The ability to understand or “read” lower-extremity redness in your patient is essential to determining its cause and providing effective treatment. Redness can occur in multiple conditions—hemosiderin staining, lipodermatosclerosis, venous dermatitis, chronic inflammation, cellulitis, and dependent rubor. This article provides clues to help you differentiate these conditions and identify the specific cause of your patient’s lower-extremity redness. (more…)
The Affordable Care Act of 2010 requires nursing homes to have an acceptable Quality Assurance and Performance Improvement (QAPI) plan within a year after the start of the QAPI regulation. While the implementation of this regulation may be a year out, now is the time to start applying its principles. Reducing pressure ulcer rates is a great program to target for a QAPI plan.
A team approach
If you decide to use pressure ulcers as your QAPI project, don’t take on your entire program at once. Break the program down into system subsets (for example, admission process, prevention program, and weekly rounds). Determining the status of your program in each subset—completed, needs improvement, or not completed—can help you prioritize which areas to target. It’s important you have support from leadership for your efforts.
I’ll use the example of the admission phase (ensuring that within the first 24 hours, skin and risk concerns are identified and a temporary plan of care is implemented) to illustrate a QAPI project. To address this area, a team was created, including representation from staff members involved with the admission process. The team then used the problem-solving model Plan-Do-Study-Act (PDSA) to examine the process.
The first step in the PDSA cycle is to Plan. During this step, you:
• evaluate and analyze the current process to determine baseline data, which are used to measure progress
• identify system performance gaps
• determine the root cause of the performance gaps
• develop an action plan that identifies the goals, steps, responsible staff, and target dates.
In our example, the team determined that within the first 24 hours, skin inspections were being completed only 10% of the time. The root-cause analysis revealed that the admission nurses didn’t feel competent to document identified pressure ulcers or skin concerns, so they deferred it until the wound nurse was available. The team’s action plan included the following:
• Develop and educate all the facility nurses on how to complete and accurately document a skin inspection.
• Develop and implement a competency evaluation to assess the nurse’s ability to apply the knowledge at the bedside.
• Develop an ongoing plan to ensure all nurses receive this education during orientation and yearly thereafter.
The team also set the following goal:
By the end of the next quarter, 100% of admitted patients will have an accurate skin inspection completed within 24 hours of admission.
The second step of the PDSA cycle is Do. During this step, you implement and execute the plan, while documenting your observations and recording data.
In our example, the “Do” was to:
• develop and provide the skin inspection education and bedside competency evaluations
• develop an evaluation and tracking
system
• add the education to the orientation program
• add the education to the staff development calendar to be offered yearly.
The third step of the PDSA cycle is to Study: In this phase, you:
• reevaluate and analyze the system
• compare the results with the baseline data and predictions
• summarize what was learned and accomplished and what needs to be improved
• determine if another PDSA cycle is
necessary to continue to improve the system.
Once all staff had been properly educated and competency testing completed, an analysis of the rate and accuracy of the admission skin inspections done within 24 hours of admission was completed. It was found that 100% of the patients admitted had a complete skin inspection done within 24 hours. However, not all the nurses could accurately stage pressure ulcers, so it was determined that the system needed improvement to ensure accurate assessments.
The last step of the PDSA cycle is to Act. In this step, you:
• determine what changes need to be made
• modify the plan to continue to improve the system
• repeat the PDSA cycle as necessary.
In our example, the team determined the nurses needed more guidance and education on staging of pressure ulcers. Therefore, a new PDSA cycle was set to ensure the nurses are competent in this area.
Benefits for staff and patients
It may be difficult to start the QAPI project and at times the process may be stressful, but keep in mind that a successful pressure ulcer QAPI project can improve not only the quality of life and care of your patients but also morale and team building for your staff. n
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has beenspecializing in wound prevention and management since 1990.
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found that using hybrid 67Ga single-photon emission computed tomography and X-ray computed tomography (SPECT/CT) imaging combined with a bedside percutaneous bone puncture in patients with a positive scan is “accurate and safe” for diagnosing osteomyelitis in patients with diabetes who have a foot ulcer without signs of soft-tissue infection.
The new method, which avoids an invasive bone biopsy, has a sensitivity of 88% and a specificity of 93.6%. In the study of 55 patients, antibiotic treatment was avoided in 55% of suspected cases.
MRSA strains will likely continue to coexist in hospitals and communities
The strains of methicillin-resistant Staphylococcus aureus (MRSA) differ in the hospital and community settings, and both are likely to coexist in the future, according to a study in PLOS Pathogens.
C. difficile prevention actions fail to stop spread
Despite increasing activities to prevent the spread of Clostridium difficile, infection from C. difficile remains a problem in healthcare facilities, according to a survey of infection preventionists by the Association for Professionals in Infection Control and Epidemiology (APIC).
The survey found that 70% of preventionists have adopted additional interventions in their healthcare facilities since March 2010, but only 42% have seen a decline in C. difficile infection rates; 43% saw no decline.
A total of 1,087 APIC members completed the survey in January 2013. The survey also found that more than 92% of respondents have increased emphasis on environmental cleaning and equipment decontamination practices, but 64% said they rely on observation, rather than more accurate and reliable monitoring technologies, to assess cleaning effectiveness.
In addition, 60% of respondents have antimicrobial stewardship programs at their facilities, compared with 52% in 2010. Such programs promote the appropriate use of antibiotics, which can help reduce the risk of C. difficile infection.
Mast cells may not play significant role in wound healing
“Evidence that mast cells are not required for healing of splinted cutaneous excisional wounds in mice,” published in PLOS One, analyzed wound healing in three types of genetically mast-deficient mice and found they reepithelialized their wounds at rates similar to control mice. At the time of closure, the researchers found that scars in all the mice groups were similar in both “quality of collagen deposition and maturity of collagen fibers.” The findings fail to support the previously held belief that mast cells are important in wound healing.
Study identifies effective casting for diabetes-related plantar foot ulcers
Nonremovable casts that relieve pressure are more effective than removable casts or dressings alone for the treatment of plantar foot ulcers caused by diabetes, according to an analysis of clinical trials.
The authors of “Pressure-relieving interventions for treating diabetic foot ulcers,” published by The Cochrane Library, reviewed 14 randomized clinical trials that included 709 participants. Nonremovable pressure-relieving casts were compared to dressings alone, temporary therapeutic shoes, removable pressure-relieving devices, and surgical lengthening of the Achilles tendon.
The study also notes that when combined with Achilles tendon lengthening, nonremovable devices were more successful in one forefoot ulcer study than the use of a nonremovable cast alone.
Most studies were from the United States (five) and Italy (five), with Germany, the Netherlands, Australia, and India each contributing one study.
Prescriber preference drives use of antibiotics in long-term care
The study of 66,901 patients from 630 long-term care facilities found that 77.8%
received a course of antibiotics. The most common length (41%) was 7 days, but the length exceeded 7 days in 44.9% of patients. Patient characteristics were similar among short-, average-, and long-duration prescribers.
The study authors conclude: “Future trials should evaluate antibiotic stewardship interventions targeting prescriber preferences to systematically shorten average treatment durations to reduce the complications, costs, and resistance associated with antibiotic overuse.”
Electrophysical therapy may be helpful for diabetic foot ulcers
The authors of the study in International Wound Journal reviewed eight trials with a combined total of 325 patients. Five studies were on electrical stimulation, two on phototherapy, and one on ultrasound. Because of the small number of trials, the possibility of harmful effects can’t be ruled out, and the authors recommend “high-quality trials with larger sample sizes.”
Significant geographic variations in spending, mortality exist for diabetic patients with foot ulcers and amputations
The study in Journal of Diabetes and Its Complications found that higher spending wasn’t associated with a significant reduction in 1-year patient mortality. In addition, rates of hospital admission were associated with higher per capita spending and higher mortality rates for patients.
Home-based exercise program improves life for lymphedema patients
An individualized, home-based progressive resistance exercise program improves upper-limb volume and circumference and quality of life in postmastectomy patients with lymphedema, according to a study published in the Journal of Rehabilitation Research and Development.
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
By Rosalyn Jordan, RN, BSN, MSc, CWOCN, WCC, and Marci Christian, BBE
Any patient with a fecal or urinary ostomy may experience complications on the skin surface around the stoma. These complications may occur lifelong, although they’re more common during the first 5 years after the initial ostomy surgery. Causative factors include infection, trauma, certain diseases, and chemical irritation; most of these problems stem from the pouching system or pouch leakage.
Peristomal skin complications can cause a wide range of signs and symptoms, from skin discoloration to polyp-like growths, from erythema to full-thickness wounds. They can lead to discomfort, pain, poor self-image, social isolation, and impaired quality of life, not to mention additional care costs.
Incidence and types of these complications are hard to compare or contrast across multiple patients. Until recently, no standardized assessment or documentation tools were available to characterize or define complications. For this reason, reported rates ranged widely, from 10% to 70%. And because no designated common language or categories related to peristomal skin complications existed, documentation was inconsistent.
In the late 2000s, a group of nurses experienced in caring for ostomy patients worked with the World Council of Enterostomal Therapists to develop a resource called the Ostomy Skin Tool, which clinicians can use to categorize and describe peristomal skin complications in a consistent, objective manner. The tool also provides a common language for documentation.
The Ostomy Skin Tool has three major assessment domains—discoloration (D), erosion/ulceration (E), and tissue overgrowth (T), known collectively as DET. The DET combined rating ranges from normal, rated 0, to the worst condition possible, rated 15. Mild DET complications are documented as less than 4, moderate as less than 7, and severe as 8 or higher. (See Using the Ostomy Skin Tool by clicking the PDF icon above.)
The tool describes four categories of peristomal complications:
• chemical irritation
• mechanical trauma
• disease-related complications
• infection-related complications.
Chemical irritation
Chemical irritation can stem from irritants (as in contact dermatitis) or allergic reactions (allergic dermatitis). The most likely cause of chemical dermatitis is effluent leakage (feces or urine) from the colostomy, ileostomy, or urostomy, in which effluent comes in contact with peristomal skin. Other potential causes include contact with soap, certain adhesives, and adhesive removers.
The major treatment of chemical irritation is identification and removal of the offending agent, followed by patient and caregiver education on the new pouching procedure the patient must use. Follow-up assessment also is recommended. In a 2010 study that followed 89 patients for 1 year after ostomy surgery, about 50% of subjects experienced peristomal skin complications, most of them from pouch leakage. Another investigator estimated that 85% of ostomy patients experience pouch leakage at some time during their lives. Pouch leakage usually occurs when stool is extremely liquid (for instance, ileostomy effluent). Other causes of pouch leakage include wearing a pouch more than half full of effluent and abdominal contours that aren’t level. Besides changes in the pouching system, treatment may entail adding products to the pouching system or removing certain agents.
Some patients experience allergic dermatitis in reaction to products used in the pouching system (such as skin barriers, belts, pouch closures, or adhesives). However, allergic dermatitis is rare. One 2010 study suggested allergic reactions to these products occur in only about 0.6% of patients with peristomal skin irritation. Most major ostomy product manufacturers provide a patch test on request to help identify allergic conditions. Once the offending product is discontinued, allergic dermatitis should resolve rapidly.
Mechanical trauma
Mechanical trauma usually results from either the pouching system itself or its removal. It also may result from harsh or multiple skin-barrier removals, pressure from convex rings or pouches, and abrasive cleansing techniques. Some researchers believe the stronger the adhesive barrier and the more often a pouch is changed, the greater the risk of epidermal damage.
Mechanical trauma may present as a partial-thickness ulcer caused by pressure, shear, friction, tearing, or skin stripping. Patients with fragile skin are susceptible to mechanical trauma, so less aggressive pouching systems may be preferred for them. Of course, if the pouching system is changed, the patient or caregiver needs to learn about the new system.
Disease-related complications
Disease-related peristomal complications may be linked to preexisting skin conditions, such as psoriasis, eczema (atopic dermatitis), or seborrheic dermatitis. Hyperplasia also may occur. This overgrowth of cells, which may appear as gray or reddish brown pseudoverrucous lesions, usually is linked to urinary ostomies, although it can occur with fecal ostomies as well. Vinegar soaks are the recommended treatment, in addition to a change in the pouching system and corresponding patient education.
Occasionally, other disease-related complications occur, including primary adenocarcinoma of the peristomal skin and peristomal pyoderma gangrenosum, a painful and problematic condition that presents as peristomal ulcers. Ulcer borders are well-defined with a bluish purple coloration at the edges. Infection must be ruled out, as this condition usually is linked to an autoimmune condition. Treatment includes pain management and, in most cases, a topical corticosteroid. Crohn’s disease also may manifest as a peristomal skin ulcer.
Infection-related complications
Infection-related complications may be bacterial or fungal. Two common peristomal skin infections are folliculitis and Candida fungal infections. An infection of the hair follicle that causes pustules, folliculitis usually stems from traumatic hair pulling in the peristomal area during pouch removal. It may warrant a prescribed antibiotic, along with patient teaching regarding proper hair removal using an electric razor.
Candida infections may arise because peristomal skin provides a warm, dark, moist environment that promotes fungal growth. These infections appear as erythema with pustules or papules and satellite lesions. Treatment usually involves antifungal powder and use of the crusting technique to secure the pouching system. (See Using the crusting technique by clicking the PDF icon above.)
Management
Many complications are well advanced by the time patients seek assistance, perhaps because they don’t understand the significance of their symptoms and think they can manage the problem themselves. In some cases, they don’t know where to turn for assistance. Commonly, the complication progresses to the point where the patient goes to the emergency department or (particularly during the immediate postoperative period) needs to be readmitted for treatment. The best way to manage peristomal skin complications is to prevent them in the first place. (See Preventing peristomal skin complications by clicking the PDF icon above.)
Patient education
Over the past 20 years, hospital stays for ostomy surgery patients have decreased from about 2 weeks to less than 5 days. Reduced stays decrease the time available for caregivers to teach patients and family members how to empty and change the pouch. They need alternative education covering (among other topics) how to recognize peristomal skin complications and when to seek help. Not only do these complications require vigilant self-observation, but many patients don’t understand their implications or how rapidly they can worsen. In some cases, the first symptoms are itching and redness under the skin barrier. Fortunately, some patients may know or remember that itching, burning, stinging, reddened, or weeping peristomal skin requires professional attention. They can avoid serious complications by seeking assistance early, such as right after noticing pouch leakage.
Early treatment can reduce the cost of treatment. In a 2012 study, researchers estimated care costs related to peristomal skin complications for a 7-week treatment period, using the Ostomy Skin Tool as a reference. Severe complications (those with a DET score above 8) cost six times more to treat than mild cases (those with a DET score below 4) and 4.5 times more than moderate cases.
Along with early intervention by a trained ostomy care specialist, self-assessment by ostomy patients promotes a better quality of life, reduces pain, and may decrease care costs. Clinicians’ use of the Ostomy Skin Tool to assess and document peristomal skin complications promotes more reliable, objective, comparable assessment data for reporting.
Selected references
Al-Niaimi F, Lyon CC. Primary adenocarcinoma in peristomal skin: a case study. Ostomy Wound Manage. 2010;56(1):45-7.
Burch J. Management of stoma complications. Nurs Times. 2011;107(45):17-8, 20.
Jemec GB, Martins L, Claessens I, et al. Assessing peristomal skin changes in ostomy patients: validation of the Ostomy Skin Tool. Br J Dermatol. 2011; 164;330-5.
Jones T, Springfield T, Brudwick M, Ladd A. Fecal ostomies: practical management for the home health clinician. Home Healthc Nurse. 2011;29(5):306-17.
Martins L, Samai O, Fernandez A, et al. Maintaining healthy skin around an ostomy: peristomal skin disorders and self-assessment. Gastrointest Nurs. 2011;
9(2):9-13.
Martins L, Tavernelli K, Serrano JLC. Introducing a peristomal skin assessment tool: The Ostomy Skin Tool. World Council Enterostomal Therapists J. 2008;28(2):3-13.
Meisner S, Lehur P, Moran B, et al. Peristomal skin complications are common, expensive, and difficult to manage: a population based cost modeling study. PLoS One. 2012;7(5):e37813.
Omura Y, Yamabe M, Anazawa S. Peristomal skin disorders in patients with intestinal and urinary ostomies: influence of adhesive forces of various hydrocolloid wafer skin barriers. J Wound Ostomy Continence Nurs. 2010;37(3):289-98.
Ratliff CR. Early peristomal skin complications reported by WOC nurses. J Wound Ostomy Continence Nurs. 2010;37(5):505-10.
Shabbir J, Britton DC. Stomal complications: a literature overview. Colorectal Dis. 2010;12(10):958- 64.
Wound, Ostomy, Continence Clinical Practice Ostomy Subcommittee. Peristomal skin complications: Best practice for clinicians. Mt. Laurel, NJ; 2007.
The authors work for RecoverCare, LLC, in Louisville, Kentucky. Rosalyn Jordan is director of clinical education and Marci Christian is a clinical associate product specialist.
The elevator door opens and you step in to find yourself face to face with the important person you’ve wanted to meet to discuss your promising idea. It’s the chance you wouldn’t want to miss. But that chance lasts only as long as the elevator ride. You have less than a minute to make an impression. Do you have an elevator speech ready?
What’s an elevator speech?
An elevator speech is any short speech that sells an idea, promotes a business, or markets an individual. It’s a short summary, or pitch, that quickly describes the value of a service, product, or organization. The term is a metaphor for unexpected access to someone to whom you’d like to sell an idea or proposal. It derives from the early days of the Internet boom when web development companies needed venture capital. Firms were swamped with applications for funding, and in many cases, the companies that won the cash were those whose reps had a simple pitch and could explain a business proposal in an elevator in the time it took to ride to their floor.
A great elevator speech describes and sells an idea in less than a minute. Of course, it’s not restricted to elevators. It comes in handy any time and anywhere you need to give a concise presentation to capture someone’s interest so you can move to the next step—a follow-up call, a referral, a meeting, or a partnership.
Why clinicians need an elevator speech
You need to be able to describe what you do, what you’re interested in doing, and how you can be a resource to someone. The ability to sum up a unique aspect of your service or expertise in a way that excites others is a fundamental skill. Doing this in a brief, persuasive manner is an asset for any professional. A good elevator speech should grab one’s attention in a few words and make that person want to know more about you. Here are examples where a good elevator speech would be helpful:
• Thomas goes to a recruitment fair hoping to get an interview at a certain hospital.
• Mary is finishing her master of science degree and is interested in a position in a new wound care clinic.
• Caroline has written a book on grant writing and would like to present her ideas at a conference.
• Brian is interested in research and would like to join the research team.
• Mindy is trying to expand her wound consultation business.
You can use an elevator speech when you want to grab someone’s attention at a meeting, convention, or other social situation. In such situations, people typically ask, “What do you do?” A well-planned elevator speech can make the listener’s ears perk up and want to know more.
How to prepare an elevator speech
Before you can write an elevator speech, you need to know yourself, what you can offer, what problems you can solve, and what benefits you can bring to the prospective contact. For example, you may be an expert in professional communication and know strategies you can teach other staff to promote a better workplace environment.
You also need to know your audience. Will you direct your pitch to an administrator, a unit manager, or staff? You’re more likely to succeed if your elevator speech is targeted to a specific audience and you adjust it to that audience. Try to prepare different pitches for different audiences; a generic pitch is almost certain to fail. (See Key elements of a good elevator speech by clicking the PDF icon above.)
In today’s busy world, clinicians must be able to communicate in a succinct, persuasive manner. Your elevator speech is your introduction to others. It has to be good. Keep practicing it and perfecting it so you can speak with poise and polish. The more often you give it, the better it will become. It’s a great way to put your best foot forward when you have only a small window of opportunity to make a good impression.
Sjodin T. Small Message, Big Impact: The Elevator Speech Effect. New York, NY: Portfolio; 2012. Sprung S, Giang V. 6 keys to delivering a powerful elevator pitch. Business Insider Web site. www .businessinsider.com/terri-sjodin-how-to-deliver- an-elevator-speech-2012-10. October 26, 2012. Accessed October 26, 2012.
Kathleen D. Pagana is a keynote speaker and professor emeritus at Lycoming College in Williamsport, Pennsylvania. She is the author of The Nurse’s Communication Advantage and The Nurse’s Etiquette Advantage. She is also the coauthor of Mosby’s Diagnostic and Laboratory Test Reference, 11th ed. To contact her, visit www.KathleenPagana.com.
One of the worst fears of a wound care clinician is inadvertently compressing a leg with critical limb ischemia—a condition marked by barely enough blood flow to sustain tissue life. Compression (as well as infection or injury) could lead to necrosis, the need for amputation, or even death. The gold standard of practice is to obtain an ankle-brachial index (ABI) before applying compression. However, recent research and expert opinion indicate an elevated or normal ABI is deceptive in patients with advanced diabetes. What’s worse, in the diabetic foot, skin may die from chronic capillary ischemia even when total blood perfusion is normal. For information on how to perform an ABI and interpret results, click on this link. (more…)
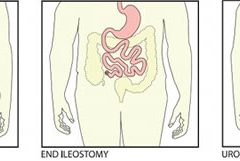
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Chronic venous insufficiency (CVI) is the most common cause of lower extremity wounds. The venous tree is defective, incapable of moving all the blood from the lower extremity back to the heart. This causes pooling of blood and intravascular fluid at the lowest gravitational point of the body—the ankle.
This article has two parts. Part 1 enhances your understanding of the disease and its clinical presentation. Part 2, which will appear in a later issue, explores the differential diagnosis of similar common diseases, the role that coexisting peripheral artery disease (PAD) may play, disease classification of venous insufficiency, and a general approach to therapy.
The most common form of lower extremity vascular disease, CVI affects 6 to 7 million people in the United States. Incidence increases with age and other risk factors. One study of 600 patients with CVI ulcers revealed that 50% had these ulcers for 7 to 9 months, 8% to 34% had them for more than 5 years, and 75% had recurrent ulcers.
Thrombotic complications of CVI include thrombophlebitis, which may range from superficial to extensive. If the thrombophlebitis extends up toward the common femoral vein leaving the leg, proximal ligation may be needed to prevent clot extension or embolization.
Understanding normal anatomy and physiology
Lower extremity veins flow horizontally from the superficial veins to the perforating veins and then into the deep veins. Normally, overall venous blood flows vertically against gravity from the foot and ankle upward toward the inferior vena cava (IVC). This antigravity flow toward the IVC results from muscular contraction around nonobstructed veins and one-way valves that close as blood passes them. These valves prevent abnormal backward blood flow toward the foot and ankle region.
The lower extremities have four types of veins. Superficial veins are located within the subcutaneous tissue between the dermis and muscular fascia. Examples are the greater and lesser (smaller) saphenous veins. Perforating veins connect the superficial veins to the deep veins of the leg. The deep veins are located below the muscular fascia. The communicating veins connect veins within the same system.
The greater saphenous vein is on the leg’s medial (inner) side. It originates from the dorsal veins on top of the foot and eventually drains into the common femoral vein in the groin region. By way of perforating veins, the greater saphenous vein drains into the deep venous system of both the calf and thigh.
The lesser saphenous vein is situated on the lateral (outer) side of the leg and originates from the lateral foot veins. As it ascends, it drains into the deep system at the popliteal vein behind the knee. Communicating veins connect the greater saphenous vein medially and the lesser saphenous vein laterally.
Intramuscular veins are the deep veins within the muscle itself, while the intermuscular veins are located between the muscle groups. The intermuscular veins are more important than other veins in development of chronic venous disease. Below the knee, the intermuscular veins are paired and take on the name of the artery they accompany—for example, paired anterior tibial, paired posterior tibial, and paired peroneal veins. Eventually, these veins form the popliteal vein behind the knee, which ultimately drains into the femoral vein of the groin.
As the common femoral vein travels below the inguinal ligament of the groin, it’s called the external iliac vein. Eventually, it becomes the common iliac vein, which drains directly into the IVC.
Pathophysiology
Abnormally elevated venous pressure stems from the leg’s inability to adequately drain blood from the leg toward the heart. Blood drainage from the leg requires the muscular pumping action of the leg onto the veins, which pump blood from the leg toward the heart as well as from the superficial veins toward the deep veins. Functioning one-way valves within the veins close when blood passes them, preventing blood from flowing backward toward the ankle. This process resembles what happens when you climb a ladder with intact rungs: As you step up from one rung to the next, you’re able to ascend.
CVI and the “broken rung” analogy
If the one-way valves are damaged or incompetent, the “broken rung” situation occurs. Think how hard it would be to climb a ladder with broken rungs: You might be able to ascend the ladder, but probably you would fall downward off the ladder due to the defective, broken rungs.
Normally, one-way valves ensure that blood flows from the lower leg toward the IVC and that the superficial venous system flows toward the deep venous system. The venous system must be patent (open) so blood flowing from the leg can flow upward toward the IVC. Blockage of a vein may result from an acute thrombosis (clot) in the superficial or deep systems. With time, blood may be rerouted around an obstructed vein. If the acute thrombosis involves one or more of the one-way valves, as the obstructing thrombosis opens up within the vein’s lumen, permanent valvular damage may occur, leading to post-thrombotic syndrome—a form of CVI.
CVI may result from an abnormality of any or all of the processes needed to drain blood from the leg—poor pumping action of the leg muscles, damage to the one-way valves, and blockage in the venous system. CVI commonly causes venous hypertension due to reversal of blood flow in the leg. Such abnormal flow may cause one or more of the following local effects:
leg swelling
tissue anoxia, inflammation, or necrosis
subcutaneous fibrosis
Compromised flow of venous blood or lymphatic fluid from the extremity.
“Water balloon” analogy
The effect of elevated venous pressure or hypertension is worst at the lowest gravitational point (around the ankle). Pooling of blood and intravascular fluid around the ankle causes a “water balloon” effect. A balloon inflated with water has a thin, easily traumatized wall. When it bursts, a large volume of fluid drains out. Due to its thicker wall, a collapsed balloon that contains less fluid is more difficult to break than one distended with water.
In a leg with CVI, subcutaneous fluid that builds up requires a weaker force to break the skin and ulcerate than does a nondistended leg with less fluid. This principle is the basis for compression therapy in treating and preventing CVI ulcers.
Effects of elevated venous pressure or hypertension
Increased pressure in the venous system causes:
abnormally high pressure in the superficial veins—60 to 90 mm Hg, compared to the normal pressure of 20 to 30 mm Hg
dilation and distortion of leg veins, because blood refluxes abnormally away from the heart and toward the lower leg and may move from the deep venous system into the superficial veins.
Abnormal vein swelling from elevated pressure in itself may impair an already abnormally functioning one-way valve. For instance, the valve may become more displaced due to the increase in intraluminal fluid, which may in turn worsen hypertension and cause an increase in leg swelling. Increased pressure from swollen veins also may dilate the capillary beds that drain into the veins; this may cause leakage of fluid and red blood cells from capillaries into the interstitial space, exacerbating leg swelling. Also, increased venous pressure may cause fibrinogen to leak from the intravascular plasma into the interstitial space. This leakage may create a fibrin cuff around the capillary bed, which may decrease the amount of oxygen entering the epidermis, increase tissue hypoxia, trigger leukocyte activation, increase capillary permeability, and cause local inflammation. These changes may lead to ulceration, lipodermatosclerosis, or both.
Visible changes may include dilated superficial veins, hemosiderin staining due to blood leakage from the venous tree, atrophie blanche, and lipodermatosclerosis. (See CVI glossary by clicking the PDF icon above.) Both atrophie blanche and lipodermatosclerosis result from local tissue scarring secondary to an inflammatory reaction of the leg distended with fluid.
Lipodermatosclerosis refers to scarring of subcutaneous tissue in severe venous insufficiency. Induration is associated with inflammation, which can cause the skin to bind to the subcutaneous tissue, causing narrowing of leg circumference. Lymphatic flow from the leg also may become compromised and inhibited in severe venous hypertension, causing additional leg swelling.
Patient history
In a patient with known or suspected CVI, a thorough history may lead to a working diagnosis. Be sure to ask the patient these questions:
Do you have pain?
Is your pain worse toward the end of the day?
Is the pain relieved with leg elevation at night?
Is it relieved with leg elevation during the day?
Do you have leg pain that awakens you at night?
How would you describe the pain?
Does the skin on your leg feel tight or irritated?
Have you noticed visible changes of your leg?
Do you have a leg ulcer?
Also determine if the patient has comorbidities that may exacerbate CVI, including PAD, renal failure, venous thrombosis, lymphedema, diabetes mellitus, heart failure, or malnutrition. (See CVI risk factors by clicking the PDF icon above .)
Common CVI symptoms
Approximately 20% of CVI patients have symptoms of the disease without physical findings. These symptoms may include:
tired, “heavy” legs that feel worse toward the end of the day
discomfort that worsens on standing
legs that feel best in the morning after sleeping or after the legs have been
elevated during the day.
Although patients may report leg discomfort, the history indicates that it doesn’t awaken them at night. Be aware that discomfort from CVI differs from that caused by PAD. With PAD, patients may report pain on exercise (claudication), pain with elevation (nocturnal pain), or constant pain (resting pain).
Signs of CVI (with or without ulcers) include:
leg swelling (seen in 25% to 75% of patients)
skin changes (such as hemosiderin staining or dermatitis)
telangiectasia, reticular veins, or both; while these are the most common signs, they represent an overall less severe finding
varicose veins with or without bleeding, occurring in one-third of patients with CVI.
Venous ulcers
Venous ulcers are the most common type of lower extremity ulcer. They’re commonly found on the medial aspect of the lower extremity, from the ankle to the more proximal calf area. Usually, they arise along the course of the greater saphenous vein, but also may be lateral and may occur at multiple locations. They aren’t found above the knee or on the forefoot. Venous ulcers are shallower than arterial ulcers and have considerable exudate consistent with drainage from a ruptured water balloon. They may extend completely around the leg.
CVI: From a heavy sensation to visible changes
In patients with CVI, blood flows within a lower extremity in an abnormal, reverse direction, causing build-up of blood and intravascular fluid around the ankle. Initially, this may cause only a sensation of heavy legs toward the end of the day, with no visible changes. Eventually, it may lead to venous ulcers or other visible changes. This abnormal blood flow results from dysfunction of the normal mechanisms that drain blood from the leg against gravity into the IVC.
Sardina D. Skin and Wound Management Course; Seminar Workbook. Wound Care Education Institute; 2011:92-112.
Donald A. Wollheim is a practicing wound care physician in southeastern Wisconsin. He also is an instructor for Wound Care Education Institute and Madison College. He serves on the Editorial Board for Wound Care Advisor.
If you’re keeping up on wound care, you know a lot of new things are coming to market with enough decent science behind them to make them reasonable options to consider in your practice. And as true-blooded Americans and citizens of the post-industrialized world, we want what’s newest, fastest, and best in class in everything. It’s just our nature.
But does it truly serve us to be eager to try new therapies even when the current treatment plan is successful? Perhaps. We know we must never close our eyes to new developments in our field that can lead to better outcomes. Knowing when and what to change can lead to better outcomes for the patient, the wound, and our collective pocketbook.
I’ve long maintained we can achieve excellent-quality wound care if we just stick to the basics the vast majority of the time. Why? Systemic, psychosocial, and local factors all affect wound healing—not just the dressing or cream. Our job is to provide the optimum environment possible for wound healing. That requires us to look at and support the whole body toward optimum health, not solely the wound.
The basics begin with identifying the cause of the wound and implementing interventions to reduce, control, or eliminate the cause. Next, we strive to manage local and psychosocial factors by choosing topical products that will maintain moisture balance, keep the wound warm, and protect it. If the wound doesn’t show progress toward healing within 2 weeks (or as expected, given the patient’s overall condition and ability to heal), we need to reevaluate the plan and begin making changes.
The best rule is to make one change at a time. That makes it much easier to determine what’s working and what isn’t. Once all the basics are in place and required changes have been made, if healing is still stalled or nonexistent, consider trying the available new products and specialty products.
Never close your clinical mind to advances in the field. To do that would be a disservice to your patients. But you should change the treatment plan only when a change is needed—not just for the sake of changing it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
The number of people with diabetes who are meeting the ABC goals—hemoglobin A1C, blood pressure, and LDL cholesterol—has risen significantly in recent years, according to a study published by Diabetes Care. Patients meeting all three goals rose from about 2% in 1988 to about 19% in 2010.
Gains were made in each of the ABC goals, based on 2007 to 2010 data: 53% of patients met A1C goals, compared to 43% in 1988 to 1994 data; 51% met blood pressure goals, compared to 33%; and 56% met LDL goals, compared to 10%.
Younger people were less likely to meet A1C and cholesterol goals. Compared with non-
Hispanic whites, Mexican Americans were less likely to meet A1C and LDL goals and non-Hispanic blacks were less likely to meet blood pressure and LDL goals.
The researchers analyzed data from the National Health and Nutrition Examination Surveys from 1988–1994, 1999–2002, 2003–2006, and 2007–2010. Nearly 5,000 people age 20 or older participated.
Although progress had been made, the researchers conclude, “Despite significant improvement during the past decade, achieving the ABC goals remains suboptimal among adults with diabetes, particularly in some minority groups.”
Daily bathing with chlorhexidine-impregnated washcloths reduces infection risk
A study in The New England Journal of Medicine reports that daily bathing with chlorhexidine-impregnated washcloths reduces the risk of becoming infected with multidrug-resistant organisms and subsequent development of hospital-acquired bloodstream infections in intensive care unit patients.
“Effect of daily chlorhexidine bathing on hospital-acquired infection” included 7,727 patients in nine intensive care and bone marrow units in six hospitals. The units were randomly assigned to bathe patients with either no-rinse 2% chlorhexidine-impregnated washcloths or nonantimicrobial washcloths for 6 months; then, the units switched to the opposite product for 6 months.
The rate of infection with multidrug-resistant organisms was 23% lower in the chlorhexidine group and the rate of hospital-acquired bloodstream infection was 28% lower in the chlorhexidine group.
Patients tend not to wear custom-made footwear for preventing diabetic foot ulcers
Adherence to wearing prescription custom-made footwear was low among patients with diabetes, neuropathy, and a recently healed plantar foot ulcer, according to a study in Diabetes Care. The low adherence was particularly notable at home, where patients did the most walking.
Factors associated with higher adherence included lower body mass index, more severe foot deformity, and more appealing footwear.
Tedizolid works as well as linezolid in patients with acute bacterial skin infections
A JAMA study says that a 200-mg once-daily dose of oral tedizolid phosphate over 6 days was as effective as 600 mg of oral linezolid every 12 hours for 10 days in patients with acute bacterial skin and skin-structure infections, including cellulitis or erysipelas, major cutaneous abscesses, and wound infections.
A shorter course of tedizolid may be a “reasonable alternative” to linezolid for treating acute bacterial skin and skin-structure infections, the study concludes.
Water-based exercise improves ROM in patients with long-term arm lymphedema
A study of breast cancer survivors (median 10 years after surgery) with lymphedema found that a water-based exercise program improved shoulder range of motion (ROM).
The program consisted of at least twice-weekly water-based exercise for 8 weeks. At first, participants were supervised, but later they exercised independently. Although lymphedema status didn’t change, those who performed water-based exercise had an increase in ROM, showing improvement years after surgery.
Dehydrated amniotic membrane allograft possible option for treating chronic wounds
A dehydrated amniotic membrane allograft (EpiFix) was used to treat four patients whose wounds hadn’t closed after conservative and advanced measures and who had been referred for plastic procedures. A variety of wounds healed (located on the elbow, knee, hand, and ankle) after one to three applications of the amniotic material, which patients tolerated well. The wounds remained closed several months later.
Study casts doubt on MLD’s role in breast cancer–related lymphedema
A meta-analysis published in the World Journal of Surgical Oncology found the “current evidence” from randomized clinical trials “does not support” the use of manual lymphatic drainage (MLD) in preventing or treating lymphedema in patients with breast cancer.
The authors analyzed 10 randomized clinical trials with 566 patients.
CDC issues additional prevention steps for carbapenem-resistant Enterobacteriaceae
On Feb. 14, the Centers for Disease Control and Prevention (CDC) issued additional prevention steps for carbapenem-resistant Enterobacteriaceae (CRE). Increased reports of CRE prompted the action: Of the 37 unusual forms of CRE reported in the U.S., the last 15 have been reported since July 2012.
• When a CRE is identified in a patient with a history of an overnight stay in a healthcare facility (within the last 6 months) outside the U.S., send the isolate to a reference laboratory for confirmatory susceptibility testing and test to determine the carbapenem resistance mechanism.
• For patients admitted to healthcare facilities in the U.S. after recently being hospitalized (within the last 6 months) in countries outside the U.S., consider performing rectal screening cultures to detect CRE colonization, and place patients on contact precautions while awaiting the results.
Examples of Enterobacteriaceae include Klebsiella species and Escherichia coli. CRE are Enterobacteriaceae with high levels of resistance to antibiotics, including carbapenems. CRE infections most commonly occur among patients who are receiving antibiotics and significant medical treatment for other conditions.
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)