http://www.swbrinc.com/pressroom/read.php?aid=867
Read MoreSearch Results for: w
Ostomy 101: Colostomy, ileostomy, and urostomy
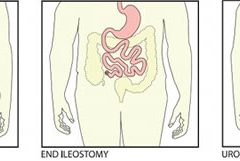
By Jackie Doubleman, BSN, RN, CWOCN
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Read MoreClinician Resources

Here are resources that can help you in your busy clinical practice by giving you information quickly.
Pressure ulcer resources
Instead of searching through Google or another search engine for pressure ulcer resources, start with this comprehensive list on the Centers for Medicare & Medicaid Services website.
Examples of resources included are:
- “Preventing pressure ulcers in hospitals: A toolkit for improving quality of care.” This toolkit from the Agency for Healthcare Research and Quality (AHRQ) is designed to help hospitals in implementing pressure ulcer prevention strategies.
- “On-time pressure ulcer healing project.” Another AHRQ initiative, this resource is designed for those working in long-term care facilities.
- “Pressure ulcer prevention.” This table from the Institute for Healthcare Improvement lists possible mentors you can work with in the area of ulcer prevention.
- “Shawnee Medical Center wound care quick reference guide.” This is a handy one-page reference guide that includes photographs and recommendations.
- “How-to guide: Prevent pressure ulcers—pediatric supplement.” This guide, tailored for pediatrics, describes key evidence-based care components for preventing pressure ulcers and describes how to implement these interventions.
You can also access case studies from a variety of facilities around the United States.
http://partnershipforpatients.cms.gov/p4p_resources/tsp-pressureulcers/
toolpressureulcers.html
Lymphedema resources
The National Lymphedema Network is a nonprofit organization founded in 1988 to provide education and other information to healthcare professionals and patients with lymphedema, as well as the general public. The site includes an explanation of lymphedema that may be helpful for you to use in teaching your patients. It also includes access to some of the articles from the newsletter LymphLink.
Diabetes clinical practice guidelines
Many patients with chronic wounds have diabetes. To ensure those patients receive the best possible care, you can refer to the 2013 Standards of Medical Care in Diabetes from the American Diabetes Association, which were published in the January issue of
Diabetes Care.
The journal provides a summary of the revisions and an executive summary of the standards related to each area, including diagnosis, testing, prevention, monitoring, and pharmacologic and nonpharmacologic management.
The guidelines include valuable information related to neuropathy screening and treatment and foot care. Recommendations for foot care include performing an annual comprehensive foot examination to identify risk factors predictive of ulcers and amputations. The foot examination should include inspection, assessment of foot pulses, and testing for loss of protective sensation.
http://care.diabetesjournals.org/content/36/Supplement_1
Read MoreFour key ingredients make up the recipe for effective team meetings
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN
Most of us have had days when we jump from meeting to meeting and at the end of the day wonder, “Did I get anything accomplished or am I more behind than ever?”
Many clinicians tell me that although their wound team meets regularly, the meetings aren’t meaningful enough, leaving the team still facing issues with their wound care program. As a consultant, when I review the wound team agenda, it’s typically missing one or more of four key ingredients:
- appropriate member representation
- proactive approach that highlights prevention
- review of the plan of care and update of the medical record
- review of supplies and products. Here’s a closer look at each of these ingredients.
Build a top team
Having the appropriate members on the wound care team is the first ingredient for success. A comprehensive, interdisciplinary team approach is the key to preventing skin breakdown and ensuring good clinical outcomes for residents with skin breakdown. Teams should include representation from nursing, dietary, and physical and occupational therapy, as well as a nurse practitioner or physician.
Nursing representation should include nurses from all three shifts and nursing assistants, who are too often missing from the team. Keep in mind that when it comes to preventing pressure ulcers, nursing assistants carry out most of interventions (for example, turning, incontinence management, heel lift). Even when a patient has a wound, the only intervention carried out by the nurses is the topical treatment; nursing assistants perform all other interventions necessary to ensure healing. Clinicians who empower nursing assistants to have a strong influence with the wound care team—and the program—tend to have very successful prevention programs and good clinical outcomes.
Think prevention
The second key ingredient is prevention. Most wound team meetings only discuss the patients with wounds, missing the bigger goal of preventing wounds in the first place. Once the patients with wounds are discussed, the team should review all high-risk patients to ensure proper preventative measures are in place and care planned. All patients should be quickly reviewed for evidence of:
- decline or change in mobility and activity
- new onset or change in continence status
- decline in nutritional status
- decline or change in cognition.
Any triggers in these areas should prompt a review of the plan of care to ensure they are being effectively addressed.
Review and update the plan
The third key ingredient for success is to use meeting time to review and update the plan of care. I’ve observed highly productive meetings and great discussions of the care the facility is providing. Then I review the medical record and discover that none of the interventions discussed are on the plan of care. Always review the patient’s plan of care to ensure it’s accurate, reflects all interventions, and is up to date. This will give you peace of mind that the medical record reflects all the good work you’re doing and helps make the team meetings feel productive.
Discuss products and supplies
The fourth key ingredient is to take the time to quickly discuss current wound care supplies and products with the team. Ask the team if the current supplies are user-friendly, are adequate, provide good outcomes, and are in good working condition.
Many times staff will not say how they’re struggling with, modifying, or not using something until they’re asked. Remember that the most expensive product is the one that doesn’t work or doesn’t get used.
A recipe for success
Using these four key ingredients will lead you to a successful wound team meeting—and a successful program. The mix may not solve your too-many-meetings days, but will give you peace of mind that at least one meeting is productive.
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has been specializing in wound prevention and management since 1990.
Read MoreUnna Boot
An Unna boot is a special dressing of inelastic gauze impregnated with zinc, glycerin, or calamine that becomes rigid when it dries. It is used for managing venous leg ulcers and lymphedema in patients who are ambulatory. When the patient walks, the rigid dressing restricts outward movement of the calf muscle, which directs the contraction force inward and improves the calf-muscle pumping action, thereby improving venous flow. An Unna boot does not provide compression and is contraindicated for arterial insufficiency.
(more…)
The “latest and greatest” vs. the basics
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
If you’re keeping up on wound care, you know a lot of new things are coming to market with enough decent science behind them to make them reasonable options to consider in your practice. And as true-blooded Americans and citizens of the post-industrialized world, we want what’s newest, fastest, and best in class in everything. It’s just our nature.
But does it truly serve us to be eager to try new therapies even when the current treatment plan is successful? Perhaps. We know we must never close our eyes to new developments in our field that can lead to better outcomes. Knowing when and what to change can lead to better outcomes for the patient, the wound, and our collective pocketbook.
I’ve long maintained we can achieve excellent-quality wound care if we just stick to the basics the vast majority of the time. Why? Systemic, psychosocial, and local factors all affect wound healing—not just the dressing or cream. Our job is to provide the optimum environment possible for wound healing. That requires us to look at and support the whole body toward optimum health, not solely the wound.
The basics begin with identifying the cause of the wound and implementing interventions to reduce, control, or eliminate the cause. Next, we strive to manage local and psychosocial factors by choosing topical products that will maintain moisture balance, keep the wound warm, and protect it. If the wound doesn’t show progress toward healing within 2 weeks (or as expected, given the patient’s overall condition and ability to heal), we need to reevaluate the plan and begin making changes.
The best rule is to make one change at a time. That makes it much easier to determine what’s working and what isn’t. Once all the basics are in place and required changes have been made, if healing is still stalled or nonexistent, consider trying the available new products and specialty products.
Never close your clinical mind to advances in the field. To do that would be a disservice to your patients. But you should change the treatment plan only when a change is needed—not just for the sake of changing it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief
Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Clinical Notes
Diabetes ‘ABC’ goals improve, but work remains
The number of people with diabetes who are meeting the ABC goals—hemoglobin A1C, blood pressure, and LDL cholesterol—has risen significantly in recent years, according to a study published by Diabetes Care. Patients meeting all three goals rose from about 2% in 1988 to about 19% in 2010.
Gains were made in each of the ABC goals, based on 2007 to 2010 data: 53% of patients met A1C goals, compared to 43% in 1988 to 1994 data; 51% met blood pressure goals, compared to 33%; and 56% met LDL goals, compared to 10%.
Younger people were less likely to meet A1C and cholesterol goals. Compared with non-
Hispanic whites, Mexican Americans were less likely to meet A1C and LDL goals and non-Hispanic blacks were less likely to meet blood pressure and LDL goals.
“The prevalence of meeting A1C, blood pressure, and LDL goals among people with diabetes, 1988–2010” also found that statin use significantly increased from about 4% in 1988 to 1994 to about 51% in 2007 to 2010.
The researchers analyzed data from the National Health and Nutrition Examination Surveys from 1988–1994, 1999–2002, 2003–2006, and 2007–2010. Nearly 5,000 people age 20 or older participated.
Although progress had been made, the researchers conclude, “Despite significant improvement during the past decade, achieving the ABC goals remains suboptimal among adults with diabetes, particularly in some minority groups.”
Daily bathing with chlorhexidine-impregnated washcloths reduces infection risk
A study in The New England Journal of Medicine reports that daily bathing with chlorhexidine-impregnated washcloths reduces the risk of becoming infected with multidrug-resistant organisms and subsequent development of hospital-acquired bloodstream infections in intensive care unit patients.
“Effect of daily chlorhexidine bathing on hospital-acquired infection” included 7,727 patients in nine intensive care and bone marrow units in six hospitals. The units were randomly assigned to bathe patients with either no-rinse 2% chlorhexidine-impregnated washcloths or nonantimicrobial washcloths for 6 months; then, the units switched to the opposite product for 6 months.
The rate of infection with multidrug-resistant organisms was 23% lower in the chlorhexidine group and the rate of hospital-acquired bloodstream infection was 28% lower in the chlorhexidine group.
Patients tend not to wear custom-made footwear for preventing diabetic foot ulcers
Adherence to wearing prescription custom-made footwear was low among patients with diabetes, neuropathy, and a recently healed plantar foot ulcer, according to a study in Diabetes Care. The low adherence was particularly notable at home, where patients did the most walking.
“Adherence to wearing prescription custom-made footwear in patients with diabetes at high risk for plantar foot ulceration” studied 107 patients by using a shoe-worn, temperature-based monitor. The researchers also measured daily step count by using an
ankle-worn activity monitor.
Factors associated with higher adherence included lower body mass index, more severe foot deformity, and more appealing footwear.
Tedizolid works as well as linezolid in patients with acute bacterial skin infections
A JAMA study says that a 200-mg once-daily dose of oral tedizolid phosphate over 6 days was as effective as 600 mg of oral linezolid every 12 hours for 10 days in patients with acute bacterial skin and skin-structure infections, including cellulitis or erysipelas, major cutaneous abscesses, and wound infections.
“Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: The ESTABLISH-1 Randomized Trial” reports a Phase 3, randomized, double-blind study conducted in 81 study centers with data analyzed from 667 adults.
A shorter course of tedizolid may be a “reasonable alternative” to linezolid for treating acute bacterial skin and skin-structure infections, the study concludes.
Water-based exercise improves ROM in patients with long-term arm lymphedema
A study of breast cancer survivors (median 10 years after surgery) with lymphedema found that a water-based exercise program improved shoulder range of motion (ROM).
Of the 29 eligible patients, 25 completed the study “Water-based exercise for patients with chronic arm lymphedema: A randomized controlled pilot trial,” published in the American Journal of Physical Medicine & Rehabilitation.
The program consisted of at least twice-weekly water-based exercise for 8 weeks. At first, participants were supervised, but later they exercised independently. Although lymphedema status didn’t change, those who performed water-based exercise had an increase in ROM, showing improvement years after surgery.
Dehydrated amniotic membrane allograft possible option for treating chronic wounds
A dehydrated amniotic membrane allograft (EpiFix) was used to treat four patients whose wounds hadn’t closed after conservative and advanced measures and who had been referred for plastic procedures. A variety of wounds healed (located on the elbow, knee, hand, and ankle) after one to three applications of the amniotic material, which patients tolerated well. The wounds remained closed several months later.
The authors of “Use of dehydrated human amniotic membrane allografts to promote healing in patients with refractory non healing wounds” recommend further investigation.
Mortality not linked to hospital readmissions in some patients
A study in JAMA reports that readmission rates aren’t linked to mortality rates in patients with an acute myocardial infarction or pneumonia and were only “weakly associated” for patients with heart failure.
“Relationship between hospital readmission and mortality rates for patients hospitalized with acute myocardial infarction, heart failure, or pneumonia” studied Medicare beneficiaries. The study is likely to fuel ongoing discussions as to the value of using readmission and mortality rates as factors for reimbursement.
Study casts doubt on MLD’s role in breast cancer–related lymphedema
A meta-analysis published in the World Journal of Surgical Oncology found the “current evidence” from randomized clinical trials “does not support” the use of manual lymphatic drainage (MLD) in preventing or treating lymphedema in patients with breast cancer.
However, the authors of “Effects of manual lymphatic drainage on breast cancer–related lymphedema: a systematic review and meta-analysis of randomized controlled trials” note that the overall methodology of the studies was poor.
The authors analyzed 10 randomized clinical trials with 566 patients.
CDC issues additional prevention steps for carbapenem-resistant Enterobacteriaceae
On Feb. 14, the Centers for Disease Control and Prevention (CDC) issued additional prevention steps for carbapenem-resistant Enterobacteriaceae (CRE). Increased reports of CRE prompted the action: Of the 37 unusual forms of CRE reported in the U.S., the last 15 have been reported since July 2012.
Facilities should follow the CDC guidance for preventing the spread of CRE in healthcare settings. The CDC also now recommends the following:
• When a CRE is identified in a patient with a history of an overnight stay in a healthcare facility (within the last 6 months) outside the U.S., send the isolate to a reference laboratory for confirmatory susceptibility testing and test to determine the carbapenem resistance mechanism.
• For patients admitted to healthcare facilities in the U.S. after recently being hospitalized (within the last 6 months) in countries outside the U.S., consider performing rectal screening cultures to detect CRE colonization, and place patients on contact precautions while awaiting the results.
Examples of Enterobacteriaceae include Klebsiella species and Escherichia coli. CRE are Enterobacteriaceae with high levels of resistance to antibiotics, including carbapenems. CRE infections most commonly occur among patients who are receiving antibiotics and significant medical treatment for other conditions.
Read MoreDebridement options: BEAMS made easy
By Cindy Broadus, RN, BSHA, LNHA, CHCRM, CLNC, CLNI, WCC, DWC, OMS
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
Read MorePositive Stemmer’s sign yields a definitive lymphedema diagnosis in 10 seconds or less

By Robyn Bjork, MPT, CWS, WCC, CLT-LANA
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)
Read MoreIn Hospitals, Daily Antiseptic Bath May Prevent Dangerous Infections
Clinician Resources
Clinical practice guidelines help ensure we are applying the latest knowledge and expertise when we’re caring for patients. Here are a few recent guidelines that you may find useful.
Measurement of ankle-brachial index
An American Heart Association scientific statement, “Measurement and interpretation of the ankle-brachial index (ABI),” published in Circulation, outlines the use of ABI, terminology, how to calculate the value, training, standards, and suggestions for future research.
Recommendations for obtaining an ABI measurement include:
• Use the Doppler method to determine the systolic blood pressure in each arm and each ankle.
• Use the appropriate cuff size, with a width of at least 40% of the limb circumference.
• Place the ankle cuff just above the malleoli with the straight wrapping method.
• Cover open lesions with the potential for contamination with an impermeable dressing.
• Avoid using a cuff over a distal bypass.
The article also recommends measurement and interpretation of ABI be part of the standard curriculum for nursing and medical students. For more information about ABI, read “Bedside ankle-brachial index testing: Time-saving tips” in this issue of Wound Care Advisor.
http://circ.ahajournals.org/content/126/24/2890
A social media approach to childhood obesity
Childhood obesity continues to be a significant problem in the United States, requiring innovative approaches for prevention and management. Those who are obese run the risk of poorer wound healing.
“Approaches to the prevention and management of childhood obesity: The role of social networks and the use of social media and related electronic technologies: A scientific statement from the American Heart Association,” published in Circulation, evaluates the role of social networks and social media in relation to childhood obesity and presents five steps for using social networks:
1 Define the goal of the intervention.
2 Identify the social network.
3 Develop and pilot test the intervention.
4 Implement the intervention.
5 Spread the intervention.
The guidelines conclude that social media holds promise as a tool, but more research is needed.
http://circ.ahajournals.org/content/early/2012/12/03/CIR.0b013e3182756d8e
Guidelines for managing patients with stable ischemic heart disease
Many patients with wound or ostomy needs have comorbid heart disease. Be sure you are aware of the most current information for managing these patients by accessing “2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease,” published in Circulation.
The guidelines acknowledge the vital importance of shared decision making between the healthcare provider and the patient. The information is divided into four sections with supporting algorithms:
• approaches to diagnosis
• risk assessment
• treatment
• follow-up.
Access the top 10 things to know and the executive summary.
http://circ.ahajournals.org/content/126/25/e354
Pressure ulcer guideline syntheses
The Agency for Healthcare Research and Quality (AHRQ) has made it easier to compare guidelines for managing pressure ulcers by publishing two guideline syntheses:
• Management of pressure ulcers
• Prevention of pressure ulcers
In each case, the synthesis includes information in the following categories:
• areas of agreement and difference
• comparison of recommendations
• strength of evidence and recommendation grading schemes
• methodology
• source(s) of funding
• benefits and harms
• abbreviations
• status.
Access these and other guideline syntheses from AHRQ.
Bonus resource: Ethical case study of a patient refusing skin ulcer treatment
View: Patient rights
Free, one-time registration is required to view the entire video and all other
content on the Medscape website.
Patients have a right to make their own decisions, but what happens when a decision is so painful for staff that it affects morale? Arthur Caplan, PhD, Division of Medical Ethics at the NYU Langone Medical Center in New York, discusses such a case: “Patients have the right to choose death from bedsores.”
Read MoreBedside ankle-brachial index testing: Time-saving tips
By Robyn Bjork, MPT, CWS, WCC, CLT-LANA
A hot flush of embarrassment creates a bead of sweat on my forehead. “I’ve got to get this measurement,” I plead to myself. One glance at the clock tells me this bedside ankle-brachial index (ABI) procedure has already taken more than 30 minutes. My stomach sinks as I realize I’ll have to abandon the test as inconclusive. (more…)
Read More