Missed care, a relatively new concept in the medical community, refers to any part ofrequired patient care that is omitted of delayed. It’s not the same as a mistake or error, but like them, missed care can negatively affect patient outcomes.
I want to share the case of a patient admitted into home health care for wound care. The case includes several areas of missed care from many different different sources. (more…)
Are you making connections that benefit your career? Are you comfortable starting a conversation at a networking session? Do you know how to exit a conversation gracefully when it’s time to move on?
These are questions and concerns many clinicians share. Career success takes more than clinical expertise, management savvy, and leadership skills. Networking can be the critical link to success. This article helps you improve your networking skills by focusing on what to do before, during, and after a networking opportunity. (more…)
Dermatologic difficulties: Skin problems in patients with chronic venous insufficiency and phlebolymphedema By Nancy Chatham, RN, MSN, ANP-BC, CWOCN, CWS; Lori Thomas, MS, OTR/L, CLT-LANA; and Michael Molyneaux, MD
Skin problems associated with chronic venous insufficiency (CVI) and phlebolymphedema are common and often difficult to treat. The CVI cycle of skin and soft tissue injury from chronic disease processes can be unrelenting. If not properly identified and treated, these skin problems can impede the prompt treatment of lymphedema and reduce a patient’s quality of life.
This article reviews skin problems that occur in patients with CVI and phlebolymphedema and discusses the importance of using a multidisciplinary team approach to manage these patients. (more…)
By Nancy Collins, PhD, RD, LD/N, FAPWCA, and Allison Schnitzer
Nutrition is a critical factor in the wound healing process, with adequate protein intake essential to the successful healing of a wound. Patients with both chronic and acute wounds, such as postsurgical wounds or pressure ulcers, require an increased amount of protein to ensure complete and timely healing of their wounds.
Elderly patients with wounds pose a special challenge because of their decreased lean body mass and the likelihood of chronic illnesses and insufficient dietary protein intake. To promote a full recovery, wound care clinicians must address the increased protein needs of wound patients, especially elderly patients. (more…)
Most of the wounds in the 154,644 patients were diabetic foot ulcers, venous leg ulcers, and pressure ulcers. The study authors note that debridement is a “key process” in wound bed preparation and starting the healing process.
The findings are congruent with previous studies and are based on an analysis of the largest wound data set to date. (more…)
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC
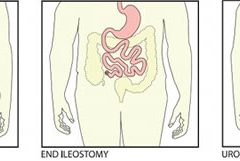
About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders.
A stoma has no sensory nerve endings and is insensitive to pain. Yet several complications can affect it, making accurate assessment crucial. These complications may occur during the immediate postoperative period, within 30 days after surgery, or later. Lifelong assessment by a healthcare provider with knowledge of ostomy surgeries and complications is important. (more…)
By Nancy Chatham, RN, MSN, ANP-BC, CCNS, CWOCN, CWS, and Lori Thomas, MS, OTR/L, CLT-LANA
An estimated 7 million people in the United States have venous disease, which can cause leg edema and ulcers. Approximately 2 to 3 million Americans suffer from secondary lymphedema. Marked by abnormal accumulation of protein-rich fluid in the interstitium, secondary lymphedema eventually can cause fibrosis and other tissue and skin changes. (more…)
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found that using hybrid 67Ga single-photon emission computed tomography and X-ray computed tomography (SPECT/CT) imaging combined with a bedside percutaneous bone puncture in patients with a positive scan is “accurate and safe” for diagnosing osteomyelitis in patients with diabetes who have a foot ulcer without signs of soft-tissue infection.
The new method, which avoids an invasive bone biopsy, has a sensitivity of 88% and a specificity of 93.6%. In the study of 55 patients, antibiotic treatment was avoided in 55% of suspected cases.
MRSA strains will likely continue to coexist in hospitals and communities
The strains of methicillin-resistant Staphylococcus aureus (MRSA) differ in the hospital and community settings, and both are likely to coexist in the future, according to a study in PLOS Pathogens.
C. difficile prevention actions fail to stop spread
Despite increasing activities to prevent the spread of Clostridium difficile, infection from C. difficile remains a problem in healthcare facilities, according to a survey of infection preventionists by the Association for Professionals in Infection Control and Epidemiology (APIC).
The survey found that 70% of preventionists have adopted additional interventions in their healthcare facilities since March 2010, but only 42% have seen a decline in C. difficile infection rates; 43% saw no decline.
A total of 1,087 APIC members completed the survey in January 2013. The survey also found that more than 92% of respondents have increased emphasis on environmental cleaning and equipment decontamination practices, but 64% said they rely on observation, rather than more accurate and reliable monitoring technologies, to assess cleaning effectiveness.
In addition, 60% of respondents have antimicrobial stewardship programs at their facilities, compared with 52% in 2010. Such programs promote the appropriate use of antibiotics, which can help reduce the risk of C. difficile infection.
Mast cells may not play significant role in wound healing
“Evidence that mast cells are not required for healing of splinted cutaneous excisional wounds in mice,” published in PLOS One, analyzed wound healing in three types of genetically mast-deficient mice and found they reepithelialized their wounds at rates similar to control mice. At the time of closure, the researchers found that scars in all the mice groups were similar in both “quality of collagen deposition and maturity of collagen fibers.” The findings fail to support the previously held belief that mast cells are important in wound healing.
Study identifies effective casting for diabetes-related plantar foot ulcers
Nonremovable casts that relieve pressure are more effective than removable casts or dressings alone for the treatment of plantar foot ulcers caused by diabetes, according to an analysis of clinical trials.
The authors of “Pressure-relieving interventions for treating diabetic foot ulcers,” published by The Cochrane Library, reviewed 14 randomized clinical trials that included 709 participants. Nonremovable pressure-relieving casts were compared to dressings alone, temporary therapeutic shoes, removable pressure-relieving devices, and surgical lengthening of the Achilles tendon.
The study also notes that when combined with Achilles tendon lengthening, nonremovable devices were more successful in one forefoot ulcer study than the use of a nonremovable cast alone.
Most studies were from the United States (five) and Italy (five), with Germany, the Netherlands, Australia, and India each contributing one study.
Prescriber preference drives use of antibiotics in long-term care
The study of 66,901 patients from 630 long-term care facilities found that 77.8%
received a course of antibiotics. The most common length (41%) was 7 days, but the length exceeded 7 days in 44.9% of patients. Patient characteristics were similar among short-, average-, and long-duration prescribers.
The study authors conclude: “Future trials should evaluate antibiotic stewardship interventions targeting prescriber preferences to systematically shorten average treatment durations to reduce the complications, costs, and resistance associated with antibiotic overuse.”
Electrophysical therapy may be helpful for diabetic foot ulcers
The authors of the study in International Wound Journal reviewed eight trials with a combined total of 325 patients. Five studies were on electrical stimulation, two on phototherapy, and one on ultrasound. Because of the small number of trials, the possibility of harmful effects can’t be ruled out, and the authors recommend “high-quality trials with larger sample sizes.”
Significant geographic variations in spending, mortality exist for diabetic patients with foot ulcers and amputations
The study in Journal of Diabetes and Its Complications found that higher spending wasn’t associated with a significant reduction in 1-year patient mortality. In addition, rates of hospital admission were associated with higher per capita spending and higher mortality rates for patients.
Home-based exercise program improves life for lymphedema patients
An individualized, home-based progressive resistance exercise program improves upper-limb volume and circumference and quality of life in postmastectomy patients with lymphedema, according to a study published in the Journal of Rehabilitation Research and Development.
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
To begin appropriate treatment for chronic venous insufficiency (CVI), clinicians must be able to make the correct diagnosis. Part 1 (published in the March-April edition) described CVI and its presentation. This article provides details of the CVI diagnosis (including the differential diagnosis from other diseases), disease classification to help assess the extent of CVI, diagnostic studies used to diagnose CVI, and various treatment options to “rescue” the patient from CVI. (more…)
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Chronic venous insufficiency (CVI) is the most common cause of lower extremity wounds. The venous tree is defective, incapable of moving all the blood from the lower extremity back to the heart. This causes pooling of blood and intravascular fluid at the lowest gravitational point of the body—the ankle.
This article has two parts. Part 1 enhances your understanding of the disease and its clinical presentation. Part 2, which will appear in a later issue, explores the differential diagnosis of similar common diseases, the role that coexisting peripheral artery disease (PAD) may play, disease classification of venous insufficiency, and a general approach to therapy.
The most common form of lower extremity vascular disease, CVI affects 6 to 7 million people in the United States. Incidence increases with age and other risk factors. One study of 600 patients with CVI ulcers revealed that 50% had these ulcers for 7 to 9 months, 8% to 34% had them for more than 5 years, and 75% had recurrent ulcers.
Thrombotic complications of CVI include thrombophlebitis, which may range from superficial to extensive. If the thrombophlebitis extends up toward the common femoral vein leaving the leg, proximal ligation may be needed to prevent clot extension or embolization.
Understanding normal anatomy and physiology
Lower extremity veins flow horizontally from the superficial veins to the perforating veins and then into the deep veins. Normally, overall venous blood flows vertically against gravity from the foot and ankle upward toward the inferior vena cava (IVC). This antigravity flow toward the IVC results from muscular contraction around nonobstructed veins and one-way valves that close as blood passes them. These valves prevent abnormal backward blood flow toward the foot and ankle region.
The lower extremities have four types of veins. Superficial veins are located within the subcutaneous tissue between the dermis and muscular fascia. Examples are the greater and lesser (smaller) saphenous veins. Perforating veins connect the superficial veins to the deep veins of the leg. The deep veins are located below the muscular fascia. The communicating veins connect veins within the same system.
The greater saphenous vein is on the leg’s medial (inner) side. It originates from the dorsal veins on top of the foot and eventually drains into the common femoral vein in the groin region. By way of perforating veins, the greater saphenous vein drains into the deep venous system of both the calf and thigh.
The lesser saphenous vein is situated on the lateral (outer) side of the leg and originates from the lateral foot veins. As it ascends, it drains into the deep system at the popliteal vein behind the knee. Communicating veins connect the greater saphenous vein medially and the lesser saphenous vein laterally.
Intramuscular veins are the deep veins within the muscle itself, while the intermuscular veins are located between the muscle groups. The intermuscular veins are more important than other veins in development of chronic venous disease. Below the knee, the intermuscular veins are paired and take on the name of the artery they accompany—for example, paired anterior tibial, paired posterior tibial, and paired peroneal veins. Eventually, these veins form the popliteal vein behind the knee, which ultimately drains into the femoral vein of the groin.
As the common femoral vein travels below the inguinal ligament of the groin, it’s called the external iliac vein. Eventually, it becomes the common iliac vein, which drains directly into the IVC.
Pathophysiology
Abnormally elevated venous pressure stems from the leg’s inability to adequately drain blood from the leg toward the heart. Blood drainage from the leg requires the muscular pumping action of the leg onto the veins, which pump blood from the leg toward the heart as well as from the superficial veins toward the deep veins. Functioning one-way valves within the veins close when blood passes them, preventing blood from flowing backward toward the ankle. This process resembles what happens when you climb a ladder with intact rungs: As you step up from one rung to the next, you’re able to ascend.
CVI and the “broken rung” analogy
If the one-way valves are damaged or incompetent, the “broken rung” situation occurs. Think how hard it would be to climb a ladder with broken rungs: You might be able to ascend the ladder, but probably you would fall downward off the ladder due to the defective, broken rungs.
Normally, one-way valves ensure that blood flows from the lower leg toward the IVC and that the superficial venous system flows toward the deep venous system. The venous system must be patent (open) so blood flowing from the leg can flow upward toward the IVC. Blockage of a vein may result from an acute thrombosis (clot) in the superficial or deep systems. With time, blood may be rerouted around an obstructed vein. If the acute thrombosis involves one or more of the one-way valves, as the obstructing thrombosis opens up within the vein’s lumen, permanent valvular damage may occur, leading to post-thrombotic syndrome—a form of CVI.
CVI may result from an abnormality of any or all of the processes needed to drain blood from the leg—poor pumping action of the leg muscles, damage to the one-way valves, and blockage in the venous system. CVI commonly causes venous hypertension due to reversal of blood flow in the leg. Such abnormal flow may cause one or more of the following local effects:
leg swelling
tissue anoxia, inflammation, or necrosis
subcutaneous fibrosis
Compromised flow of venous blood or lymphatic fluid from the extremity.
“Water balloon” analogy
The effect of elevated venous pressure or hypertension is worst at the lowest gravitational point (around the ankle). Pooling of blood and intravascular fluid around the ankle causes a “water balloon” effect. A balloon inflated with water has a thin, easily traumatized wall. When it bursts, a large volume of fluid drains out. Due to its thicker wall, a collapsed balloon that contains less fluid is more difficult to break than one distended with water.
In a leg with CVI, subcutaneous fluid that builds up requires a weaker force to break the skin and ulcerate than does a nondistended leg with less fluid. This principle is the basis for compression therapy in treating and preventing CVI ulcers.
Effects of elevated venous pressure or hypertension
Increased pressure in the venous system causes:
abnormally high pressure in the superficial veins—60 to 90 mm Hg, compared to the normal pressure of 20 to 30 mm Hg
dilation and distortion of leg veins, because blood refluxes abnormally away from the heart and toward the lower leg and may move from the deep venous system into the superficial veins.
Abnormal vein swelling from elevated pressure in itself may impair an already abnormally functioning one-way valve. For instance, the valve may become more displaced due to the increase in intraluminal fluid, which may in turn worsen hypertension and cause an increase in leg swelling. Increased pressure from swollen veins also may dilate the capillary beds that drain into the veins; this may cause leakage of fluid and red blood cells from capillaries into the interstitial space, exacerbating leg swelling. Also, increased venous pressure may cause fibrinogen to leak from the intravascular plasma into the interstitial space. This leakage may create a fibrin cuff around the capillary bed, which may decrease the amount of oxygen entering the epidermis, increase tissue hypoxia, trigger leukocyte activation, increase capillary permeability, and cause local inflammation. These changes may lead to ulceration, lipodermatosclerosis, or both.
Visible changes may include dilated superficial veins, hemosiderin staining due to blood leakage from the venous tree, atrophie blanche, and lipodermatosclerosis. (See CVI glossary by clicking the PDF icon above.) Both atrophie blanche and lipodermatosclerosis result from local tissue scarring secondary to an inflammatory reaction of the leg distended with fluid.
Lipodermatosclerosis refers to scarring of subcutaneous tissue in severe venous insufficiency. Induration is associated with inflammation, which can cause the skin to bind to the subcutaneous tissue, causing narrowing of leg circumference. Lymphatic flow from the leg also may become compromised and inhibited in severe venous hypertension, causing additional leg swelling.
Patient history
In a patient with known or suspected CVI, a thorough history may lead to a working diagnosis. Be sure to ask the patient these questions:
Do you have pain?
Is your pain worse toward the end of the day?
Is the pain relieved with leg elevation at night?
Is it relieved with leg elevation during the day?
Do you have leg pain that awakens you at night?
How would you describe the pain?
Does the skin on your leg feel tight or irritated?
Have you noticed visible changes of your leg?
Do you have a leg ulcer?
Also determine if the patient has comorbidities that may exacerbate CVI, including PAD, renal failure, venous thrombosis, lymphedema, diabetes mellitus, heart failure, or malnutrition. (See CVI risk factors by clicking the PDF icon above .)
Common CVI symptoms
Approximately 20% of CVI patients have symptoms of the disease without physical findings. These symptoms may include:
tired, “heavy” legs that feel worse toward the end of the day
discomfort that worsens on standing
legs that feel best in the morning after sleeping or after the legs have been
elevated during the day.
Although patients may report leg discomfort, the history indicates that it doesn’t awaken them at night. Be aware that discomfort from CVI differs from that caused by PAD. With PAD, patients may report pain on exercise (claudication), pain with elevation (nocturnal pain), or constant pain (resting pain).
Signs of CVI (with or without ulcers) include:
leg swelling (seen in 25% to 75% of patients)
skin changes (such as hemosiderin staining or dermatitis)
telangiectasia, reticular veins, or both; while these are the most common signs, they represent an overall less severe finding
varicose veins with or without bleeding, occurring in one-third of patients with CVI.
Venous ulcers
Venous ulcers are the most common type of lower extremity ulcer. They’re commonly found on the medial aspect of the lower extremity, from the ankle to the more proximal calf area. Usually, they arise along the course of the greater saphenous vein, but also may be lateral and may occur at multiple locations. They aren’t found above the knee or on the forefoot. Venous ulcers are shallower than arterial ulcers and have considerable exudate consistent with drainage from a ruptured water balloon. They may extend completely around the leg.
CVI: From a heavy sensation to visible changes
In patients with CVI, blood flows within a lower extremity in an abnormal, reverse direction, causing build-up of blood and intravascular fluid around the ankle. Initially, this may cause only a sensation of heavy legs toward the end of the day, with no visible changes. Eventually, it may lead to venous ulcers or other visible changes. This abnormal blood flow results from dysfunction of the normal mechanisms that drain blood from the leg against gravity into the IVC.
Sardina D. Skin and Wound Management Course; Seminar Workbook. Wound Care Education Institute; 2011:92-112.
Donald A. Wollheim is a practicing wound care physician in southeastern Wisconsin. He also is an instructor for Wound Care Education Institute and Madison College. He serves on the Editorial Board for Wound Care Advisor.