This issue’s resources include patient tools and new guidelines.
Improving patient safety
Research suggests that adverse events affect patients with limited English proficiency (LEP) more frequently, are commonly caused by communication problems, and are more likely to result in serious harm compared to adverse events affecting English-speaking patients. Your hospital can take steps to reduce risks of adverse events for patients with LEP with “Improving patient safety systems for patients with limited english proficiency: a guide for hospitals,” from The Disparities Solutions Center, Mongan Institute for Health Policy at Massachusetts General Hospital, Boston, and Abt Associates, Cambridge, Massachusetts. (more…)
The Rolling Stones may have said it best when they sang, “You can’t always get what you want,” a sentiment that also applies to wound care. A common frustration among certified wound care clinicians is working with other clinicians who have limited current wound care education and knowledge. This situation worsens when these clinicians are making treatment recommendations or writing treatment orders not based on current wound-healing principles or standards of care.
Frequently, these same clinicians seem uninterested in listening to what you say and aren’t receptive to treatment suggestions. This is where your skills of diplomacy will make all the difference. Rarely is it a simple matter of sharing your expertise to change a person’s mind. Lack of training and knowledge of current best practices may be part of the reason for resistance. “We’ve always done it that way” or “The rep told me” are common statements you might hear.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Have you ever faced responsibility for a patient-care situation you learned about in school but had yet to encounter in the real world? With so many different health conditions and constant advancements in medical care, it’s not surprising that this happens frequently to many clinicians. The first and easiest way for most…
By Joanne Aspiras Jovero, BSEd, BSN, RN; Hussam Al-Nusair, MSc Critical Care, ANP, RN; and Marilou Manarang, BSN, RN A common problem in long-term care facilities, pressure ulcers are linked to prolonged hospitalization, pain, social isolation, sepsis, and death. This article explains how a Middle East rehabilitation facility battles pressure ulcers with the latest evidence-based practices, continual staff education, and…
By Julie Boertje, MS, RN, LMFT, QMRP, and Liz Ferron, MSW, LICSW Almost everyone agrees that achieving a work-life balance is a good thing. Without it, we risk long-term negative effects on our physical and mental health, our relationships, and our work performance. But many clinicians have a hard time achieving this balance due to job demands, erratic work schedules,…
By Bill Richlen, PT, WCC, CWS, DWC, and Denise Stetter, PT, WCC, DCCT The Rolling Stones may have said it best when they sang, “You can’t always get what you want,” a sentiment that also applies to wound care. A common frustration among certified wound care clinicians is working with other clinicians who have limited current wound care education and…
Low BMD common after ostomy Low bone mineral density (BMD) is common in patients with inflammatory bowel disease who have a stoma placed, according to “Frequency, risk factors, and adverse sequelae of bone loss in patients with ostomy for inflammatory bowel diseases,” published in Inflammatory Bowel Diseases.
Take a few minutes to check out this potpourri of resources. International Ostomy Association The International Ostomy Association is an association of regional ostomy associations that is committed to improving the lives of ostomates. Resources on the association’s website include: a variety of discussion groups information for patients list of helpful links. The site also provides contact information for the…
By Ron Rock MSN, RN, ACNS-BC Since its introduction almost 20 years ago, negative-pressure wound therapy (NPWT) has become a leading technology in the care and management of acute, chronic, dehisced, traumatic wounds; pressure ulcers; diabetic ulcers; orthopedic trauma; skin flaps; and grafts. NPWT applies controlled suction to a wound using a suction pump that delivers intermittent, continuous, or variable…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Exudate (drainage), a liquid produced by the body in response to tissue damage, is present in wounds as they heal. It consists of fluid that has leaked out of blood vessels and closely resembles blood…
By Jennifer Oakley, BS, RN, WCC, DWC, OMS I used to think I could do it alone. I took the wound care certification course, passed the certification exam, and took all of my new knowledge—and my new WCC credential—back to the long-term care facility where I worked. I was ready to change the world. It didn’t take me long to…
By Carrie Carls, BSN, RN, CWOCN, CHRN, and Sherry Clayton, RHIA In an atmosphere of changing reimbursement, it’s important to understand indications and utilization guidelines for healthcare services. Otherwise, facilities won’t receive appropriate reimbursement for provided services. This article focuses on Medicare reimbursement for hyperbaric oxygen therapy (HBOT). (See What is hyperbaric oxygen therapy?) Indications and documentation requirements
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN We’ve all experienced how a bad night’s sleep can affect our mood and ability to function the next day. Now imagine you’re a patient who has a pressure ulcer, most likely secondary to a declining disease state, and you’re being awakened and manipulated every 2 hours or in some cases hourly. How…
Since its introduction almost 20 years ago, negative-pressure wound therapy (NPWT) has become a leading technology in the care and management of acute, chronic, dehisced, traumatic wounds; pressure ulcers; diabetic ulcers; orthopedic trauma; skin flaps; and grafts. NPWT applies controlled suction to a wound using a suction pump that delivers intermittent, continuous, or variable negative pressure evenly through a wound filler (foam or gauze). Drainage tubing adheres to an occlusive transparent dressing; drainage is removed through the tubing into a collection canister. NWPT increases local vascularity and oxygenation of the wound bed and reduces edema by removing wound fluid, exudate, and bacteria. (more…)
By Carrie Carls, BSN, RN, CWOCN, CHRN, and Sherry Clayton, RHIA
In an atmosphere of changing reimbursement, it’s important to understand indications and utilization guidelines for healthcare services. Otherwise, facilities won’t receive appropriate reimbursement for provided services. This article focuses on Medicare reimbursement for hyperbaric oxygen therapy (HBOT). (See What is hyperbaric oxygen therapy?)
By Jennifer Zinn, MSN, RN, CNS-BC, CNOR, and Vangela Swofford, BSN, RN, ASQ-CSSBB
For surgical patients, operative wound classification is crucial in predicting postoperative surgical site infections (SSIs) and associated risks. Information about a patient’s wound typically is collected by circulating registered nurses (RNs) and documented at the end of every surgical procedure. (more…)
Aresolution is a serious decision or determination to do, or not to do, something. Traditionally, most New Year’s resolutions focus on self-improvement: losing weight, giving up a bad habit, exercising more, being a better person. Because most of us spend about half of our waking lives at work, perhaps our work lives should be the subject
of some of our resolutions. Here are a few work-related resolutions I’ve come up with: (more…)
No matter where you work or who your distributors are, ensuring the patient has sufficient ostomy supplies can be a challenge. Whether you’re the nurse, the physician, the patient, or the family, not having supplies for treatments can heighten frustration with an already challenging situation, such as a new ostomy. Here’s how to reduce the chance of experiencing frustrations related to ostomy supplies. (more…)
By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS
Imagine your physician has just told you that your rectal pain and bleeding are caused by invasive colon cancer and you need prompt surgery. She then informs you that surgery will reroute your feces to an opening on your abdominal wall. You will be taught how to manage your new stoma by using specially made ostomy pouches, but will be able to lead a normal life.
Like most people, you’d probably be in shock after hearing this. More than 700,000 people in the United States are living with ostomies. Every year, at least 100,000 ostomy surgeries are done, preceded by a conversation much like the one above. So how do patients recover from the shock of learning about their pending surgery—and then return to a full life? (more…)
Knowledge is exploding online, making it essential that you’re comfortable using the Internet. You can also go online to save time and find a job, among other tasks. (See Online value.)
However, you also need to keep in mind that anyone can put information on the Internet. As the caption of a cartoon by Peter Steiner, published in The New Yorker says, “On the Internet, nobody knows you’re a dog.” (more…)
The guidelines include recommendations for practice, education, policy, and future resource. Strategies for implementation are given, as well as several useful appendices, such as:
• Debridement Decision-Making Algorithm
• A Guide to Dressing Foot Wounds
• PEDIS: Diabetes Foot Ulcer Classification System
• Offloading Devices
• Optimal Treatment Modalities.
PREPARE is a useful and patient-friendly website designed to help prepare people to make complex medical decisions. The website was developed by clinical researchers from the San Francisco VA Medical Center; the University of California, San Francisco; and NCIRE—The Veterans Health Research Institute.
PREPARE uses videos to provide concrete examples of how to identify what is most important in life; how to communicate that with family, friends, and doctors; and how to make informed medical decisions when the time comes. Users can also download a PDF of a PREPARE pamphlet.
Free guides for infection prevention from APIC
Download two free implementation guides for infection prevention from the Association for Professionals in Infection Control and Epidemiology (APIC):
This revised guide contains strategies for prevention, considerations for specific patient populations, evolving practices, and how to incorporate current regulations.
Topics include:
• C. difficile in pediatrics and skilled nursing facilities
• pathogenesis and changing epidemiology of C. difficile infection diagnosis
• environmental control
• new and emerging technologies
• tools and examples to help apply preventative measures, such as hand hygiene monitoring, environmental cleaning, and isolation compliance.
This guide includes infection-prevention standards, regulations, and best practices, as well as instructions, examples, and tools to conduct surveillance and risk assessments.
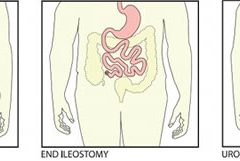
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
If you’re keeping up on wound care, you know a lot of new things are coming to market with enough decent science behind them to make them reasonable options to consider in your practice. And as true-blooded Americans and citizens of the post-industrialized world, we want what’s newest, fastest, and best in class in everything. It’s just our nature.
But does it truly serve us to be eager to try new therapies even when the current treatment plan is successful? Perhaps. We know we must never close our eyes to new developments in our field that can lead to better outcomes. Knowing when and what to change can lead to better outcomes for the patient, the wound, and our collective pocketbook.
I’ve long maintained we can achieve excellent-quality wound care if we just stick to the basics the vast majority of the time. Why? Systemic, psychosocial, and local factors all affect wound healing—not just the dressing or cream. Our job is to provide the optimum environment possible for wound healing. That requires us to look at and support the whole body toward optimum health, not solely the wound.
The basics begin with identifying the cause of the wound and implementing interventions to reduce, control, or eliminate the cause. Next, we strive to manage local and psychosocial factors by choosing topical products that will maintain moisture balance, keep the wound warm, and protect it. If the wound doesn’t show progress toward healing within 2 weeks (or as expected, given the patient’s overall condition and ability to heal), we need to reevaluate the plan and begin making changes.
The best rule is to make one change at a time. That makes it much easier to determine what’s working and what isn’t. Once all the basics are in place and required changes have been made, if healing is still stalled or nonexistent, consider trying the available new products and specialty products.
Never close your clinical mind to advances in the field. To do that would be a disservice to your patients. But you should change the treatment plan only when a change is needed—not just for the sake of changing it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois