Missed care, a relatively new concept in the medical community, refers to any part ofrequired patient care that is omitted of delayed. It’s not the same as a mistake or error, but like them, missed care can negatively affect patient outcomes.
I want to share the case of a patient admitted into home health care for wound care. The case includes several areas of missed care from many different different sources. (more…)
By Nancy Collins, PhD, RD, LD/N, FAPWCA, and Allison Schnitzer
Nutrition is a critical factor in the wound healing process, with adequate protein intake essential to the successful healing of a wound. Patients with both chronic and acute wounds, such as postsurgical wounds or pressure ulcers, require an increased amount of protein to ensure complete and timely healing of their wounds.
Elderly patients with wounds pose a special challenge because of their decreased lean body mass and the likelihood of chronic illnesses and insufficient dietary protein intake. To promote a full recovery, wound care clinicians must address the increased protein needs of wound patients, especially elderly patients. (more…)
Achieving excellent wound care outcomes can be challenging, given the growing number of high-risk patients admitted to healthcare facilities today. Many of these patients have comorbidities, such as obesity, diabetes, renal disease, smoking, chronic obstructive pulmonary disease, and poor nutritional status. These conditions reduce wound-healing ability. (more…)
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found that using hybrid 67Ga single-photon emission computed tomography and X-ray computed tomography (SPECT/CT) imaging combined with a bedside percutaneous bone puncture in patients with a positive scan is “accurate and safe” for diagnosing osteomyelitis in patients with diabetes who have a foot ulcer without signs of soft-tissue infection.
The new method, which avoids an invasive bone biopsy, has a sensitivity of 88% and a specificity of 93.6%. In the study of 55 patients, antibiotic treatment was avoided in 55% of suspected cases.
MRSA strains will likely continue to coexist in hospitals and communities
The strains of methicillin-resistant Staphylococcus aureus (MRSA) differ in the hospital and community settings, and both are likely to coexist in the future, according to a study in PLOS Pathogens.
C. difficile prevention actions fail to stop spread
Despite increasing activities to prevent the spread of Clostridium difficile, infection from C. difficile remains a problem in healthcare facilities, according to a survey of infection preventionists by the Association for Professionals in Infection Control and Epidemiology (APIC).
The survey found that 70% of preventionists have adopted additional interventions in their healthcare facilities since March 2010, but only 42% have seen a decline in C. difficile infection rates; 43% saw no decline.
A total of 1,087 APIC members completed the survey in January 2013. The survey also found that more than 92% of respondents have increased emphasis on environmental cleaning and equipment decontamination practices, but 64% said they rely on observation, rather than more accurate and reliable monitoring technologies, to assess cleaning effectiveness.
In addition, 60% of respondents have antimicrobial stewardship programs at their facilities, compared with 52% in 2010. Such programs promote the appropriate use of antibiotics, which can help reduce the risk of C. difficile infection.
Mast cells may not play significant role in wound healing
“Evidence that mast cells are not required for healing of splinted cutaneous excisional wounds in mice,” published in PLOS One, analyzed wound healing in three types of genetically mast-deficient mice and found they reepithelialized their wounds at rates similar to control mice. At the time of closure, the researchers found that scars in all the mice groups were similar in both “quality of collagen deposition and maturity of collagen fibers.” The findings fail to support the previously held belief that mast cells are important in wound healing.
Study identifies effective casting for diabetes-related plantar foot ulcers
Nonremovable casts that relieve pressure are more effective than removable casts or dressings alone for the treatment of plantar foot ulcers caused by diabetes, according to an analysis of clinical trials.
The authors of “Pressure-relieving interventions for treating diabetic foot ulcers,” published by The Cochrane Library, reviewed 14 randomized clinical trials that included 709 participants. Nonremovable pressure-relieving casts were compared to dressings alone, temporary therapeutic shoes, removable pressure-relieving devices, and surgical lengthening of the Achilles tendon.
The study also notes that when combined with Achilles tendon lengthening, nonremovable devices were more successful in one forefoot ulcer study than the use of a nonremovable cast alone.
Most studies were from the United States (five) and Italy (five), with Germany, the Netherlands, Australia, and India each contributing one study.
Prescriber preference drives use of antibiotics in long-term care
The study of 66,901 patients from 630 long-term care facilities found that 77.8%
received a course of antibiotics. The most common length (41%) was 7 days, but the length exceeded 7 days in 44.9% of patients. Patient characteristics were similar among short-, average-, and long-duration prescribers.
The study authors conclude: “Future trials should evaluate antibiotic stewardship interventions targeting prescriber preferences to systematically shorten average treatment durations to reduce the complications, costs, and resistance associated with antibiotic overuse.”
Electrophysical therapy may be helpful for diabetic foot ulcers
The authors of the study in International Wound Journal reviewed eight trials with a combined total of 325 patients. Five studies were on electrical stimulation, two on phototherapy, and one on ultrasound. Because of the small number of trials, the possibility of harmful effects can’t be ruled out, and the authors recommend “high-quality trials with larger sample sizes.”
Significant geographic variations in spending, mortality exist for diabetic patients with foot ulcers and amputations
The study in Journal of Diabetes and Its Complications found that higher spending wasn’t associated with a significant reduction in 1-year patient mortality. In addition, rates of hospital admission were associated with higher per capita spending and higher mortality rates for patients.
Home-based exercise program improves life for lymphedema patients
An individualized, home-based progressive resistance exercise program improves upper-limb volume and circumference and quality of life in postmastectomy patients with lymphedema, according to a study published in the Journal of Rehabilitation Research and Development.
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT
Every year, 1.9% of patients with diabetes develop foot ulcers. Of those, 15% to 20% undergo an amputation within 5 years of ulcer onset. During their lifetimes, an estimated 25% of diabetic patients develop a foot ulcer. This article discusses use of hyperbaric oxygen therapy (HBOT) in treating diabetic foot ulcers, presenting several case studies.
HBOT involves intermittent administration of 100% oxygen inhaled at a pressure greater than sea level. It may be given in a:
• multi-place chamber (used to treat multiple patients at the same time), compressed to depth by air as the patient breathes 100% oxygen through a face mask or hood (more…)
Necrotizing fasciitis (NF) results from an infection that attacks the fascia and subcutaneous tissues. The primary bacterial etiology is group A streptococcus, a facultative anaerobic bacterium. However, other bacteria may contribute. Sometimes called the “flesh-eating” disease because of the potentially devastating effect on the afflicted patient, NF can be monomicrobial or polymicrobial.
The four typical settings for NF are:
surgical bowel or abdominal trauma surgery
pressure ulcer and perianal abscess
injection sites (especially in drug users)
Bartholin abscess or minor vulvovaginal infection.
Because of the rapid course and ravaging nature of acute NF, clinicians must maintain a high index of suspicion if the patient has suggestive signs and symptoms. In 1990, puppeteer Jim Henson (best known for creating the Muppets) died from NF. At that time, little was known about the progression of group A streptococcal infection.
The disease can quickly cause death, so starting immediate treatment is even more crucial than confirming the diagnosis. Once the disease is suspected, antibiotics must be given immediately and the patient must be prepared for surgery at once. NF spreads rapidly, capable of progressing from a small lesion to death in days to weeks. Thus, delayed diagnosis increases the risk of death. Lack of knowledge about the disease and inability to recognize it promptly are the main reasons many victims die. This article can improve your knowledge base.
Overview
NF was discovered in 1871 by Joseph Jones, a Confederate Army surgeon. At that time, it was called hemolytic streptococcal gangrene, nonclostridial gas gangrene, nonclostridial crepitant cellulitis, necrotizing or gangrenous erysipelas, necrotizing cellulitis, bacterial synergistic gangrene, or synergistic necrotizing cellulitis.
NF involves the fascia, muscle compartments, or both. It can affect not only the muscle fascia but the superficial fascia. NF and cellulitis differ in the amount of tissue involved and extent of tissue involvement.
The most common areas of infection are the abdominal wall, perineum, and extremities. When NF affects the perineum and scrotum, it’s called Fournier gangrene, after the French dermatologist and virologist Alfred Jean Fournier.
The most common causes are trauma, surgery, and insect bites. The disease can affect persons of any age. Such comorbidities as diabetes, chronic renal failure, immunosuppressive therapy, hypertension, obesity, and malnutrition increase susceptibility.
Pathophysiology
NF falls into four classifications based on wound microbiology. Type 1, the most common, involves polymicrobial bacteria. Type 2 results from trauma and is associated with comorbidities. Type 3, rare in this country, stems from gram-negative marine bacteria. Type 4 is a fungal infection occurring mostly in immunocompromised persons. (See Comparing types of necrotizing fasciitis by clicking the PDF icon above.)
Disease progression
The four types of NF progress in a similar way. Bacteria secrete pyrogenic exotoxin A, which stimulates cytokines. These cytokines damage the endothelial lining; fluid then leaks into the extravascular space.
M proteins in streptococci and β-hemolytic streptococci exacerbate the immune reaction by inhibiting phagocytosis of polymorphonuclear leukocytes and normal neutrophil chemotaxis. As the immune reaction increases, blood vessels dilate, allowing toxins to leak through vessel walls, which in turn decreases blood flow. As the cascade continues, hypoxic conditions cause facultative aerobic organisms to grow and become anaerobic. These bacteria exacerbate destruction of surrounding cells and lead to release of carbon dioxide, water, hydrogen, nitrogen, hydrogen sulfide, and methane. As the infection continues to progress, toxins spread throughout the bloodstream and the patient becomes septic.
Assessment
Obtain the patient’s medical history and description of the wound. Determine when the changes first appeared and whether the affected area seemed to get worse recently.
In all NF types, patients commonly present with a small, painful area (possibly with entry marks) but no other signs or symptoms. The wound may appear as a bulla, cellulitis, or dermatitis, representing an infection developing in underlying tissues. The skin may have a wooden-hard feel as the infection progresses to the subcutaneous space and causes necrosis. The wound becomes discolored and necrotic; drainage is rare until surgical debridement begins. The patient quickly develops fever, chills, nausea, and vomiting. As NF progresses, bullae become dark purple with darkened edges; the patient grows disoriented and lethargic, and organ failure and respiratory failure
ensue. Without treatment, the patient dies.
Diagnosis
Diagnostic tests usually include magnetic resonance imaging, complete blood count with differential, comprehensive metabolic panel, and cultures. (See Diagnostic findings in necrotizing fasciitis by clicking the PDF icon above.)
Treatment
Immediate surgical debridement and broad-spectrum antibiotics are needed to stop the immune response to infection. Clindamycin, gentamicin, penicillin, or metronidazole may be given alone or in combination until culture results are available. Supportive care includes total parenteral nutrition for nutritional support, I.V. fluids, and oxygen. Limb amputation should be done only as a last resort.
Surgical debridement involves penetrating deep into the fascia and removing all necrotic tissue. After the first debridement, release of “dishwater fluid” may occur.
Administering hyperbaric oxygen therapy (HBOT) after the first debridement increases tissue oxygenation, thus reducing tissue destruction by anaerobic bacteria. During HBOT (usually given as a 90-minute treatment), the patient breathes 100% oxygen in an environment of increasing atmospheric pressure.
HBOT should be given in conjunction with surgical debridement (usually after each debridement) and should continue until necrotic tissue ceases and cell destruction stops. HBOT also promotes collagen synthesis and neoangiogenesis (new blood vessel growth), which boosts blood supply and oxygen to tissues.
Adverse effects of HBOT include ear pain, oxygen toxicity, and seizures. Ear pain can be minimized by swallowing or yawning. If the patient continues to have ear pain, ear tubes may be inserted by an otolaryngologist. During HBOT, air breaks (intervals of breathing room air) are important in controlling oxygen toxicity (the main cause of seizures).
Throughout the HBOT treatment period, wound dressings must be simple. Well-moistened gauze dressings and an abdominal pad provide good support. Once necrotic destruction occurs, dressings depend on wound size and the need to fill cavities. The patient may require a diverting colostomy, depending on wound
location and the amount of uncontrolled diarrhea. Blood glucose levels must be monitored before and after HBOT, as this treatment affects blood glucose.
Supportive care and follow-up treatment
During initial treatment, patients need supportive care and monitoring. Once they’re out of danger, begin teaching them how to prevent NF recurrences. Advise them to control blood glucose levels, keeping the glycated hemoglobin (HbA1c) level to 7% or less. Caution patients to keep needles capped until use and not to reuse needles. Instruct them to clean the skin thoroughly before blood glucose testing or insulin injection, and to use alcohol pads to clean the area afterward.
Before discharge, help arrange the patient’s aftercare, including home health care for wound management and teaching, social services to promote adjustment to lifestyle changes and financial concerns, and physical therapy to help rebuild strength and promote the return to optimal physical health. One helpful patient resource is the National Necrotizing Fasciitis Foundation. The Centers for Disease Control and Prevention section on necrotizing fasciitis includes “Common sense and great wound care are the best ways to prevent a bacterial skin infection.”
The life-threatening nature of NF, scarring caused by the disease, and in some cases the need for limb amputation can alter the patient’s attitude and viewpoint, so be sure to take a holistic approach when dealing with the patient and family. Today, NF has a much better survival rate than 2 decades ago when Jim Henson died. In my practice, I’ve seen four NF cases. Thanks to early identification, good wound care, and HBOT, these patients suffered only minimal damage.
Selected references
Boyer A, Vargas F, Coste F, et al. Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management. Intensive Care Med. 2009;35(5):847-853. doi:10.1007/s00134-008-1373-4.
Cain S. Necrotizing fasciitis: recognition and care. Practice Nurs. 2010;21(6):297-302.
Centers for Disease Control and Prevention. Notes from the field: fatal fungal soft-tissue infections after a tornado—Joplin, Missouri, 2011. MMWR. 2011;60(29):992.
Chamber AC, Leaper DJ. Role of oxygen in wound healing: a review of evidence. J Wound Care. 2011; 20(4):160-164.
Christophoros K, Achilleas K, Vasilia D, et al. Postraumatic zygomycotic necrotizing abdominal wall fasciitis with intraabdominal invasion in a non immunosuppressed patient. Internet J Surg. 2007;11(1). doi:10.5580/17a8.
Ecker K-W, Baars A, Topfer J, Frank J. Necrotizing fasciitis of the perineum and the abdominal wall-surgical approach. Europ J Trauma Emerg Surg. 2008;
34(3):219-228. doi:10.1007/s00068-008-8072-2.
Hunter J, Quarterman C, Waseem M, Wills A. Diagnosis and management of necrotizing fasciitis. Br J Hosp Med. 2011;72(7):391-395.
Magel DC. The nurse’s role in managing necrotizing fasciitis. AORN J. 2008;88(6):977-982.
Phanzu MD, Bafende AE, Imposo BB, Meyers WM, Portaels F. Under treated necrotizing fasciitis masquerading as ulcerated edematous Mycobacterium ulcerans infection (Buruli ulcer). Am J Trop Med Hyg. 2012;82(3):478-481.
Ruth-Sahd LA, Gonzales M. Multiple dimensions of caring for a patient with acute necrotizing fasciitis. Dimens Crit Care Nurs. 2006;25(1):15-21.
Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41(10):1373-1406.
Su YC, Chen HW, Hong YC, Chen CT, et al. Laboratory risk indicator for necrotizing fasciitis score and the outcomes. ANZ J Surg. 2008;78(11):968-972.
Taviloglu K, Yanar H. Necrotizing fasciitis: strategies for diagnosis and management. World J Emerg Surg. 2007;2:19.
Lydia Meyers is a medical reviewer for National Government Services in Castleton, Indiana, and a clinical liaison at CTI Nutrition in Indianapolis. She has 11 years of wound care experience in nursing homes, wound clinics, and home health.
Wound care has come a long way in just a few decades. With our expanded knowledge of wound healing and recent advances in treatment, we’re now able to assess wounds more accurately, recognize wound-related problems sooner, provide better interventions, and reduce morbidity.
To bring you up to date on current evidence-based wound management, this article focuses on assessing patients with chronic wounds, optimizing wound healing with effective wound-bed preparation, and selecting an appropriate dressing.
Wound chronicity and cause
Developing an appropriate plan of care hinges on conducting a thorough, accurate evaluation of both the patient and the wound. The first step is to determine whether the wound is acute or chronic.
• A chronic wound is one that fails to heal within a reasonable time—usually
3 months.
• An acute wound heals more quickly, causing minimal functional loss in the part of the body with the wound.
Identifying the cause of the wound also is essential. If the wound etiology is unknown, explore the patient’s medical history (including medication history) for clues to possible causes. Also review the patient’s history for conditions that could impede wound healing. (See What factors hamper healing? by clicking the PDF icon above)
Other important aspects of assessment include evaluating the patient’s nutritional status, quantifying the level of pain (if present), and gauging the patient’s self-care abilities.
General physical appearance
Conduct a general head-to-toe physical examination, focusing on the patient’s height, weight, and skin characteristics.
Height, weight, and weight trend
On admission, the patient’s height and weight should be measured to ensure appropriate nutritional and pharmacologic management. After a weight gain or loss, various factors may complicate wound healing. For instance, involuntary weight loss and protein-energy malnutrition may occur in both acute-care and long-term-care patients.
Especially note trends in your patient’s weight. For a long-term-care patient, a 5% weight loss over 30 days or a 10% loss over 180 days is considered involuntary. Arrange for a nutritional consult for any patient with an involuntary weight loss, as adequate nutrition is essential for general well-being and wound healing. (See A wound on the mend by clicking the PDF icon above.)
Skin color
Evaluate the patient’s skin color in light of ethnic background. If you note erythema—especially on a pressure point over a bony prominence—examine this area carefully for nonblanching erythema. Keep in mind that darkly pigmented skin doesn’t show such erythema and subsequent blanching, yet the patient may still be in jeopardy. So in dark-skinned patients, check for differences in skin color, temperature, or firmness compared to adjacent tissue; these differences may signify skin compromise.
Skin texture and turgor
Generally, healthy skin feels smooth and firm and has an even surface and good turgor (elasticity). To test turgor, gently grasp and pull up a fold of skin on a site such as the anterior chest below the clavicle. Does the skin return to place almost immediately after you release it, or does it stand up (“tent”)? Tenting indicates dehydration. But keep in mind that skin loses elasticity with age, so elderly patients normally have decreased turgor.
Skin temperature
With normal circulatory status, the skin is warm and its temperature is similar bilaterally. Areas of increased warmth or coolness suggest infection or compromised circulation. Be sure to check the temperature of skin surrounding the wound.
Wound assessment
Proper wound assessment can significantly influence patient outcome. Measure the wound carefully and document the condition of the wound bed. Remember that accurate descriptions are essential for guiding ongoing wound care. Repeat wound measurement and wound-bed assessment at least weekly, after the wound bed has been cleaned and debrided.
Keep in mind that assessing a chronic wound can be challenging. Wounds commonly have irregular shapes that can change quickly. Also, the multiple clinicians caring for the same patient may each describe the wound a bit differently.
Wound location
Note the precise anatomic location of the wound, as this can influence the wound care plan. A venous ulcer on the lower leg, for instance, requires different care than an arterial ulcer in the same site or a pressure ulcer on the ischium.
Circumference and depth
Use a paper or plastic measuring device to measure wound circumference and depth in centimeters (cm) or millimeters (mm). To promote accurate assessment of healing, be sure to use the same reference points each time you measure the wound.
You can use several methods to measure circumference. The most commonly used method of measurement is done in the head to toe direction. Measure the wound at its greatest length in that direction & measure the width at a 90 degree angle, at the widest point of the wound. Then multiply these two measurements (greatest length x greatest width) to obtain the total wound area. Although such linear measurements are imprecise, they yield gross information relative to wound healing when repeated over time.
Classify wound depth as partial thickness or full thickness.
• Partial-thickness wounds are limited to the skin layers and don’t penetrate the dermis. They usually heal by reepithelialization, in which epidermal cells regenerate and cover the wound. Abrasions, lacerations, and blisters are examples of partial-thickness wounds.
• Full-thickness wounds involve tissue loss below the dermis.
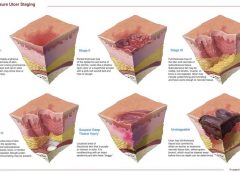
(Note: Pressure ulcers usually are classified by a four-stage system and diabetic foot ulcers by a grading system. Both systems are beyond this article’s scope.)
Measure and record wound depth based on the deepest area of tissue loss. To measure depth, gently place an appropriate device (such as a foam-tipped applicator) vertically in the deepest part of the wound, and mark the applicator at the patient’s skin level. Then measure from the end of the applicator to the mark to obtain depth.
Surrounding skin and tissue
Inspect for and document any erythema, edema, or ecchymosis within 4 cm of the wound edges, and reevaluate for these signs frequently. Because compromised skin near the wound is at risk for breakdown, preventive measures may be necessary.
Appearance of wound-bed tissue
Document viable tissue in the wound bed as granulation, epithelial, muscle, or subcutaneous tissue. Granulation tissue is connective tissue containing multiple small blood vessels, which aid rapid healing of the wound bed; appearing red or pink, it commonly looks shiny and granular. Epithelial tissue consists of regenerated epidermal cells across the wound bed; it may be shiny and silvery.
Check for nonviable tissue (also called necrotic, slough, or fibrin slough tissue), which may impede wound healing. It may vary in color from black or tan to yellow, and may adhere firmly or loosely to the wound bed. (See Picturing a necrotic wound by clicking the PDF icon above.)
Be sure to document the range of colors visible throughout the wound. Identify the color that covers the largest percentage of the wound bed. This color—and its significance—guide dressing selection.
Wound exudate
Document the amount, color, and odor of exudate (drainage) in the wound. Exudate with high protease levels and low growth factor levels may impede healing.
If the wound is covered by an occlusive dressing, assess exudate after the wound has been cleaned. Describe the amount of exudate as none, minimal, moderate, or heavy.
Describe exudate color as serous, serosanguineous, sanguineous, or purulent. Serous exudate is clear and watery, with no debris or blood present. Serosanguineous exudate is clear, watery, and tinged pink or pale red, denoting presence of blood. Sanguineous exudate is bloody, indicating active bleeding. Purulent exudate may range from yellow to green to brown or tan.
Describe wound odor as absent, faint, moderate, or strong. Note whether the odor is present only during dressing removal, if it disappears after the dressing is discarded, or if it permeates the room.
Wound edges
Wound edges indicate the epithelialization trend and suggest the possible cause and chronicity of the wound. The edges should attach to the wound bed. Edges that are rolled (a condition called epibole) indicate a chronic wound, in which epithelial cells are unable to adhere to a moist, healthy wound bed and can’t migrate across and resurface the wound.
Undermining and tracts
Gently probe around the wound edges and in the wound bed to check for undermining and tracts. Undermining, which may occur around the edges, presents as a space between the intact skin and wound bed (resembling a roof over part of the wound). It commonly results from shear forces in conjunction with sustained pressure. A tract, or tunnel, is a channel extending from one part of the wound through subcutaneous tissue or muscle to another part.
Measure the depth of a tract or undermining by inserting an appropriate device into the wound as far as it will go without forcing it. Then mark the skin on the outside where you can see or feel the applicator tip. Document your findings based on a clock face, with 12 o’clock representing the patient’s head and 6 o’clock denoting the feet. For instance, you might note “2.0-cm undermining from 7:00 to 9:00 position.”
Pain level
Ask the patient to quantify the level of pain caused by the wound, using the pain scale designated by your facility. Find out which pain-management techniques have relieved your patient’s pain in the past; as appropriate, incorporate these into a pain-management plan. Reevaluate the patient’s pain level regularly.
Wound-bed preparation
An evolving science, wound-bed preparation is crucial for minimizing or removing barriers to healing. The goal is to minimize factors that impair healing and maximize the effects of wound care. The key elements of wound-bed preparation are controlling bioburden and maintaining moisture balance. (For online resources on wound-bed preparation and other wound-care topics, see Where to get more information by clicking the PDF icon above.)
Controlling bioburden
Necrotic tissue and exudate harbor bacteria. A wound’s bioburden—the number of contaminating microbes—contributes to poor healing. All chronic wounds are considered contaminated or colonized, but not necessarily infected. In a colonized wound, healing is impeded as bacteria compete for nutrients; also, bacteria have harmful byproducts. To control bioburden, the wound must be cleaned and necrotic tissue must be debrided.
Cleaning the wound. Clean the wound before assessing it and applying a dressing. Use a noncytotoxic agent (typically, potable water, normal saline irrigating solution, or an appropriate wound-cleaning agent). Antiseptic solutions generally aren’t recommended for wound irrigation or dressings because they’re toxic to fibroblasts and other wound-repairing cells. If you must use such a solution, make sure it’s well diluted.
To ensure gentle cleaning or irrigation, pour solution over the wound bed or gently flush the wound with solution (using a 60-mL catheter-tip syringe) until the drainage clears. Know that pressurized irrigation techniques and whirlpool therapy aren’t recommended for wound cleaning because they disturb cell proliferation in the wound bed.
Debriding the wound. Debridement removes slough and necrotic tissue. Nonselective debridement techniques remove any type of tissue within the wound bed, whereas selective methods remove only necrotic tissue. (See Wound debridement techniques by clicking the PDF icon below.)
Maintaining moisture balance
To maintain moisture balance in the wound bed, you must manage exudate and keep the wound bed moist. The proper dressing (which may stay in place for days or longer) supports moist wound healing and exudate management. To minimize fluid pooling, a drain may be inserted into the wound. Negative-pressure wound therapy also may aid removal of excess exudate.
Choosing an appropriate dressing
The wound dressing plays a major role in maintaining moisture balance. Dressing selection is challenging because of the large number and variety of dressings available. Each product has specific actions, benefits, and drawbacks, so determining which dressing best suits the patient’s needs is a multifaceted process.
Dressing choice depends on such factors as wound type and appearance, exudate, presence or absence of pain, and required dressing change frequency. (See Dressings Options by clicking the PDF icon above.)
In a traditional dressing, gauze is applied in layers. The initial (contact) layer in the wound bed absorbs drainage and wicks it to the next layer; most often, this layer consists of woven cotton gauze or synthetic gauze. Remove the gauze gently, because it may be stuck to the wound or incision (especially if the gauze is cotton). For easier removal, moisten the dressing with normal saline solution to loosen it.
With a traditional dressing, the cover layer or secondary dressing is an abdominal pad with a “no-strike-through” layer next to the outside of the dressing. Be aware that wet-to-dry dressings are highly discouraged for their nonselective debriding effect and inability to provide a moist wound bed.
Reassess the patient’s wound at least weekly (after preparing the wound bed and dressing the wound) to determine healing progress. Keep in mind that wound-care management is a collaborative effort. Once you’ve assessed the patient, discuss your findings and subsequent wound management with other members of the team.
Wound care wisdom
Getting wiser about wound care will help your patients achieve good outcomes. Poor wound healing can be frustrating to patients, family members, and healthcare providers alike. Chronic wounds may necessitate lifestyle changes and lead to severe physical consequences ranging from infection to loss of function and even death. By performing careful assessment, tailoring patients’ wound care to wound etiology, and using evidence-based protocols to manage wounds, you can promote speedier wound healing, help lower morbidity, and improve quality of life.
Selected references
Bryant RA, Nix DP. Acute and Chronic Wounds: Current Management Concepts. 4th ed. St. Louis, MO: Mosby; 2011.
Gardener SE, Frantz R, Hillis SL, Park H, Scherubel M. Diagnostic validity of semiquantitative swab cultures. Wounds. 2007;(19)2:31-38.
Krasner DL, Rodeheaver GT, Sibbald RG. Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. 4th ed. Wayne, PA: HMP Communications; 2007.
Langemo DK, Brown G. Skin fails too: acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19(4):206-211.
Langemo DK, Anderson J, Hanson D, Hunter S, Thompson P. Measuring wound length, width, and area: which technique? Adv Skin Wound Care. 2008;21:42-45.
Milne C, Armand OC, Lassie M. A comparison of collagenase to hydrogel dressings in wound debridement. Wounds. 2010:22(11):270-274.
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Washington, DC: National Pressure Ulcer Advisory Panel; 2009.
Ovington LG. Hanging wet-to-dry dressings out to dry. Adv Skin Wound Care. 2002;15(2):79-86.
Sibbald RG, Coutts P, Woo KY. Reduction of bacterial burden and pain in chronic wounds using a new polyhexamethylene biguanide antimicrobial foam dressing—clinical trial results. Adv Skin Wound Care. 2011;24(2):78-84.
Solway DR, Consalter M, Levinson DJ. Microbial cellulose wound dressing in the treatment of skin tears in the frail elderly. Wounds. 2010:22(1):17-19.
Wound Ostomy and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers. Mt. Laurel, NJ: Author; 2010
Patricia A. Slachta is a Clinical Nurse Specialist at The Queens Medical Center in Honolulu, Hawaii and an adjunct nursing instructor at the Technical College of the Lowcountry in Beaufort, South Carolina.
By combining bioactive peptides, researchers have successfully stimulated wound healing in an in vitro and in vivo study. The studies, published in PLoS ONE, show that the combination of two peptides stimulates growth of blood vessels and promotes tissue re-growth of tissue. Further research into these peptides could potentially lead to new therapies for chronic and acute wounds.
The researchers evaluated a newly-created peptide, UN3, in pre-clinical models with the goal of simulating impaired wound healing as in patients suffering from peripheral vascular diseases or uncontrolled diabetes. They discovered that the peptide increased the development of blood vessel walls by 50%, with an 250% increase in blood vessel growth, and a 300% increase in cell migration in response to the injury. (more…)