Submit your manuscript electronically as an MS Word file. Follow these guidelines:
At the top of the first page of the document, place the article title, your initials (not your name), and the date.
DO NOT include extra hard returns between lines or paragraphs, extra spaces between words, or any special coding.
Send a separate cover letter that includes your name; credentials; position; address; home, cell, and work telephone numbers; email address; and your employer’s name, city, and state.
If your manuscript contains clinical information and we believe it has publication potential, we will send it out for blind peer review (neither you nor the reviewers will know who wrote the article). All manuscripts also receive an internal editorial review. After the review, we’ll let you know whether the manuscript has been accepted, accepted pending revisions, or declined.
If we accept your manuscript for publication, we’ll ask you to sign an agreement that gives HealthCom Media (publisher of Wound Care Advisor) the rights to your article so that it can be published. Each author must sign a separate agreement.
Your article will go through our in-house editorial process, where professional editors ensure consistency with our editorial style. You will have a chance to review the edited version before it’s published.
We will email you if we decide not to publish your manuscript.
Thank you for considering publishing in Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy, the official. If you have any questions, please email: Cynthia Saver, RN, MS, at [email protected] or [email protected].
Get access to original and peer-reviewed clinical content dealing with chronic wounds and ostomy management issues. Monthly frequency. Sign up for the Wound Care Advisor email newsletter today!
Nearly all clinicians know exercise is good for our physical and mental health. But incorporating it into our busy lives can be a challenge. The only types of exercise some clinicians have time for are working long shifts, juggling life’s demands, balancing the books, jumping on the bandwagon, climbing the ladder of success, and skipping meals.
Clinicians are in a unique position to help patients change their behavior to improve their health. Ironically, the first behavior clinicians need to change is to work toward improving our own exercise habits. (more…)
Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement you’d feel.
What if you had to live through this experience repeatedly? That’s what many elderly people go through, suffering with skin tears through no fault of their own. Some go on to develop complications.
A skin tear is a traumatic wound caused by shear, friction, or blunt-force trauma that results in a partial- or full-thickness injury. Skin tears are painful because the precipitating injury commonly involves the dermis, which is rich with nerve endings. (more…)
Using a checklist form to document wound care can make the task easier and faster—and help ensure that you’ve captured all pertinent data needed for assessment, reimbursement, and legal support. But the form itself may not be comprehensive; some important fields may be missing.
Recently, we at Wound Care Advisor received a question from a clinician who was having trouble deciding how to code a patient’s wound in her hospital’s electronic health record (EHR). Her patient’s specific wound and tissue types weren’t available options in the dropdown menu on the software system. Luckily, on investigating, we discovered her system provided the option to override the checklist and add comments in a notes section. (more…)
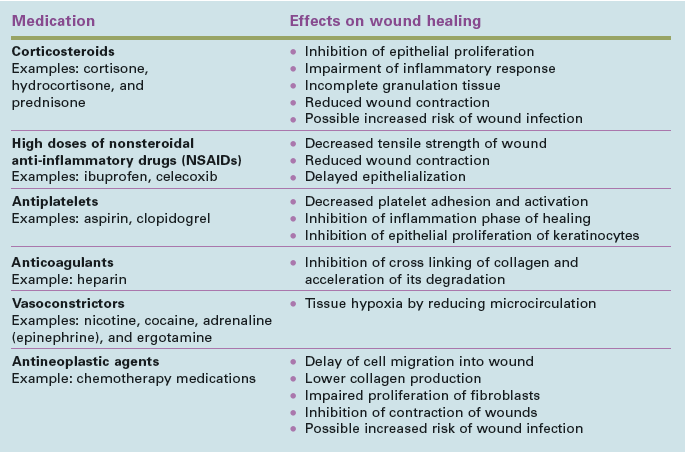
Assessment and care planning for wound healing should include a thorough review of the individual’s current medications to identify those that may affect healing outcomes. Clinicians must then weigh the risks and benefits of continuing or discontinuing the medications. In some cases, the risk of discontinuing the medication outweighs the importance of wound healing, so the goal of the care plan should be adjusted to “maintain a wound” instead of “healing.” (more…)
A fundamental rule of wound care is to treat the “whole” patient, not just the “hole” in the patient. To do this, we need to focus on a holistic
approach to healing, which means evaluating everything that’s going on with the patient—from nutrition, underlying diseases, and medications to activity level, social interactions, and even sleep patterns.
We know that as specialists, we’re expected to do all of these things. But in the real world, we can’t be specialists in all areas. That’s where the team concept comes in. In fact, the team approach is imperative for helping us heal our patients’ wounds and achieve our overall goal of improving patient outcomes. (more…)
The authors of the article explain evidence-based practice and provide useful definitions for key terms. They then provide a list of eight questions to use when evaluating SRs and practical tips such as how to search for SR and MA studies. The article finishes with a list of eight interventions supported by the most evidence: hydrocolloidal dressings, honey, biosynthetic dressings, iodine complexes, silver compounds, hydrogels, foam dressings, and negative pressure wound therapy. (more…)
Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of cutaneous candidiasis.
Cutaneous candidiasis is an infection of the skin caused by the yeast Candida albicans or other Candida species. Here’s a snapshot of this condition. (more…)
A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI), a unique staging category for a pressure ulcer. Otherwise, a clinician might think a pressure ulcer is getting worse instead of the change being the normal progression of a pressure ulcer that is presenting as a DTI.
By: Donna Sardina, RN, MHA, WCC, CWCMS What do the Los Angeles Lakers, Green Bay Packers, Montreal Canadiens, and New York Yankees have in common? All three have “three-peated”, meaning they have won three consecutive championships. This year, we at Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy (NAWCO), mark our own three-peat—our…
Mild compression diabetic socks safe and effective for lower extremity edema Diabetic socks with mild compression can reduce lower extremity edema in patients with diabetes without adversely affecting arterial circulation, according to a randomized control trial presented at the American Diabetes Association 75th Scientific Sessions Conference.
The resources below will help you address issues in your practice. NPUAP position statement on hand check for bottoming out Use of the hand check to determine “bottoming out” of support systems should be limited to static air overlay mattresses, according to a position statement from the National Pressure Ulcer Advisory Panel (NPUAP).
By Jennifer Oakley, BS, RN, WCC, DWC, OMS It’s time again for annual staff education, and you, the certified wound clinician, need to teach the staff at your organization. You dream of staff entering a state-of-the-art classroom with computers at each station, mannequins, wound anatomy models, and enough products for each student to do hands-on demonstrations. But when you open…
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI),…
By Cindy Barefield, BSN, RN-BC, CWOCN Like many hospitals, Houston Methodist San Jacinto Hospital uses national benchmarks such as the National Database of Nursing Quality Indicators (NDNQI®) to measure quality outcomes. Based on benchmark reports that showed an increased trend of pressure ulcers in critically ill patients in our hospital, the clinical nurses in our Critical Care Shared Governance Unit-Based…
By Beth Hoffmire Heideman, MSN, RN No one wants an ostomy, but sometimes it’s required to save a patient’s life. As ostomy specialists, our role is to assess and intervene for patients with a stoma or an ostomy to enhance their quality of life. We play an active role in helping patients perform self-care for their ostomy and adjust to…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Exudate (drainage), a liquid produced by the body in response to tissue damage, is present in wounds as they heal. It consists of fluid that has leaked out of blood vessels and closely resembles blood…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Medical gauze, a bleached white cloth or fabric used in bandages, dressings, and surgical sponges, is the most widely used wound care dressing. Commonly known as “4×4s,” gauze is made from fibers of cotton, rayon,…
By Gail Rogers Hebert, MS, RN, CWCN, WCC, DWC, OMS, LNHA The World Health Organization defines palliative care as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other…
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson, PhD, RN; and Keith Swanson, MD Cellulitis is an acute, painful, and potentially serious spreading bacterial skin infection that affects mainly the subcutaneous and dermal layers. Usually of an acute onset, it’s marked by redness, warmth, swelling, and tenderness. Borders of the affected skin…










{kind=link}