Compression in venous leg ulcers: a consensus document. London: MEP Ltd; 2008. www.woundsinternational.com/pdf/content_25.pdf. Accessed June 4, 2012.
Study finds ultrasound therapy improves venous ulcer healing
In a study of 10 venous ulcers not responding to treatment, the use of noncontact ultrasound significantly reduced the wound area over 4 weeks of treatment.
It has been unclear exactly how ultrasound achieves its positive results. The
authors of “A prospective pilot study of ultrasound therapy effectiveness in refractory venous leg ulcers,” an article published online on February 1 by the International Wound Journal, found that patients treated with ultrasound and compression therapy had reduced inflammatory cytokines and bacterial counts, but the reduction wasn’t statistically significant.
The study found another important benefit for patients-reduced pain.
Serum albumin is not a goodindicator of nutritional status
Traditionally the standard of practice for wound care patients has been to review albumin blood levels as a measure of nutritional status and the effect of nutritional interventions. But as noted in The Role of Nutrition in Pressure Ulcer Prevention and Treatment: National Pressure Ulcer Advisory Panel White Paper, recent studies show that hepatic proteins (albumin, transthyretin, and transferrin) correlate with the severity of an underlying disease, not nutritional status. Moreover, many factors can alter albumin levels even when protein intake is adequate, including infection, acute stress, surgery, cortisone excess, and hydration status.
For these reasons, the National Pressure Ulcer Advisory Panel (NPUAP) and the Academy of Nutrition and Dietetics (previously known as The American Dietetic Association) recommend against using serum proteins as a nutritional assessment tool. Evaluation of lab values is just one part of the nutritional assessment process and should be considered along with other factors such as ensuring that the patient receives what is prescribed; daily food/fluid intake; changes in weight status, diagnosis, and medications; and clinical improvement in the wound.
The mean number of serious comorbid conditions was 1.8.
The most common comorbid conditions were obesity/overweight (71.3%), cardiovascular or peripheral vascular disease (51.3%), and diabetes (46.8%).
Nearly two-thirds (65.8%) of wounds healed, with an average healing time
of 15 weeks.
In half of the wounds that healed, patients received only moist wound care and no advanced therapeutics.
The mean cost for wound healing was $3,927.
The authors of the article, published in March’s Wounds, analyzed 5,240 patients with 7,099 wounds in 59 hospital-based outpatient wound centers in 18 states over 5 years.
LOI index comparable to ABI for assessing PAD in patients with type 2 diabetes
The pilot study “Lanarkshire Oximetry Index as a diagnostic tool for peripheral arterial disease in type 2 diabetes,” published in Angiology, compared the gold standard ankle brachial index (ABI) to the Lanarkshire Oximetry Index (LOI) in 161 patients with type 2 diabetes. Researchers assessed the patients for peripheral artery disease (PAD, defined as ABI < 0.9) using both ABI and LOI.
Using a LOI cut-off value of 0.9., the sensitivity and specificity for PAD were 93.3% and 89.1%, respectively. The study concluded that LOI is a “potentially useful alternative diagnostic test for PAD” in patients with type 2 diabetes.
LOI is a noninvasive procedure similar to ABI; both indices indicate whether it’s safe to apply compression to the limb of a patient who has lower leg ulceration or venous hypertension. With LOI, a pulse oximeter is used in place of a hand-held Doppler to determine the index.
Start planning for World Diabetes Day
It’s not too early to begin planning for World Diabetes Day, November 14. Started by the World Health Organization (WHO) and the International Diabetes Federation (IDF), the day is designed to raise global awareness of diabetes.
Access materials, including posters, a campaign book, and the Word Diabetes Day Logo, from IDF’s website, which also has activity ideas.
WHO estimates that more than 346 million people worldwide have diabetes, and the number is expected to double by 2030. World Diabetes Day is celebrated on November 14 to mark the birthday of Frederick Banting who, along with Charles Best, was instrumental in the discovery of insulin in 1922.
Guidelines for PAD in patients with diabetes and foot ulceration published
February’s issue of Diabetes/Metabolism Research and Reviews includes “Specific guidelines for the diagnosis and treatment of peripheral arterial disease in a patient with diabetes and ulceration of the foot 2011,” which is based on two companion International Working Group on the Diabetic foot papers. The guidelines state that if a patient’s PAD is impairing wound healing, revascularization through bypass or endovascular technique must be considered except in a few cases such as severely frail patients. Limb salvage rates after revascularization procedures are about 80-85%, and there is ulcer healing in > 60% at 12 months.
Other points of particular interest to wound care professionals:
Patients with PAD and a foot infection are at high risk for major limb amputation, so should be treated as a “medical emergency”, preferably within 24 hours.
Half of patients with diabetes, a foot ulcer, and PAD die within 5 years because of higher cardiovascular morbidity and mortality. Cardiovascular risk management should include “support for cessation of smoking, treatment of hypertension, and prescription of a statin as well as low-dose aspirin or clopidrogel.