General characteristics
Document if the diversion is an intestinal or urinary ostomy, whether it’s temporary or permanent, and the location— abdominal quadrant, skin fold, umbilicus. (See Descriptor reference.) (more…)
Read MoreMore results...
Practical Issues in Wound, Skin and Ostomy Management

Document if the diversion is an intestinal or urinary ostomy, whether it’s temporary or permanent, and the location— abdominal quadrant, skin fold, umbilicus. (See Descriptor reference.) (more…)
Read More

As a wound care specialist, you have learned about many skin conditions, some so unusual and rare that you probably thought you would never observe them. I’ve been a nurse for 38 years, with the last 10 years in wound care, and that’s certainly what I thought. But I was wrong. Let me tell you about my challenging patient with…

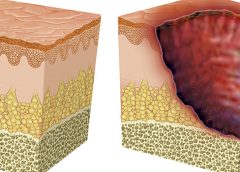
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when…
Electrical stimulation and pressure ulcer healing in SCI patients A systematic review of eight clinical trials of 517 patients with spinal cord injury (SCI) and at least one pressure ulcer indicates that electrical stimulation increases the healing rate of pressure ulcers. Wounds with electrodes overlaying the wound bed seem to have faster pressureulcer healing than wounds with electrodes placed on intact skin around the ulcer.

Here is a round-up of resources that you may find helpful in your practice. New illustrations for pressure-injury staging The National Pressure Ulcer Advisory Panel (NPUAP) has released new illustrations of pressure injury stages. You can download the illustrations, which include normal Caucasian and non-Caucasian skin illustrations for reference. There is no charge for the illustrations as long as they are being used for educational purposes, but donations to…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of cutaneous candidiasis. Cutaneous candidiasis is an infection of the skin caused by the yeast Candida albicans or other Candida species. Here’s a snapshot of this condition.

Topical application of silver nitrate is often used in wound care to help remove and debride hypergranulation tissue or calloused rolled edges in wounds or ulcerations. It’s also an effective agent to cauterize bleeding in wounds. Silver nitrate is a highly caustic material, so it must be used with caution to prevent damage to healthy tissues.

For an ostomy pouching system to adhere properly, the skin around the stoma must be dry and intact. Otherwise, peristomal skin problems and skin breakdown around the stoma may occur. In fact, these problems are the most common complications of surgical stomas. They can worsen the patient’s pain and discomfort, diminish quality of life, delay rehabilitation, increase use of ostomy supplies, and raise healthcare costs. Peristomal skin problems also perpetuate a…
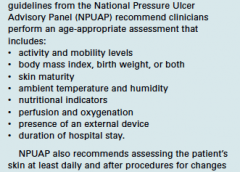
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular…

Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement you’d feel. What if you had to live through this experience repeatedly? That’s what many elderly people go through, suffering with skin tears through no fault of their own. Some go on to develop complications. A skin tear is a traumatic wound caused by shear, friction, or blunt-force trauma that results in a partial-…

This issue marks the fourth anniversary of the “Best of the Best” issue of Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy. Fittingly, it comes during an Olympics year. Since 1904, the Olympics have awarded gold medals to athletes whose performance makes them the “best of the best.” This year, we’re proud to present our own “Best…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to…

Diabetic foot ulcers stem from multiple factors, including peripheral neuropathy, high plantar pressures, decreased vascularity, and impaired wound healing. Contributing significantly to morbidity, they may cause limb loss and death. (See Foot ulcers and diabetes.) Initially, hydrocolloid dressings were developed to function as part of the stomal flange. Based on their success in protecting peristomal skin, they were introduced gradually…

Imagine you have a health condition that affects your life every day. Then imagine being told nothing can be done about it; you’ll just have to live with it. Or worse yet, your physician tells you the problem is “you’re just fat.”
Many people with lymphedema or lipedema have no idea their condition has a name or that many other people suffer from the same thing. Although lymphedema and lipedema can’t be cured, proper management and resources can help patients cope. This article improves your grasp of these conditions, describes how to recognize and manage them, and explains how to support your patients.
To understand lymphedema and lipedema, first you need to understand how the lymphatic system functions. It makes lymph, then moves it from tissues to the bloodstream. It also plays a major role in the immune system, aiding immune defense. In addition, it helps maintain normal fluid balance by promoting fluid movement from the interstitial tissues back to the venous circulation. (See Lymphatic system: Four major functions.)
If the lymphatic system is impaired from a primary (hereditary or congenital) condition or a secondary problem, lymphedema can result. In this chronic, potentially progressive, and incurable condition, protein-rich fluid accumulates in the interstitial tissues.
Lymphedema occurs in four stages.
Stage 0. During this stage (also called the subclinical or latency stage), transport capacity of the lymphatic system decreases but remains sufficient to manage normal lymphatic loads. Signs and symptomsaren’t evident and can be measured only by sensitive instruments, such as bioimpedance spectroscopy and optoelectronic volumetry. Without such instruments to quantify volume changes, diagnosis may rest on subjective complaints.
In this stage, limited functional reserve of the lymphatic system leads to a fragile balance between subnormal transport capacity and lymphatic loads. Added stress on the lymphatic system (as from extended heat or cold exposure, injury, or infection) may cause progression to stage 1.
Providing appropriate patient information and education, especially after surgery, can dramatically reduce the risk that lymphedema will progress to a more serious stage.
Stage 1. Considered the spontaneously reversible stage, stage 1 is marked by softtissue pliability without fibrotic changes. Pitting can be induced easily. In early stage 1, limb swelling may recede over – night. With proper management, the patient can expect the extremity to decrease to a normal size compared to that of the uninvolved limb. Otherwise, lymphedema is likely to progress to stage 2.
Stage 1 lymphedema may be hard to distinguish from edemas from other causes. Clinicians must rely on the patient history and monitor for swelling resolution with conventional management, such as compression and elevation, or note if swelling persists despite these standard interventions.
Stage 2. Sometimes called the spontaneously irreversible stage, stage 2 is identified mainly from tissue proliferation and subsequent fibrosis (called lymphostatic fibrosis). The fluid component can be removed spontaneously, but removal of the increased tissue proliferation (initially irreversible) takes more time. Tissue proliferation stems from long-standing accumulation of protein-rich fluid; over time, the tissue hardens and pitting is hard to induce. In many cases, swelling volume increases, exacerbating the already compromised local immune defense.
Consequently, infections (particularly cellulitis) are common; these, in turn, increase the volume of the affected area. Proper treatment can reduce volume.
With proper care (complete decongestive therapy [CDT]), lymphedema can stabilize during stage 2. But patients with chronic or recurrent infections are likely to progress to stage 3.
Stage 3. Also called lymphostatic elephantiasis, this stage is marked by further fluid volume increases and progression of tissue changes. Lymphostatic fibrosis becomes firmer and other skin alterations may occur, including papillomas, cysts, fistulas, hyperkeratosis, fungal infections, and ulcers. Pitting may be present. Natural skinfolds deepen (especially those of the dorsum of the wrist or ankle) and, in many cases, cellulitis recurs.
If lymphedema management starts during this stage, reduction can still occur. Even in extreme cases, with proper care and patient adherence to treatment, lymphostatic elephantiasis can be reduced so the leg is a normal or near-normal size.
A thorough physical examination is the gold standard for diagnosing lymphedema. A complete patient history, body-systems review, inspection, and palpation can help determine if edema is lymphedema.
Clinically, the only test with proven reliability and validity in diagnosing lymphedema is the Stemmer sign. Fibrotic changes associated with lymphedema can lead to thickened skin over the proximal phalanges of the toes or fingers. If you can’t tent or pinch the skin on the involved extremity, lymphedema is present (a positive Stemmer sign). However, a negative finding (soft, pliable tissue) doesn’t rule out lymphedema because the condition may be in an early stage, before tissue proliferation and fibrosis have set in.
Although incurable, lymphedema can be managed successfully through CDT. This approach involves proper identification of lymphedema, manual lymph drainage, skin and nail care, patient education, compression, and exercise.
CDT has two phases:
• Phase I, the intensive phase, continues until the extremity has decongested or reached a plateau. The clinician provides treatments and educates the patient about all aspects of CDT to prepare him or her for phase II. Phase I can last several weeks to several months depending on lymphedema severity.
• Phase II, the maintenance phase, begins once the extremity has decongested or plateaued. This phase still focuses on CDT, but now the patient, not the clinician, is responsible for all care. The goal is to reduce limb size while enabling the patient to become self-sufficient in managing lymphedema. Although CDT can bring significant improvements in limb size, skin quality, and function, patients must remember that phase II continues lifelong. Be sure to provide education about ongoing self-management strategies.
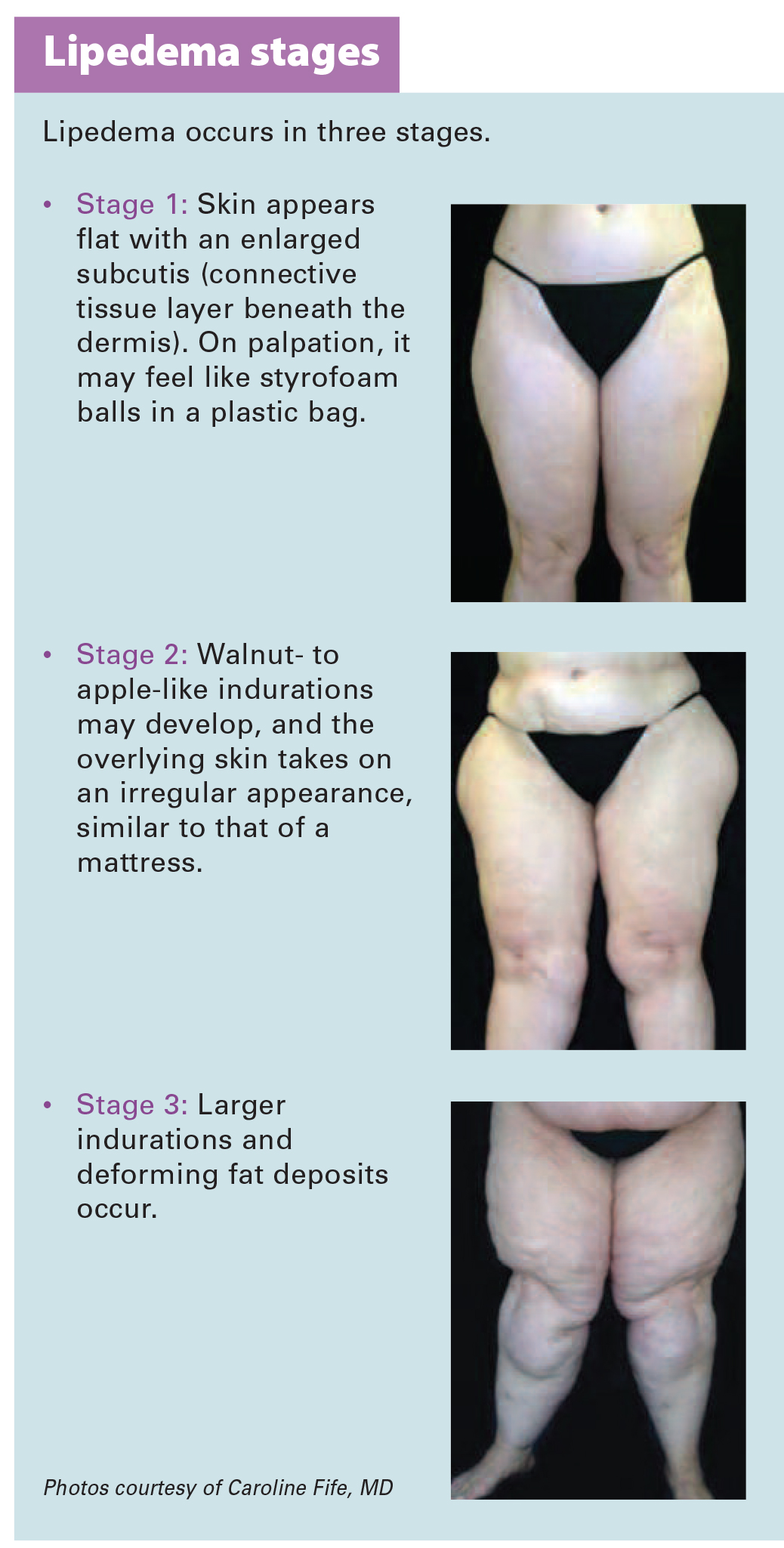
Lipedema is a painful disorder of fat deposition. Pathologic deposition of fatty tissue (usually below the waist) leads to progressive leg enlargement. Like lymphedema, lipedema is incurable but manageable. Unless managed properly, lipedema can reduce mobility, interfere with activities of daily living, and lead to secondary lymphedema. (See Lipedema stages.)
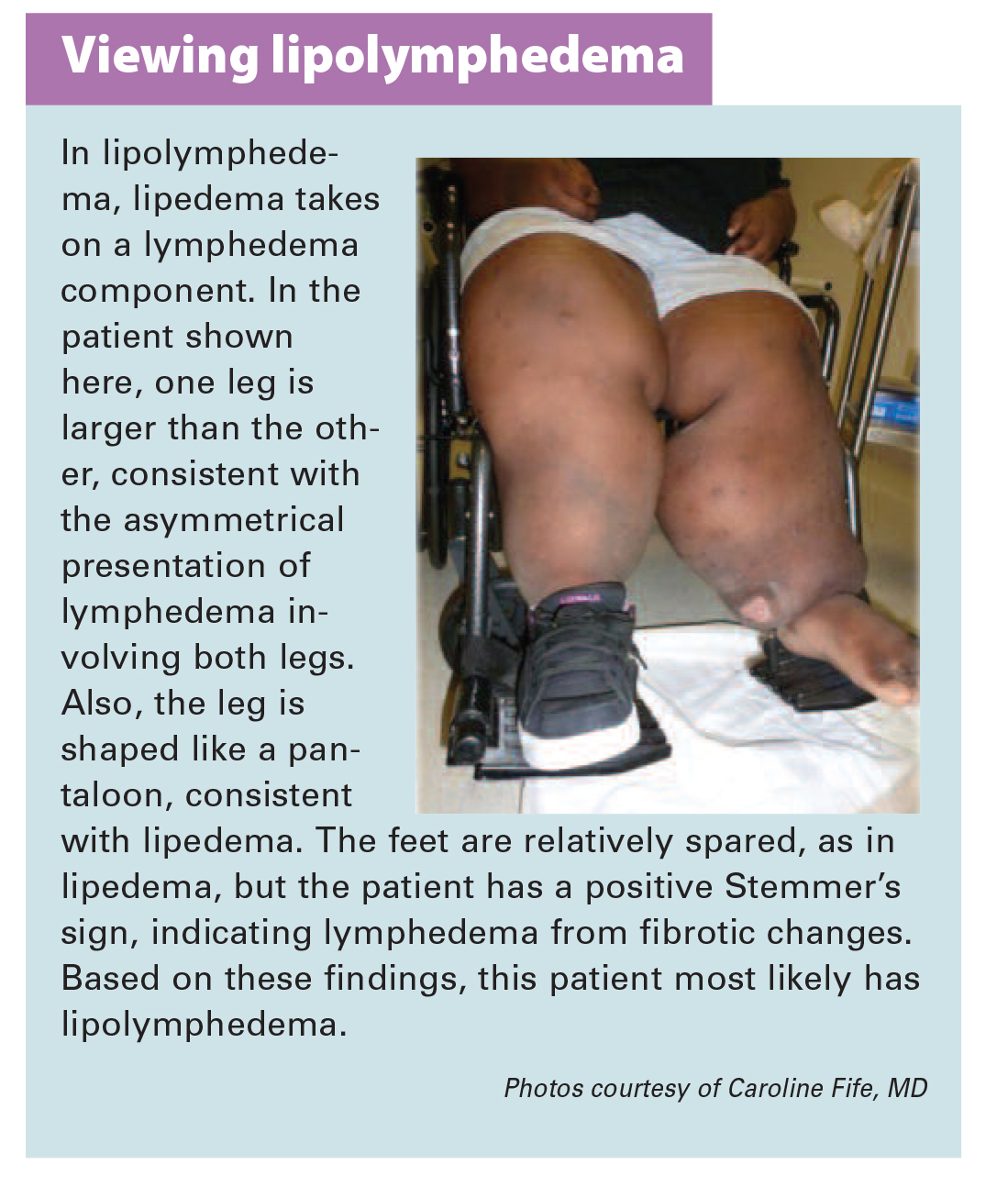
Lipedema commonly is misdiagnosed as lymphedema. However, lymphedema involves protein-rich fluid, whereas lip edema is a genetically mediated fat disorder. Because lipedema resists diet and exercise, it can lead to psychosocial complications. Lipedema occurs almost exclusively in women; typically, onset occurs between puberty and age 30. One unpublished epidemiologic study puts lip edema incidence in females at 11%. Some patients have a combination of lipedema and lymphedema. (See Viewing lipolymphedema.)
As with lymphedema, lipedema diagnosis rests on clinical presentation. Lipedema characteristics include bilateral and symmetrical involvement, absence of pitting (because lipedema isn’t a fluid disorder), soft and pliable skin, and filling of the retromalleolar sulcus (called the fat pad sign.)
Key signs and symptoms include:
• feeling of heaviness in the legs (aching dysesthesia)
• easy bruising
• sensitivity to touch (called “painful fat syndrome”)
• orthostatic edema
• oatmeal-like changes to skin texture.
Nearly half of lipedema patients are overweight or obese, but many appear of normal weight from the waist up. Essentially, the upper and lower extremities don’t match. The lower extremities typically show fatty deposits extending from the iliac crest to the ankles, sparing the feet. (See Lipedema patterns.)
Lipedema is best managed through weight control, as additional weight gain through adipose tissue tends to deposit in the legs. For patients with concomitant lymphedema (lipolymphedema), modified CDT helps reduce and manage lymphatic compromise. To address excess fat deposition, newer “wet” liposuction techniques have proven beneficial. These techniques gently detach adipose cells from the tissue, helping to preserve connective tissue and lymphatic vessels.
In both lymphedema and lipedema, early identification and proper diagnosis are key. (See Differentiating lymphedema and lipedema.) A thorough history and physical exam will likely lead to an accurate diagnosis, if clinicians know what to look for. Proper diagnosis and treatment can prevent expensive and ineffective interventions, which can negatively affect both the patient’s condition and psychological well being.
Heather Hettrick is an associate professor at Nova Southeastern University, Department of Physical Therapy in Fort Lauderdale, Florida.
Fat Disorders Research Society. Lipedema description.
Fife CE, Maus EA, Carter MJ. Lipedema: a frequently misdiagnosed and misunderstood fatty deposition syndrome. Adv Skin Wound Care. 2010;23(2):81-92
Herbst KL. Rare adipose disorders (RADS) masquerading as obesity. Acta Pharmacol Sin. 2012;33(2):155-72.
National Lymphedema Network. Position papers.
Schmeller W, Hueppe M, Meier-Vollrath I. Tumescent liposuction in lipoedema yields good long-term results. Br J Dermatol. 2012;166(1):161-8.
Zuther J. A closer look at lipedema and the effects on the lymphatic system. December 13, 2012. lymphedemablog.com/2012/12/13/a-closer-look-at-lipedema-and-the-effects-on-the-lymphatic-system/
Zuther J. Stages of lymphedema. October 3, 2012.
Read More
The goal of wound-bed preparation is to create a stable, well-vascularized environment that aids healing of chronic wounds. Without proper preparation, even the most expensive wound-care products and devices are unlikely to produce positive outcomes.
To best prepare the wound bed, you need to understand wound healing physiology and wound care basics, as well as how to evaluate the patient’s overall health and manage wounds that don’t respond to treatment. (See Normal wound healing.) (more…)
Read More

Keeping clinicians up-to-date on clinical knowledge is one of the main goals of the Wild on Wounds (WOW) conference held each September in Las Vegas. Every year, I present the opening session, called “The Buzz Report,” which focuses on the latest-breaking wound care news—what’s new, what’s now, and what’s coming up. I discuss new products, practice guidelines, resources, and tools from the last 12 months in skin, wound, and ostomy management. In…

Using a checklist form to document wound care can make the task easier and faster—and help ensure that you’ve captured all pertinent data needed for assessment, reimbursement, and legal support. But the form itself may not be comprehensive; some important fields may be missing. Recently, we at Wound Care Advisor received a question from a clinician who was having trouble deciding how to code a patient’s wound in her hospital’s…

Self-management ostomy program improves HRQOL A five-session ostomy self-care program with a curriculum based on the Chronic Care Model can improve health-related quality of life (HRQOL), according to a study in Psycho-Oncology. “A chronic care ostomy self-management program for cancer survivors” describes results from a longitudinal pilot study of 38 people. Participants reported sustained improvements in patient activation, self-efficacy, total HRQOL, and physical and social well-being. Most patients had a history of…

Check out the following resources, all designed to help you in your clinical practice. Human trafficking resources Victims of human trafficking often suffer tremendous physical and psychological damage. Clinicians play an important role in identifying potential victims so they can obtain help. Here are some resources to learn more about human trafficking. • “Addressing human trafficking in the health care setting” is an online course that includes a…

Turning programs are essential to prevent and promote healing of pressure ulcers and to prevent the many negative effects of immobility, ranging from constipation to respiratory infections. However, turning a patient often puts a caregiver’s body in an awkward position, which can lead to musculoskeletal damage, especially back injuries. According to the U.S. Bureau of Labor Statistics, healthcare workers suffer…

Nearly all clinicians know exercise is good for our physical and mental health. But incorporating it into our busy lives can be a challenge. The only types of exercise some clinicians have time for are working long shifts, juggling life’s demands, balancing the books, jumping on the bandwagon, climbing the ladder of success, and skipping meals. Clinicians are in a…

Support surfaces are consistently recommended for the prevention and treatment of pressure ulcers. So patients can derive optimal benefits from support surfaces, clinicians must understand how to use them effectively. This article answers several questions about these useful tools.
Topical application of silver nitrate is often used in wound care to help remove and debride hypergranulation tissue or calloused rolled edges in wounds or ulcerations. It’s also an effective agent to cauterize bleeding in wounds. Silver nitrate is a highly caustic material, so it must be used with caution to prevent damage to healthy tissues.
Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement you’d feel. What if you had to live through this experience repeatedly? That’s what many elderly people go through, suffering with skin tears through no fault of their own. Some go on to develop complications. A skin tear is a traumatic wound caused by shear, friction, or blunt-force trauma that results in a partial-…

Optimizing nutritional status is a key strategy both in preventing and managing pressure ulcers. In patients across all care settings, compromised nutrition— as from poor intake, undesired weight loss, and malnutrition—increases the risk of pressure ulcers. It contributes to altered immune function, impaired collagen synthesis, and decreased tensile strength. In many cases, malnutrition also contributes to wound chronicity and increases the risk for delayed and impaired wound healing. In patients with chronic…

According to the National Cancer Institute, an estimated 1.6 million new cases of cancer will have been diagnosed in the United States in 2015. During the course of their disease, most cancer patients receive radiation therapy.
Delivering high energy in the form of waves or particles, radiation therapy alters the DNA of cancer cells, causing their death. Radiation can be administered either externally or internally (through materials placed into the body). It’s given in fraction doses, with the total recommended dose divided into daily amounts. Treatment, including the total dose, is determined on an individual basis.
Although improvements have been made in delivery of radiation therapy, approximately 95% of patients who receive it experience a skin reaction. What’s more, radiation therapy commonly is given concurrently with chemotherapy or targeted therapy to improve survival, which increases the toxicity risk. (more…)
Read More
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when cells meet (contact inhibition). The ideal wound edge is attached to and flush with the wound bed, moist and open with the epithelial rim thin, and pale pink to translucent. (more…)
Read More

Attending a professional conference can yield many benefits if you follow these 10 tips. 1 Obtain new knowledge. Conferences provide opportunities for clinicians to gain new knowledge about procedures, technology, and research. Take notes and keep handouts for reference. After you return, share what you have learned with colleagues so multiple people benefit from the conference. Remember to complete the necessary information to obtain professional continuing education (CE) credit. 2 Become certified.…
Just when we think we’ve figured out pressure ulcer staging, it changes again. In April 2016, the National Pressure Ulcer Advisory Panel (NPUAP) held a consensus conference on staging definitions and terminology. The purpose: to analyze and discuss the rationale for the panel’s changes. One of the key changes is replacing the term “pressure ulcer” with “pressure injury.” So instead of calling it a pressure ulcer staging system, NPUAP will…

Using maggots to treat wounds dates back to 1931 in this country. Until the advent of antibiotics in the 1940s, maggots were used routinely. In the 1980s, interest in them revived due to the increasing emergence of antibiotic-resistant bacteria. At Select Specialty Hospital Houston in Texas, we recently decided to try maggot therapy for a patient with a particularly difficult wound. In this case study, we share our experience.
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when…

Moldable skin barrier effective for elderly patients with ostomy A study in Gastroenterology Nursing reports that compared to a conventional skin barrier, a moldable skin barrier significantly improves self-care satisfaction scores in elderly patients who have a stoma. The moldable skin barrier also caused less irritant dermatitis and the costs for leakage-proof cream were lower. “The application of a moldable skin barrier in the self-care of elderly ostomy patients” included…

This issue we focus on resources to help clinicians protect themselves from injuries and engage in a healthier lifestyle. OSHA safety website A hospital is one of the most hazardous places to work, according to the Occupational Safety and Health Administration (OSHA). The agency provides a wealth of information on how to protect hospital workers as part of its website Worker Safety in Hospitals: Caring for Our Caregivers. PDF…
For an ostomy pouching system to adhere properly, the skin around the stoma must be dry and intact. Otherwise, peristomal skin problems and skin breakdown around the stoma may occur. In fact, these problems are the most common complications of surgical stomas. They can worsen the patient’s pain and discomfort, diminish quality of life, delay rehabilitation, increase use of ostomy supplies, and raise healthcare costs. Peristomal skin problems also perpetuate a…

Why would a patient with a wound spend almost 2 hours a day, 5 days a week, in a locked chamber receiving 100% oxygen? The answer is that medical grade hyperbaric oxygen therapy (HBOT) can be a valuable adjunct therapy for selected types of wounds. In this article, I’ll focus on hospitals and clinics that follow guidelines from the Undersea…
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT Every year, 1.9% of patients with diabetes develop foot ulcers. Of those, 15% to 20% undergo an amputation within 5 years of ulcer onset. During their lifetimes, an estimated 25% of diabetic patients develop a foot ulcer. This article discusses use of hyperbaric oxygen therapy (HBOT)…
According to the National Cancer Institute, an estimated 1.6 million new cases of cancer will have been diagnosed in the United States in 2015. During the course of their disease, most cancer patients receive radiation therapy. Delivering high energy in the form of waves or particles, radiation therapy alters the DNA of cancer cells, causing their death. Radiation can be administered either externally or internally (through materials placed into the body). It’s…

Antibiotic resistance is a pressing public health threat not only in the United States, but worldwide. According to the World Health Organization (WHO), it is one of the major threats to human health. Despite these concerns, antibiotics continue to be widely used—and overused. In long-term care, for instance, antibiotics are the most frequently prescribed medications, with as many as 70% of residents receiving one or more courses per year.…
Which statement about hyperglycemia and mortality in patients receiving nutritional support is correct?
a. Compared to parenteral nutrition (PN), general nutrition (EN) increases hyperglycemia risk nearly twofold.
b. Compared to EN, PN increases hyperglycemia risk nearly twofold.
c. Patients whose blood glucose (BG) level stays above 220 mg/dL during PN therapy have an increased risk of death.
d. Patients whose blood glucose (BG) level stays above 220 mg/dL during PN therapy have a decreased risk of death.
Correct answer: b. Experts estimate that up to 30% of patients receiving EN and more than 50% of those receiving PN develop hyperglycemia, defined as a BG level above 200 mg/ dL. Compared to EN, PN increases hyperglycemia risk nearly twofold, even when caloric intake is similar. One study found inadequate glucose control both before and during nutrition therapy predicted a higher mortality risk.
Learn more by reading “Supplemental nutrition in hospitalized patients with diabetes“
Read More
Nearly all clinicians know exercise is good for our physical and mental health. But incorporating it into our busy lives can be a challenge. The only types of exercise some clinicians have time for are working long shifts, juggling life’s demands, balancing the books, jumping on the bandwagon, climbing the ladder of success, and skipping meals.
Clinicians are in a unique position to help patients change their behavior to improve their health. Ironically, the first behavior clinicians need to change is to work toward improving our own exercise habits. (more…)
Read More
Optimizing nutritional status is a key strategy both in preventing and managing pressure ulcers. In patients across all care settings, compromised nutrition— as from poor intake, undesired weight loss, and malnutrition—increases the risk of pressure ulcers. It contributes to altered immune function, impaired collagen synthesis, and decreased tensile strength. In many cases, malnutrition also contributes to wound chronicity and increases the risk for delayed and impaired wound healing. In patients with chronic wounds, such as pressure ulcers, a chronic inflammatory state can induce catabolic metabolism, malnutrition, and dehydration. (more…)
Read More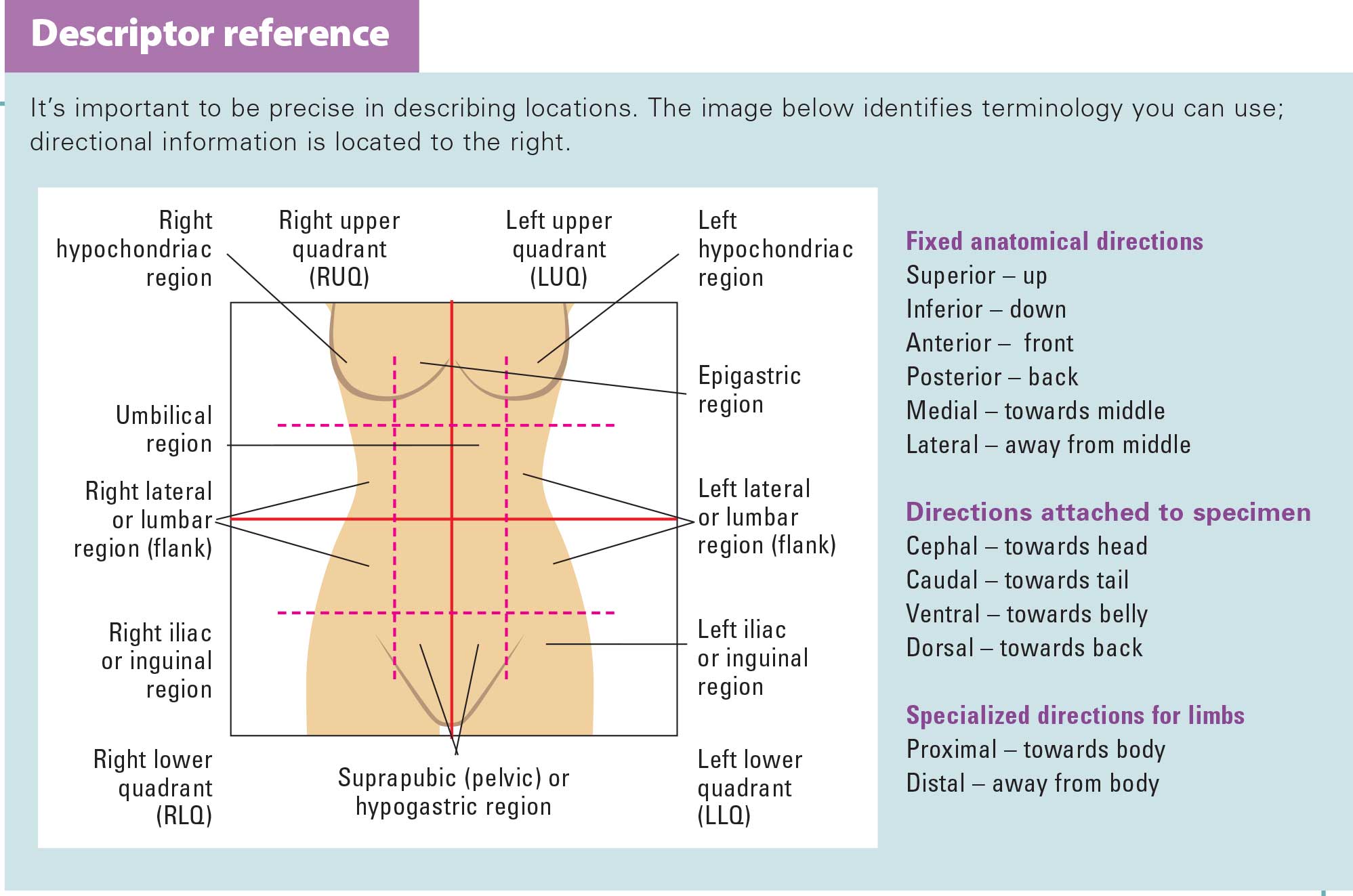{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}