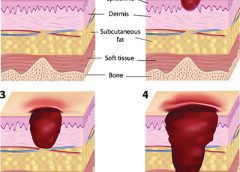
A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI), a unique staging category for a pressure ulcer. Otherwise, a clinician might think a pressure ulcer is getting worse instead of the change being the normal progression of a pressure ulcer that is presenting as a DTI.
By: Donna Sardina, RN, MHA, WCC, CWCMS What do the Los Angeles Lakers, Green Bay Packers, Montreal Canadiens, and New York Yankees have in common? All three have “three-peated”, meaning they have won three consecutive championships. This year, we at Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy (NAWCO), mark our own three-peat—our…
Mild compression diabetic socks safe and effective for lower extremity edema Diabetic socks with mild compression can reduce lower extremity edema in patients with diabetes without adversely affecting arterial circulation, according to a randomized control trial presented at the American Diabetes Association 75th Scientific Sessions Conference.
The resources below will help you address issues in your practice. NPUAP position statement on hand check for bottoming out Use of the hand check to determine “bottoming out” of support systems should be limited to static air overlay mattresses, according to a position statement from the National Pressure Ulcer Advisory Panel (NPUAP).
By Jennifer Oakley, BS, RN, WCC, DWC, OMS It’s time again for annual staff education, and you, the certified wound clinician, need to teach the staff at your organization. You dream of staff entering a state-of-the-art classroom with computers at each station, mannequins, wound anatomy models, and enough products for each student to do hands-on demonstrations. But when you open…
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI),…
By Cindy Barefield, BSN, RN-BC, CWOCN Like many hospitals, Houston Methodist San Jacinto Hospital uses national benchmarks such as the National Database of Nursing Quality Indicators (NDNQI®) to measure quality outcomes. Based on benchmark reports that showed an increased trend of pressure ulcers in critically ill patients in our hospital, the clinical nurses in our Critical Care Shared Governance Unit-Based…
By Beth Hoffmire Heideman, MSN, RN No one wants an ostomy, but sometimes it’s required to save a patient’s life. As ostomy specialists, our role is to assess and intervene for patients with a stoma or an ostomy to enhance their quality of life. We play an active role in helping patients perform self-care for their ostomy and adjust to…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Exudate (drainage), a liquid produced by the body in response to tissue damage, is present in wounds as they heal. It consists of fluid that has leaked out of blood vessels and closely resembles blood…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Medical gauze, a bleached white cloth or fabric used in bandages, dressings, and surgical sponges, is the most widely used wound care dressing. Commonly known as “4×4s,” gauze is made from fibers of cotton, rayon,…
By Gail Rogers Hebert, MS, RN, CWCN, WCC, DWC, OMS, LNHA The World Health Organization defines palliative care as “an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other…
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson, PhD, RN; and Keith Swanson, MD Cellulitis is an acute, painful, and potentially serious spreading bacterial skin infection that affects mainly the subcutaneous and dermal layers. Usually of an acute onset, it’s marked by redness, warmth, swelling, and tenderness. Borders of the affected skin…
As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to support and direct the care of pediatric patients with pressure ulcers. This article describes efforts to reduce pressure ulcers in pediatric patients at Driscoll Children’s Hospital (DCH) in Corpus Christi, Texas.
By Erin Fazzari, MPT, CLT, CWS, DWC Have you seen legs like these in your practice? These legs show lymphedema and chronic wounds before treatment (left image) and after treatment (right image) with complex decongestive therapy (CDT)—the gold standard of lymphedema care. The patient benefited from multidisciplinary collaboration between wound care and lymphedema therapists.
By Todd Zortman, RN, WCC, and James Malec, PhD Pressure ulcers are a chronic healthcare burden for both patients and providers. Over 2.5 million patients in the United States are affected annually by pressure ulcers, with nearly 60,000 of those cases directly resulting in death. From a provider’s perspective, the cost of individual care ranges anywhere from $500 to $70,000…
By Janet Wolfson, PT, CWS, CLT-LANA After landing my dream job as the wound care coordinator at an inpatient rehabilitation facility (IRF), I found myself trying to determine how much healing could be achieved for our more challenging patients, given the constraints of reimbursement and what can be done in the typical 10 to 14 days of a patient stay.…
Leg revascularization fails to improve outcomes in nursing home patients Lower-extremity revascularization often fails to improve outcomes in nursing home patients, according to an article in JAMA Internal Medicine. “Functional outcomes after lower extremity revascularization in nursing home residents: A national cohort study” found that few patients are alive and ambulatory a year after surgery, and those who are alive…
Check out these resources for your practice. Be a nutrition champion One in three patients enters a hospital malnourished. Fight malnutrition by viewing six short videos from the Alliance to Advance Patient Nutrition, including “Rapidly Implement Nutrition Interventions” and “Recognize and Diagnose All Patients at Risk of Malnutrition.” The videos show how to collaborate with the care team to become…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of performing a comprehensive skin assessment. In the healthcare setting, a comprehensive skin assessment is a process in which the entire skin of a patient is examined for abnormalities. It requires looking…
By Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Pressure ulcers have been a health concern for a long time—since at least 5,000 years ago, when evidence of a pressure ulcer was found on an ancient Egyptian mummy. But not until 1975 did the staging classification system we’re familiar with begin. This system was designed to make things easier by…
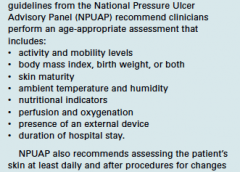
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular…
By Sharon Morrison, MAT, RN Michael had diabetes and a history of elevated blood glucose levels. A long-time drinker, he seemed to have no interest in giving up the habit. I met him while working as a diabetes nurse educator for the Boston Health Care for the Homeless Program, traveling from shelter to shelter to help persons with diabetes set…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to…
As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to support and direct the care of pediatric patients with pressure ulcers. This article describes efforts to reduce pressure ulcers in pediatric patients at Driscoll Children’s Hospital (DCH) in Corpus Christi, Texas. (more…)
By Darlene Hanson, PhD, RN; Diane Langemo, PhD, RN, FAAN; Patricia Thompson, MS, RN; Julie Anderson, PhD, RN; and Keith Swanson, MD
Cellulitis is an acute, painful, and potentially serious spreading bacterial skin infection that affects mainly the subcutaneous and dermal layers. Usually of an acute onset, it’s marked by redness, warmth, swelling, and tenderness. Borders of the affected skin are characteristically irregular. Although cellulitis may occur in many body areas, this article discusses the most common location—the lower limb. (more…)
Like many hospitals, Houston Methodist San Jacinto Hospital uses national benchmarks such as the National Database of Nursing Quality Indicators (NDNQI®) to measure quality outcomes. Based on benchmark reports that showed an increased trend of pressure ulcers in critically ill patients in our hospital, the clinical nurses in our Critical Care Shared Governance Unit-Based Council (CCSGUBC) identified an improvement opportunity. (more…)
The author describes how to overcome challenges to effective communication in the healthcare setting.
Accurate communication among healthcare professionals can spell the difference between patient safety and patient harm. Communication can be a challenge, especially when done electronically. With an e-mail or a text, you can’t hear the other person’s voice or see the body language, so it’s easy to misinterpret the words. (more…)
I’m one of the nurses responsible for the pressure ulcer prevention education program at the 150-bed skilled nursing facility where I work. We try to keep education sessions simple, fun, and interactive. One day, our administrator asked us to develop a crossword puzzle and “minute to win it” education game that would be appropriate for all staff—registered nurses, licensed practical nurses, certified nursing assistants, and staff from administration, the business office, scheduling, maintenance, dietary, and housekeeping. (more…)
A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI), a unique staging category for a pressure ulcer. Otherwise, a clinician might think a pressure ulcer is getting worse instead of the change being the normal progression of a pressure ulcer that is presenting as a DTI. (more…)
It’s time again for annual staff education, and you, the certified wound clinician, need to teach the staff at your organization. You dream of staff entering a state-of-the-art classroom with computers at each station, mannequins, wound anatomy models, and enough products for each student to do hands-on demonstrations. But when you open your eyes, you’re sitting in a room with ordinary tables and chairs, your laptop, a screen, a brain full of knowledge, and a very tight budget. (more…)
Providers are often surprised at how pages upon pages of documentation in a patient’s health record can result in few reportable diagnosis and/or procedure codes, which often fail to capture the complexity of the patient’s condition. However, providers need to be aware of the implications of coding. As healthcare data become increasingly digital through initiatives such as meaningful use, coded data not only impact reimbursement but also are increasingly used to represent the quality of care provided. Here’s a closer look at how documentation and coding work in the context of wound care. (more…)
The Affordable Care Act of 2010 requires nursing homes to have an acceptable Quality Assurance and Performance Improvement (QAPI) plan within a year after the start of the QAPI regulation. While the implementation of this regulation may be a year out, now is the time to start applying its principles. Reducing pressure ulcer rates is a great program to target for a QAPI plan.
A team approach
If you decide to use pressure ulcers as your QAPI project, don’t take on your entire program at once. Break the program down into system subsets (for example, admission process, prevention program, and weekly rounds). Determining the status of your program in each subset—completed, needs improvement, or not completed—can help you prioritize which areas to target. It’s important you have support from leadership for your efforts.
I’ll use the example of the admission phase (ensuring that within the first 24 hours, skin and risk concerns are identified and a temporary plan of care is implemented) to illustrate a QAPI project. To address this area, a team was created, including representation from staff members involved with the admission process. The team then used the problem-solving model Plan-Do-Study-Act (PDSA) to examine the process.
The first step in the PDSA cycle is to Plan. During this step, you:
• evaluate and analyze the current process to determine baseline data, which are used to measure progress
• identify system performance gaps
• determine the root cause of the performance gaps
• develop an action plan that identifies the goals, steps, responsible staff, and target dates.
In our example, the team determined that within the first 24 hours, skin inspections were being completed only 10% of the time. The root-cause analysis revealed that the admission nurses didn’t feel competent to document identified pressure ulcers or skin concerns, so they deferred it until the wound nurse was available. The team’s action plan included the following:
• Develop and educate all the facility nurses on how to complete and accurately document a skin inspection.
• Develop and implement a competency evaluation to assess the nurse’s ability to apply the knowledge at the bedside.
• Develop an ongoing plan to ensure all nurses receive this education during orientation and yearly thereafter.
The team also set the following goal:
By the end of the next quarter, 100% of admitted patients will have an accurate skin inspection completed within 24 hours of admission.
The second step of the PDSA cycle is Do. During this step, you implement and execute the plan, while documenting your observations and recording data.
In our example, the “Do” was to:
• develop and provide the skin inspection education and bedside competency evaluations
• develop an evaluation and tracking
system
• add the education to the orientation program
• add the education to the staff development calendar to be offered yearly.
The third step of the PDSA cycle is to Study: In this phase, you:
• reevaluate and analyze the system
• compare the results with the baseline data and predictions
• summarize what was learned and accomplished and what needs to be improved
• determine if another PDSA cycle is
necessary to continue to improve the system.
Once all staff had been properly educated and competency testing completed, an analysis of the rate and accuracy of the admission skin inspections done within 24 hours of admission was completed. It was found that 100% of the patients admitted had a complete skin inspection done within 24 hours. However, not all the nurses could accurately stage pressure ulcers, so it was determined that the system needed improvement to ensure accurate assessments.
The last step of the PDSA cycle is to Act. In this step, you:
• determine what changes need to be made
• modify the plan to continue to improve the system
• repeat the PDSA cycle as necessary.
In our example, the team determined the nurses needed more guidance and education on staging of pressure ulcers. Therefore, a new PDSA cycle was set to ensure the nurses are competent in this area.
Benefits for staff and patients
It may be difficult to start the QAPI project and at times the process may be stressful, but keep in mind that a successful pressure ulcer QAPI project can improve not only the quality of life and care of your patients but also morale and team building for your staff. n
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has beenspecializing in wound prevention and management since 1990.