A hot flush of embarrassment creates a bead of sweat on my forehead. “I’ve got to get this measurement,” I plead to myself. One glance at the clock tells me this bedside ankle-brachial index (ABI) procedure has already taken more than 30 minutes. My stomach sinks as I realize I’ll have to abandon the test as inconclusive. (more…)
Guidelines for managing prosthetic joint infections released
The Infectious Diseases Society of America has released guidelines for diagnosing and managing prosthetic joint infections.
“Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America,” published in Clinical Infectious Diseases, notes that of the 1 million people each year who have their hips or knees replaced, as many as 20,000 will get an infection in the new joint.
The guidelines describe the best methods for diagnosing these infections, which are not easy to identify. Specifically, infection should be suspected in a patient who has any of the following: persistent wound drainage in the skin over the joint replacement, sudden onset of a painful prosthesis, or ongoing pain after the prosthesis has been implanted, especially if there had been no pain for several years or if there is a history of prior wound healing problems or infections.
Guidelines for treating infections are included and note that 4 to 6 weeks of I.V. or highly bioavailable oral antibiotic therapy is almost always necessary to treat prosthetic joint infections.
A decade of TIME
The TIME acronym (tissue, infection/inflammation, moisture balance, and edge of wound) was first developed more than 10 years ago to provide a framework for a structured approach to wound bed preparation and a basis for optimizing the management of open chronic wounds healing by secondary intention. To mark the event, the International Wound Journal has published “Extending the TIME concept: What have we learned in the past 10 years?”
The review points out four key developments:
• recognition of the importance of biofilms (and the need for a simple diagnostic)
• use of negative-pressure wound therapy
• evolution of topical antiseptic therapy as dressings and for wound lavage (notably, silver and polyhexamethylene biguanide)
• expanded insight into the role of molecular biological processes in chronic wounds (with emerging diagnostics).
The authors conclude, “The TIME principle remains relevant 10 years on, with continuing important developments that incorporate new evidence for wound care.”
Bed alarms fail to reduce patient falls
A study in Annals of Internal Medicine found that the use of bed alarms had no statistical or clinical effect on falls in an urban community hospital.
The 18-month trial included 16 nursing units and 27,672 inpatients. There was no difference in fall rates per 1,000 patient-days, the number of patients who fell, or the number of patients physically restrained on units using bed alarms, compared with control units.
Authors of “Effects of an intervention to increase bed alarm use to prevent falls in hospitalized patients: A cluster randomized trial” speculate the lack of response may be related to “alarm fatigue.”
Drug for HIV might help in Staph infections
A study in Nature reports that the drug maraviroc, used to treat HIV, might be useful for treating Staphylococcus aureus infections.
“CCR5 is a receptor for Staphylococcus aureus leukotoxin ED” found that the CCR5 receptor, which dots the surface of immune T cells, macrophages, and dendritic cells, is critical to the ability of certain strains of Staph to specifically target and kill cells with CCR5, which orchestrate an immune response against the bacteria. One of the toxins the bacterium releases, called LukED, latches on to CCR5 and subsequently punches holes through the membrane of immune cells, causing them to rapidly die.
When researchers treated cells with CCR5 with maraviroc and exposed the cells to the Staph toxin, they found maraviroc blocked toxic effects.
Dog able to sniff out C. difficile
A 2-year-old beagle trained to identify the smell of Clostridium difficile was 100% successful in identifying the bacteria in stool samples, and correctly identified 25 of 30 cases of patients with C. difficile, according to a study in BMJ.
“Using a dog’s superior olfactory sensitivity to identify Clostridium difficile in stools and patients: Proof of principle study” discusses how the dog was trained to detect C. difficile and concludes that although more research is needed, dogs have the potential for screening for C. difficile infection.
After-hours access to providers reduces ED use
Patients who have access to their primary healthcare providers after hours use emergency departments (EDs) less frequently, according to a study in Health Affairs.
“After-hours access to primary care practices linked with lower emergency department use and less unmet medical need” found that 30.4% of patients with after-hours access to their primary care providers reported ED use, compared with 37.7% of those without this access. In addition, those with after-hours access had lower rates of unmet needs (6.1% compared to 12.7%).
The findings come from the 2010 Health Tracking Household Survey of the Center for Studying Health System Change. The total sample included 9,577 respondents.
Neuropathic pain in patients with DPN might contribute to risk of falling
The presence of neuropathic pain in patients with diabetic peripheral neuropathy (DPN) contributes to gait variability, which could in turn contribute to the risk of falling, according to “Increased gait variability in diabetes mellitus patients with neuropathic pain.”
The study, published in the Journal of Diabetes and Its Complications, compared patients with at least moderate neuropathic pain with those who had no pain. Researchers used a portable device to measure gait parameters, such as step length and step velocity.
Amputation rates decrease significantly in patients with PAD
“Temporal trends and geographic variation of lower-extremity amputation in patients with peripheral artery disease (PAD): Results from U.S. Medicare 2000–2008” found that amputation rates have decreased significantly, but that significant patient and geographic variations remain.
The study, published in the Journal of the American College of Cardiology, found that among 2,730,742 older patients with identified PAD, the overall rate of lower extremity amputation decreased from 7,258 per 100,000 patients to 5,790 per 100,000. Predictors of lower-extremity amputation included male sex, black race, diabetes mellitus, and renal disease.
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT
Every year, 1.9% of patients with diabetes develop foot ulcers. Of those, 15% to 20% undergo an amputation within 5 years of ulcer onset. During their lifetimes, an estimated 25% of diabetic patients develop a foot ulcer. This article discusses use of hyperbaric oxygen therapy (HBOT) in treating diabetic foot ulcers, presenting several case studies.
HBOT involves intermittent administration of 100% oxygen inhaled at a pressure greater than sea level. It may be given in a:
• multi-place chamber (used to treat multiple patients at the same time), compressed to depth by air as the patient breathes 100% oxygen through a face mask or hood (more…)
Staphylococcus aureus is one of the most feared human pathogens, causing a wide range of infections. Most wound care professionals can expect to frequently encounter patients with S. aureus infections. Soft-tissue infections caused by S. aureus include impetigo, cellulitis, and cutaneous abscesses, as well as such life-threatening processes as necrotizing fasciitis and pyomyositis (a hematogenous intramuscular abscess). Serious non-soft-tissue infections include septic arthritis, osteomyelitis, pneumonia, endocarditis, and sepsis.
Why is S. aureus such a nasty bug?
S. aureus produces various cellular and extracellular factors involved in the pathogenesis of infection. S. aureus protein A, an important surface protein, helps the organism resist phagocytosis. Also, S. aureus produces several cytotoxins and enzymes that contribute to infection spread and severity. In addition, some strains produce toxins (including toxic shock syndrome toxin-1) that function as superantigens—molecules that nonspecifically trigger release of large amounts of cytokines, leading to a sepsislike condition. Taken together, such factors combine to make S. aureus a dangerous pathogen.
MRSA emergence
When penicillin was introduced in the 1940s, virtually all S. aureus isolates were sensitive to that drug. But soon thereafter, S. aureus strains that produced a β-lactamase enzyme capable of inactivating penicillin became widespread. During the 1950s, outbreaks of penicillin-resistant S. aureus occurred in many U.S. hospitals. Introduction of penicillinase-resistant antibiotics, such as methicillin and oxacillin, temporarily restored the ability to treat all strains of this pathogen using penicillin antibiotics. The first strain of methicillin-resistant S. aureus (MRSA) was described in 1961 shortly after introduction of penicillinase-resistant antibiotics.
The mechanism of methicillin resistance involves a mutation in one of the bacterial cell-wall proteins to which penicillins must bind to kill the bacterium. This mutation renders the organism resistant to all penicillins and penems and almost all cephalosporins.
MRSA incidence has increased steadily to the point where it currently constitutes up to 60% of S. aureus isolates in many U.S. hospitals. These organisms commonly carry genetic material that makes them resistant to various non-β lactam antibiotics as well, leading some to suggest that the term MRSA should stand for multiply resistant S. aureus. S. aureus has continued to mutate in the face of persistent antibiotic pressure. Vancomycin-intermediate S. aureus (VISA) was described in 1997; vancomycin-resistant S. aureus (VRSA), in 2003. Fortunately, these two strains remain rare and haven’t become established pathogens. (See Strains of antibiotic-resistantS. aureus by clicking the PDF icon above.)
Healthcare- versus community-acquired MRSA
Although MRSA initially arose and spread within healthcare settings (chiefly acute-care hospitals), a community-based variant was described in 1998. Called community-
acquired MRSA (CA-MRSA), this variant differs from healthcare-associated MRSA (HCA-MRSA) in more ways than the acquisition site. CA-MRSA occurs predominately in otherwise healthy children and young adults.
It most commonly presents as recurrent cutaneous abscesses, although life-threatening infections (such as necrotizing fasciitis and pneumonia) also have occurred. The propensity to cause cutaneous abscesses isn’t fully understood but may relate partly to production of the Panton-Valentine toxin by many CA-MRSA isolates.
In contrast, HCA-MRSA afflicts mainly older patients, particularly those with chronic illnesses, including chronic wounds. It typically causes wound infections, urinary tract infections, pneumonia, and bacteremia.
Besides these epidemiologic and clinical differences, many CA-MRSA isolates derive from a single clone, known as clone USA 300, whereas HCA-MRSA is composed of multiple non-USA 300 clones. Finally, many CA-MRSA isolates are sensitive to non-β
lactam antibiotics, whereas most HCA-MRSA isolates resist multiple antibiotics. More recently, the distinction between CA-MRSA and HCA-MRSA has been blurred as evidence emerges that CA-MRSA now is being transmitted in healthcare settings as well as in the community.
S. aureus carrier state
Staphylococci are frequent colonizers of humans. Common colonization sites include the skin, anterior nares, axillae, and inguinal regions. Individuals can be colonized continuously or transiently, with nasal carriage rates varying from 20% to 40%. Most S. aureus infections result from the strain carried by the infected patient.
Three patterns of S. aureus carriage exist in humans:
• 20% of individuals are continuously colonized.
• 30% of individuals are intermittently colonized.
• 50% of individuals are never colonized.
The highest carriage rates occur in patients receiving frequent injections (such as insulin-dependent diabetics, hemodialysis patients, and I.V. drug users) and those with chronic skin conditions (for instance, psoriasis or eczema). In the general population, MRSA carriage rates have increased to 1% or 2%, with clinical consequences hinging on the colonizing strain (CA-MRSA versus HCA-MRSA) and host characteristics. The most consistent carriage site is the anterior nares, but many other sites may carry this pathogen, including the axillae, inguinal regions, and perirectal area.
MRSA treatment
Therapy for MRSA infection depends on the infection location and antibiotic sensitivity of the infecting strain.
• Cutaneous abscesses are treated by incision and drainage; antibiotics play a secondary role to adequate drainage.
• Therapy for necrotizing fasciitis caused by MRSA involves aggressive debridement with removal of all necrotic tissue, plus adequate antibiotic therapy. Typically, patients require serial debridement followed by subsequent careful wound care, often with eventual skin grafting.
• Pyomyositis treatment entails drainage of the muscle abscess (which sometimes can be done with percutaneous tube placement instead of open drainage), plus appropriate antibiotic therapy.
Vancomycin has been the mainstay of I.V. therapy for MRSA for decades, but some clinicians are concerned that its effectiveness may be declining due to slowly increasing minimum inhibitory concentrations (the minimum concentration of an
antibiotic needed to inhibit pathogen growth). Other parenteral options have emerged in the last few years. (See I.V. drugs used to treat MRSA by clicking the PDF icon above.) Several oral antibiotics also are available for MRSA treatment. (See Oral agents used to treat MRSA by clicking the PDF icon above.)
Knowing the antibiotic sensitivity pattern of the infecting MRSA strain is crucial to ensuring that the patient receives an appropriate antibiotic. Treatment duration for soft-
tissue infections usually ranges from 7 to 14 days, but bacteremia and bone or joint infections call for more prolonged therapy.
Efforts to eradicate MRSA carriage
Because the carrier state increases the risk of subsequent S. aureus infection, efforts have been made to eradicate carriage. Unfortunately, this has proven to be difficult. A commonly used regimen involves 5 days of twice-daily mupirocin nasal ointment with either chlorhexidine gluconate showers or immersion up to the neck in a dilute bleach solution. However, success in eliminating carriage is limited, although the bleach bath seems to improve eradication rates better than other modalities.
Controlling MRSA in hospitals
How best to control MRSA spread within hospitals is controversial. Some experts advocate an aggressive, “search and destroy” approach involving screening all patients for nasal carriage on admission and initiating contact precautions with subsequent decolonization efforts. Others focus on improving the overall level of hand hygiene and other general infection-control measures, arguing that nasal screening misses at least 20% of MRSA-colonized patients and thus gives an unwarranted sense of security.
Many hospitals use a mixed approach, screening patients suspected to be at high risk for MRSA carriage (such as those admitted from extended-care facilities or to the intensive care unit), while simultaneously trying to improve hand hygiene and general infection-control measures. Recent data suggest MRSA colonization and infection rates have stopped increasing and are beginning to decline.
MRSA is one of the most problematic pathogens encountered on a regular basis, and among the most dangerous pathogens we face. While some MRSA infections are relatively mild, many are serious or life-threatening. Severe soft-tissue infections, such as necrotizing fasciitis and pyomyositis, require surgical debridement or drainage, appropriate antibiotic therapy, and assistance from a wound-care professional to achieve optimal outcomes. n
Selected references
Calfee DP. The epidemiology, treatment and prevention of transmission of methicillin-resistant Staphylococcus aureus. J Infus Nurs. 2011 Nov-Dec;34(6):359-64.
DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010 May 1;375(9725): 1557-68.
Ippolito G, Leone S, Lauria FN, et al. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010 Oct;14 Suppl 4:S7-11.
Landrum ML, Neumann C, Cook C, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010. JAMA. July 4;308:50-9.
Lee AS, Huttner B, Harbarth S. Control of methicillin-resistant Staphylococcus aureus. Infect Dis Clin North Am. 2011 Mar;25(1):155-79.
Moellering RC Jr. MRSA: the first half century. J Antimicrob Chemother. 2012 Jan;67(1):4-11.
Otter JA, French GL. Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection. J Hosp Infect. 2011 Nov:79(3):189-93.
Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant pneumococci, and vancomycin-resistant enterococci. Mayo Clin Proc. 2011 Dec;86(12):1230-43.
Simor AE. Staphylococcal decolonization: an effective strategy for prevention of infection? Lancet Infect Dis. 2011 Dec;11(12):952-62.
Joseph G. Garner is director of the infectious disease division and hospital epidemiologist at the Hospital of Central Connecticut and a professor of medicine at the University of Connecticut.
Before discharge, a new ostomy patient and caregiver have a lot to learn, including how to empty the pouch, establish a schedule for pouch changes, measure the stoma to ensure protection from effluent, and use accessory supplies appropriately.
New wound-swabbing technique detects more bacteria
The new Essen Rotary swabbing technique takes a few seconds longer to perform than traditional techniques, but improves bacterial count accuracy in patients with chronic leg ulcers, according to a study published by Wounds International.
“Evaluation of the Essen Rotary as a new technique for bacterial swabs: Results of a prospective controlled clinical investigation in 50 patients with chronic leg ulcers” reports that Essen Rotary detected significantly more bacteria compared to standard techniques and was the only one to identify five patients with methicillin-resistant Staphylococcus aureus (MRSA), compared to three detected by other techniques.
The Essen Rotary technique samples a larger surface area of the wound, which is beneficial for detecting MRSA.
“The Essen Rotary may become the new gold standard in routinely taken bacteriological swabs especially for MRSA screenings in patients with chronic leg ulcers,” the study authors write.
Reducing HbA1c by less than 1% cuts cardiovascular risk by 45% in patients with type 2 diabetes
A study presented at the American Diabetes Association 72nd Scientific Sessions found lowering HbA1c an average of 0.8% (from a mean of 7.8% to 7.0%, the treatment target) reduced the risk of cardiovascular death by 45% in patients with type
2 diabetes.
The absolute risk of mortality from a cardiovascular event was 9.9 events per 1,000 person-years in patients with decreasing HbA1c compared to 17.8 events in patients with stable or increasing HbA1c.
“HbA1c reduction and risk of cardiovascular diseases in type 2 diabetes: An observational study from the Swedish NDR” examined data from 18,035 patients in the Swedish National Diabetes Register.
CMS revises hospital, nursing home comparison websites
The Centers for Medicare & Medicaid Services (CMS) has enhanced two websites designed to help the public make informed choices about their health care. Hospital Compare and Nursing Home Compare now have better navigation and new comparison tools. The two sites include data on quality measures, such as frequency of hospital-acquired infections, and allow the user to compare hospitals on these measures.
Improvements include easy-to-use maps for locating hospitals, a new search function that enables the user to input the name of a hospital, and glossaries that are easier to understand. It’s now also possible to access the data on the sites through mobile applications.
CMS maintains the websites, which are helpful for anyone who wants to compare facilities, not just patients on Medicare or Medicaid.
For more information, read the article in Healthcare IT News.
IOM releases report on accelerating new drug and diagnostics development
The Institute of Medicine (IOM) released “Accelerating the development of new drugs and diagnostics: Maximizing the impact of the Cures Acceleration Network—Workshop Summary.” The report is a summary of a forum that brought together members of federal government agencies, the private sector, academia, and advocacy groups to explore options and opportunities in the implementation of Cures Acceleration Network (CAN). The newly developed CAN has the potential to stimulate widespread changes in the National Institutes of Health and drug development in general.
Focus on individualized care—not just reducing swelling—in lymphedema patients
As a result of two extensive literature reviews, a researcher at the University of Missouri found that emphasizing quality of life—not just reducing swelling—is important for patients with lymphedema. Many providers and insurance companies base treatment on the degree of edema, but the volume of fluid doesn’t always correspond with the patients’ discomfort. Instead, an individualized plan of care should be developed.
The researchers found that Complete Decongestive Therapy (CDT), a comprehensive approach for treating lymphedema that includes skin and nail care, exercise, manual lymphatic drainage, and compression, may be the best form of specialized lymphedema management. For more information about CDT, watch for the November/December issue of Wound Care Advisor.
Plague case in Oregon draws national attention
An article about a case of the plague in Oregon has appeared on Huffington Post. A welder contracted the disease as a result of unsuccessfully removing a mouse from a stray cat’s mouth. Part of his hands have, in the words of the article, “darkened to the color of charcoal.” Later tests confirmed the cat had the plague.
Plague cases are rare in the United States. According to the Centers for Disease Control and Prevention, an average of 7 human cases are reported each year, with a range of 1 to 17 cases. Antibiotics have significantly reduced morality. About half of cases occur in people ages 12 to 45.
Use of negative pressure wound therapy with skin grafts
“Optimal use of negative pressure wound therapy for skin grafts,” published by International Wound Journal, reviews expert opinion and scientific evidence related to the use of negative pressure wound therapy with reticulated open-cell foam for securing split-thickness skin grafts.
The article covers wound preparation, treatment criteria and goals, economic value, and case studies. The authors conclude that the therapy has many benefits, but note that future studies are needed “to better measure the expanding treatment goals associated with graft care, including increased patient satisfaction, increased patience compliance and improved clinical outcomes.”
Mechanism for halting healing of venous ulcers identified
Researchers have identified that aberrantly expressed microRNAs inhibit healing of chronic venous ulcers, according to a study in The Journal of Biological Chemistry.
Six microRNAs were plentiful in 10 patients with chronic venous ulcers. The microRNAs target genes important in healing the ulcers. In an article about the study, one of the researchers said, “The more we know about the molecular mechanisms that contribute to [the development of venous ulcers], the more we can rationally develop both diagnostic tools and new therapies.”
Hemodialysis-related foot ulcers not limited to patients with diabetes
Both patients with diabetes and those without are at risk for hemodialysis-related foot ulcers, according to a study published by International Wound Journal.
Researchers assessed 57 patients for ulcer risk factors (peripheral neuropathy, peripheral arterial disease, and foot pathology, such as claw toes, hallux valgus, prominent metatarsal heads, corns, callosities, and nail pathologies) at baseline, and noted mortality 3 years later.
In all, 79% of patients had foot pathology at baseline, and 18% of patients without diabetes had peripheral neuropathy. Peripheral arterial disease was present in 45% of diabetic and 30% of nondiabetic patients. Nearly half (49%) of patients had two or more risk factors. Only 12% of patients had no risk factors. The presence of peripheral arterial disease and peripheral neuropathy increased risk of mortality.
The authors of “Prevalence of risk factors for foot ulceration in a general haemodialysis population” state that the high prevalence of risk factors in nondiabetic patients indicates that they are at risk for developing foot ulcers.
Study identifies risk factors for mortality from MRSA bacteremia
A study in Emerging Infectious Diseases found that older age, living in a nursing home, severe bacteremia, and organ impairment increase the risk of death from methicillin-resistant Staphylococcus aureus (MRSA) bacteremia.
Consultation with a specialist in infectious disease lowers the risk of death, and MRSA strain types weren’t associated with mortality.
“Predicting risk for death from MRSA bacteremia” studied 699 incidents of blood infection from 603 patients who had MRSA bacteremia.
Lymphedema is characterized by regional immune dysfunction, distorted limb contours, and such skin changes as papillomas, hyperkeratosis, and increased girth. The condition may involve the limbs, face, neck, trunk, and external genitals; its effects may include psychological distress. For optimal patient management, clinicians must understand what causes lymphedema and how it’s diagnosed and treated.
This two-part series provides an overview of lymphedema. Part 1 covers etiology, pathology, and diagnosis. Part 2, which will appear in the November-
December issue, will focus on treatment.
Causes of lymphedema
Lymphedema occurs when protein-rich fluid accumulates in the interstitium due to impaired lymphatic function. Proteins, other macromolecular wastes, and water constitute lymphatic loads. These wastes rely on specially structured absorptive and transport structures in peripheral regions for their return to central circulation.
When lymph stasis prevails, inflammatory processes and lymphostatic fibrosis trigger tissue-density changes, further entrapping superficial vessels and accelerating mechanical insufficiency. (See Physiologic changes caused by lymphatic disruption by clicking the PDF icon above.)
Classifying lymphedema
Lymphedema can be primary or secondary. Primary lymphedema either is congenital (present at birth) or arises around puberty. In the vast majority of cases, it is associated with structural changes in the lymphatic system and isn’t associated with another disease or condition. Most structural changes (87%) manifest before age 35 and cause hypoplasia of vessels and nodes. Syndromes involving hyperplasia, node fibrosis, or aplasia also may occur, although they’re much less common. Dysplasia (either hypoplasia, hyperplasia, or aplasia) predisposes drainage regions to inadequate lymph collection, resulting in edema and secondary tissue changes, such as chronic inflammation and reactive fibrosis. Genetic variability in lymphatic constitution may explain why seemingly similar patients receiving the same surgical protocol have different lymphedema risks over time. Secondary lymphedema stems from a significant insult to lymphatic tissues, as from lymphadenectomy, radiation therapy, trauma, infection, or cancer. It commonly results from direct trauma to regional nodes or vessel structures. Slow degradation of lymphatic function also occurs when adjacent tissues (such as superficial and deep veins) become diseased, when cellulitis occurs, or when accumulations
of adipose or radiation fibrosis mechanical-ly disrupt drainage of skin lymphatics.
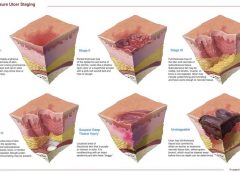
Lymphedema stages
Lymphedema progresses in stages, which involve secondary connective-tissue disease combined with disturbed fluid update and transport. These conditions cause a universal and classic clinical picture.
• Stage 0 (latency stage) is marked by reduced transport capacity and functional reserve. The patient has no visible or palpable edema, but has such subjective complaints as heaviness, tightness, and waterlogged sensations.
• In Stage 1 edema (reversible lymphedema), edema decreases with elevation. Pitting edema is present, but fibrosis is absent.
• During Stage 2 (spontaneously irreversible lymphedema), lymphedema doesn’t resolve entirely, although it may fluctuate. Pitting is more pronounced and fibrosis is present.
• Stage 3 (lymphostatic elephantiasis) is marked by dermal hardening, nonpitting edema, papillomas, hyperkeratosis, and in some cases, extreme girth.
Assessment and diagnosis
Diagnosing lymphedema can be challenging because edema may be associated with other diseases and disorders. For a summary of signs and symptoms, see Clinical findings in lymphedema by clicking the PDF icon above.
Discomfort and skin appearance
Lymphedema rarely causes pain because the skin accommodates gradual, insidious fluid accumulation. However, secondary orthopedic discomfort may result from increased weight of the affected limb due to deconditioning or decreased range of motion.
Because lymphedema usually progresses slowly, gravity and centrifugal forces pull fluids toward distal limb areas, causing an entrenched, stubborn pitting edema. Later, further valvular incompetence contributes to worsening distal edema in the fingers, toes, and dorsal regions of the hand and foot. Prominent lower-extremity structures, such as the malleolus, patella, tibia, anterior tibialis tendon, and Achilles tendon, become progressively less distinct. This creates a columnar limb appearance; the swollen limb has the same girth from distal to proximal aspects, unlike the natural cone shape of a normal limb.
Lymphatic failure doesn’t tax the venous system, so skin color remains normal. Blood supply remains patent, helping to prevent secondary ulcers.
Severity
Lymphedema severity correlates directly with such factors as onset of the condition and extent of cancer therapy, if given (number of nodes resected, number of positive nodes, and use of radiotherapy). Lymphedema may worsen with a greater number of infection episodes, weight gain, injury, diuretics, limb disuse, pneumatic compression therapy (when used for pure lymphedema), and ill-fitting compression garments. The single most important contributor to increasing lymphedema severity is lack of patient education, which can result in improper treatment or none at all.
Opportunistic infections
Lymphedema causes regional immune suppression and leads to an increase in opportunistic infections such as cellulitis. As skin integrity suffers, scaling and dryness allow resident skin pathogens (such as streptococci and staphylococci) to gain access through the defective skin barrier into protein-rich interstitial fluid, creating a medium favorable to bacterial colonization. Lymphocyte migration decreases, and dissected or irradiated nodal sites are slow to detect invaders. Furthermore, stagnant lymph promotes further delays in the immune response. Patients with opportunistic infections may exhibit high fever, local erythema, regional hypersensitivity or acute pain, flulike symptoms, and rapidly advancing “map-like” borders in the skin.
Differential diagnosis
Several methods can aid differential diagnosis. Clinical findings. Lymphedema can be diagnosed from patient history, physical examination, palpation, and inspection. Trauma to lymph nodes (each of which governs a distinct body region) decreases the transport capacity of lymph formed in that region, in turn causing local swelling (lymphedema). Trauma to the axillary or inguinal lymph nodes, which exist on both the left and right of the body and in both the upper and lower regions, predisposes these quadrants to swelling. Therefore, if lymph nodes on only one side are damaged, lymphedema occurs only on that side of the body. Using the universal characteristics cited above as a guide, while ruling out cancer recurrence, acute deep vein thrombosis, or plasma protein abnormalities, yields sufficient data to form a diagnosis. Imaging. Lymphography involves subcutaneous injection of a lymph vessel–
specific dye (Patent Blue V), followed by X-ray. Although it provides high-resolution images of lymphatic structures, this technique is invasive, painful, damaging to lymphatics, and potentially lethal—and therefore is no longer recommended.
Lymphangioscintigraphy (LAS) uses interdigital subcutaneous injection of protein-labeled radioisotopes, followed by
imaging at specific intervals to gather information about uptake and transport time. Images are hazy and false-negatives are common, so well-trained radiotherapists familiar with lymphology and lymphedema should administer and interpret the test. Also, experts don’t agree on standard criteria for LAS administration, so measures may not be similarly conclusive. Limb-measuring instruments and methods. Serial measurement of affected limb circumference using a standard garment tape measure is the most widely accessible approach. Intra-rater reliability is comparable to that of currently used tools; however, these methods can’t be used for early detection, for screening, or when various raters are used to assess the same patient. Circumferences are measured at four points and are considered positive if a distance of 2 cm or more separates the involved from uninvolved extremity in comparison. Water displacement techniques for limb-volume calculation, although accurate, are impractical in most clinical settings and rarely used.
Various devices have been used to obtain measurements. For instance, the Perometer® uses optoelectronic volumetry. By scanning the limb with infrared beams circumferentially, the device accurately records girth at 4-mm intervals along the limb length and transmits these measurements to a computer. The Perometer is used mainly in the research setting. Preoperative and postoperative measurements at intervals can detect lymphedema early.
Impedimed XCA® uses bioelectrical
impedance to calculate ratios of intracellular to extracellular fluid. A weak electrical current is passed through affected and unaffected limbs, allowing comparison of results. Impedance is lower in edematous tissue, supporting an accurate diagnosis.
Next step: Treatment
Once a diagnosis is made, the next step is treatment. Part 2 of this series covers lymphedema treatment.
Selected references
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
Kubik S, Manestar M. Anatomy of the lymph capillaries and precollectors of the skin. In: Bollinger A, Partsch H, Wolfe JHN, eds. The Initial Lymphatics. Stuttgart: Thieme-Verlag; 1985:66-74.
Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)—2009. Int Angiol. 2010 Oct;29(5):454-70.
Lerner R. Chronic lymphedema. In: Prasad H, Olsen ER, Sumpio BE, Chang JB, eds. Textbook of Angiology. Springer; 2000.
Mayrovitz HN. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology. 2009 June;42(2):88-98
Pecking AP, Alberini JL, Wartski M, et al. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008 Mar;41(1):1-10.
Stanton AW, Northfield JW, Holroyd, B, et al. Validation of an optoelectronic volumeter (Perometer). Lymphology. 1997 June;30(2):77-97
Weissleder H, Schuchhardt C. Lymphedema: Diagnosis and Therapy. 4th ed. Viavital Verlag GmbH; 2007.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
In the current healthcare environment, wound care practitioners need to capitalize on all available reimbursement avenues for care delivery and wound care supplies and dressings. And when it comes to reimbursement, there’s one constant: The rules change constantly. Whether these changes always benefit the patient is questionable. Nowhere is this more evident than in acute-care settings. Clinicians constantly are challenged to make sure their patient-care decisions comply with current Medicare reimbursement guidelines. (And if you’re not sure about today’s guidelines, be prepared for the guidelines to change tomorrow.) (more…)
Complex wound failures are costly and time-consuming. They increase length of stay and contribute to morbidity and mortality in surgical patients. Negative-pressure wound therapy (NPWT)—a common adjunct to wound-care therapy—is used to accelerate wound healing in all fields of surgery. Using a vacuum device and wound-packing material, it applies subatmospheric pressure to complex wounds.
But NPWT alone doesn’t ensure adequate wound healing. Many physiologic factors—including infection, excessive moisture, nutrition, and medications—influence wound-healing success. Failure to account for these factors or improper application of NPWT can limit patient outcomes and cause debilitating complications.
For clinicians, applying and establishing an airtight seal on a complex wound is among the most dreaded, time-consuming, and challenging NPWT-related tasks. Simply applying NPWT material under layers of transparent drape may delay wound healing or exacerbate the wound. This article provides tips on safe application of NPWT to enhance the outcomes of patients with complex wounds.
Consider wound location
Wounds on the body’s anterior surfaces are less susceptible to the forces of pressure, friction, and shear than those on posterior and lateral surfaces. Posterior and lateral wounds commonly require posterior offloading or repositioning the patient in bed to reduce or eliminate direct pressure. This can be done with judicious and frequent patient turning using a specialty bed or support surface.
Bridge a posterior or lateral wound to an anterior surface by placing the drainage collection tubing to a nonpressure-bearing surface away from the wound. Bridging keeps the tubing from exerting pressure on intact skin and decreases the risk of a pressure ulcer. To create the bridge, cut foam into a single spiral of 0.5 to 1 cm, or if using gauze, fold gauze into 8 single layers.
Place the spiraled foam or gauze layers onto the drape, ensure the bridge is wider than the collection tubing disc, and secure it with an additional drape. Next, apply the NPWT collection tubing on the end of the bridge away from the wound. A wide bridge under the collection tubing disc will minimize the potential for periwound breakdown when negative pressure is initiated. You may modify this spiraling technique by varying the width of the foam to fill undermining and wounds of irregular configuration and depth.
Protect the periwound
An intact periwound may break down from exposure to moisture, injury from repetitive removal of a transparent drape, or NPWT material coming in contact with skin. Skin protection is critical in preventing additional breakdown stemming from contact with potentially damaging material.
Transparent drapes are designed to permit transmission of moisture vapor and oxygen. Avoid using multiple layers of transparent drapes to secure dressings over intact skin, as this can decrease the transmission of moisture vapor and oxygen, which in turn may increase the risk of fungal infection, maceration, and loss of an intact seal.
Periwound maceration also may indicate increased wound exudate, requiring an increase in negative pressure. Conversely, an ecchymotic periwound may indicate excessively high negative pressures. If either occurs, assess the need to adjust negative pressure and intervene accordingly. Reassess NPWT effectiveness with subsequent dressing changes.
Apply a protective liquid skin barrier to the periwound and adjacent healthy tissue to help protect the skin surface from body fluids. The skin barrier also helps prevent stripping of fragile skin by minimizing shear forces from repetitive or forceful removal of transparent drapes. Excessive moisture can be absorbed by using a light dusting of ostomy powder sealed with a skin barrier. A “window pane” of transparent drape or hydrocolloid dressing around the wound also can protect surface tissue from contactwith NPWT material and prevent maceration.
Avoid creating rolled wound edges
In the best-case scenario, epithelial tissue at the wound edge is attached to the wound bed and migrates across healthy granulation tissue, causing the wound to contract and finally close. With deep wound environments that lack moisture or healthy granulation tissue, the wound edges may roll downward and epibole may develop. Epibole is premature closure of the wound edges, which prevents epithelialization and wound closure when it comes in contact with a deeper wound bed. (See Picturing epibole by clicking the PDF icon above.)
Materials used in NPWT are primarily air-filled. Applying negative pressure causes air removal, leading to wound contraction by pulling on the wound edges—an action called macrostrain. Without sufficient NPWT material in the wound, macrostrain can cause the wound to contract downward and the wound edges to roll.
Ensure that enough NPWT material has been applied into the wound to enhance wound-edge approximation and avoid creating a potential defect as the wound heals. Before NPWT begins, material should be raised 1 to 2 cm above the intact skin. Additional material may be needed with subsequent changes if the NPWT material compresses below the periwound. The amount of NPWT material needed to remain above the periwound once NPWT starts varies with the amount of material compressed and the wound depth.
Reduce the infection risk
To some degree, all wounds are contaminated. Usually, the body’s immunologic response is able to clear bacterial organisms and wound healing isn’t delayed. But a patient who has an infection of a complex wound needs additional support.
Systemic antibiotics alone aren’t enough because they’re selective for specific organisms and don’t reach therapeutic levels in the wound bed. In contrast, topical antimicrobial adjuncts, such as controlled-release ionic silver, provide broad-spectrum antimicrobial coverage against fungi, viruses, yeasts, and gram-negative and gram-positive bacteria, including methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci.
Consider using controlled-release ionic silver for a wound known to be infected or at risk for infection due to its location or potential urine or fecal contamination. To be bactericidal, ionic silver must be in concentrations of at least 20 parts per million; also, it must be kept moist and must come in direct contact with infected wound bed. At lower concentrations, organisms may develop resistance. Ionic silver has no known resistance or contraindications. Dressings using it come in several forms, including a hydrogel sheet, perforated sheet, cavity version, and semiliquid hydrogel. Be sure the form you choose doesn’t occlude the NPWT material and compromise therapy. (See NPWT for a patient with necrotizing fasciitis by clicking the PDF icon above.)
One of the most daunting aspects of NPWT is obtaining and maintaining a good seal—in other words, avoiding the dreaded leak. Preventive skin measures may contribute to a poor seal; skin-care products containing glycerin, surfactant, or dimethicone may prevent adequate adhesion of NPWT drapes. Body oil, sweat, and hair may need to be minimized or removed.
To avoid leaks, don’t overlook the obvious—loose connections, a loose drainage collection canister, exposed NPWT material, and skinfolds extending beyond the transparent drape. Tincture of benzoin (with or without a thin hydrocolloid dressing) increases tackiness to enhance the adhesive property of a transparent drape on the diaphoretic patient and on hard-to-drape areas, such as the perineum. But be sure to use tincture of benzoin with discretion, as it may remove fragile periwound tissue when the dressing is removed.
Ostomy paste products can serve as effective filler. These pliable products can be spread into position to obtain a secure seal under the transparent drape in hard-to-seal areas, such as the perineum. Pastes remain flexible and can be removed without residue. Temporarily increasing NPWT pressure to a higher setting may help locate a subtle leak or provide enough negative pressure to self-seal the leak. Once the leak resolves, remember to return the pressure to the ordered setting.
Knowledge optimizes healing
It’s important to be aware of potential complications of NPWT (See Take care with NPWT by clicking on the PDF icon above). However, when applied correctly, NPWT is an effective option for managing complex wounds. Recognizing and managing potential complications at the wound site, ensuring periwound protection, minimizing epibole formation, and preventing wound infection can result in a better-prepared wound bed and promote optimal healing.
Selected references
Baranoski S, Ayello EA. (2012). Wound Care Essentials: Practice Principles. 3rd ed. Springhouse, PA; Lippincott Williams & Wilkins.
Bovill E, Banwell PE, Teot L, et al. Topical negative pressure wound therapy: a review of its role and guidelines for its use in the management of acute wounds. Int Wound J. 2008;5:511-529.
Sussman C, Bates-Jensen B. Wound Care: A Collaborative Practice Manual for Health Professionals. 4th ed. Baltimore, MD; Lippincott Williams & Wilkins; 2011.
Ronald Rock is an Adult Health Clinical Nurse Specialist in the Digestive Disease Institute at the Cleveland Clinic in Cleveland, Ohio.
Venous leg ulcers are the most common cause of lower extremity ulcers, affecting 1% of the U.S. population (approximately 3 million people). Annual treatment costs for venous disease in this country range from $1.9 to $3.5 billion.
The gold standard for venous ulcer treatment includes moist wound healing and compression therapy. But before compression wraps are applied, we must determine if adequate arterial blood flow exists—or consequences could be life-threatening.
Raise your hand if you know what ABI is. Now raise your hand if you routinely obtain ABIs for patients. I’ve been asking these questions at wound care seminars around the country for the last 10 years, and the answers are always the same:
Between 50% and 95% of the audience know what an ABI is, but only 1% to 2% say they perform the ABI test. My next question is “Why not?”
The ABI (ankle brachial index) is a noninvasive screening test performed with a handheld vascular Doppler and a blood pressure cuff. This simple test helps determine if you can safely apply compression therapy, aids diagnosis of peripheral arterial disease, and even helps monitor the efficacy of therapeutic interventions.
Numerous standard practice guidelines from various organizations recommend obtaining ABIs to determine arterial blood flow. These organizations include the American College of Cardiology, American Heart Association, American Diabetes Association, Society for Vascular Nursing, Wound Ostomy Continence Nurses, Society for Vascular Medicine, U.S. Preventive Services Task Force, and World Union of Wound Healing Societies.
Instructions for most compression therapy products include indications for Doppler ABI readings above 0.8. So if you don’t get an ABI reading, how can you safely apply these products? A report by Allie and colleagues found that more than 50% of lower extremity amputations occur without previous vascular testing of any type, including ABI.
So why aren’t more practitioners obtaining ABIs? The leading answer: “We don’t have a Doppler.” I understand the dilemma of not having equipment or the funds to get the equipment. But do we want to tell a patient who has just lost her leg, “Oh, sorry. We didn’t have a Doppler”?
It’s our responsibility and duty as WCCs, wound care experts, and health care clinicians to ensure we provide the highest standard of care for patients with venous leg ulcers. So communicate with management, explaining what you need and why you need it. Work with your medical supply company for an extended payment plan. Hold a fundraiser. Consider using the alternative Lanarkshire Oximetry Index procedure. Or send the patient to a wound clinic or other healthcare provider who can perform the test.
It’s time to step it up and take greater accountability—and to no longer use the excuse “We don’t have a Doppler.”
Donna Sardina, RN, MHA, WCC, CWCMS, DWC Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Selected references
Allie DE, Hebert CJ, Lirtzman MD, et al. Critical limb ischemia: a global epidemic. A critical analysis of current treatment unmasks the clinical and economic costs of CLI. EuroIntervention. 2005; 1(1):75-84. http://www.ncbi.nlm.nih.gov/pubmed/
19758881. Accessed June 4, 2012.
Lazarus GS, Cooper DM, Knighton DR, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch Dermatol. 1994; 130(4):489-493. http://www.ncbi.nlm.nih.gov/pubmed/8166487. Accessed June 4, 2012.
Olin JW, Allie DE, Belkin M, et al. ACCF/AHA/ACR/SCAI/SIR/SVM/SVN/SVS 2010 performance measures for adults with peripheral artery disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures, the American College of Radiology, the Society for Cardiac Angiography and Interventions, the Society for Interventional Radiology, the Society for Vascular Medicine, the Society for Vascular Nursing, and the Society for Vascular Surgery (Writing Committee to Develop Performance Measures for Peripheral Artery Disease). J Am Coll Cardiol. 2010;56(25):2147-2181. http://content.onlinejacc
.org/cgi/content/full/j.jacc.2010.08.606. Accessed June 4, 2012.
O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev. 2010;(1):CD003557. http://www.ncbi.nlm.nih.gov/pubmed/20091548. Accessed June 4, 2012.
Rooke TW, Hirsch AT, Misra S, et al; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society for Vascular Medicine; Society for Vascular Surgery. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58(19):2020-2045. http://
content.onlinejacc.org/cgi/content/full/j.jacc.2011.08.023v1. Accessed June 4, 2012.
Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insufficiency and venous leg ulceration. J Am Acad Dermatol. 2001;44(3):401-421. http://www.ncbi.nlm.nih.gov/pubmed/11209109. Accessed June 4, 2012.
World Union of Wound Healing Societies. Principles of best practice:. Compression in venous leg ulcers: a consensus document. London: MEP Ltd; 2008. www.woundsinternational.com/pdf/content_25.pdf. Accessed June 4, 2012.
The guideline updates IDSA’s 2004 diabetic foot infections guideline. It focuses on appropriate therapy, including debridement of dead tissue, appropriate antibiotic therapy, removing pressure on the wound, and assessing (and potentially improving) blood flow to the foot. The guideline also provides suggestions regarding when and how long antibiotics should be administered for soft-tissue and bone infections.
When diagnosing a diabetic patient with foot infection, the guideline recommends clinicians evaluate the patient at three levels—the patient as a whole, the affected foot or limb, and the infected wound. The guideline also provides advice on when and how to culture diabetic foot wounds.
Access a podcast on the guideline, which is available in a smartphone format and as a pocket-size quick-reference edition.
Combining bariatric surgery with medical therapy improves glycemic control
In obese patients with uncontrolled type 2 diabetes, bariatric surgery and 12 months of medical therapy significantly improved glycemic control compared to those who received only medical therapy, according to a study in The New England Journal of Medicine. “Bariatric surgery versus intensive medical therapy in obese patients with diabetes” was a randomized, nonblinded, single-center trial that included 150 patients in three groups: medical therapy only, medical therapy and Roux-en-Y gastric bypass, and medical therapy and sleeve gastrectomy.
Although glycemic control improved for all three groups, those who received bariatric surgery had better control. Use of drugs to lower glucose, lipid, and blood-pressure levels decreased significantly after both surgical procedures but increased in patients receiving medical therapy only. No deaths or life-threatening complications occurred.
HHS launches web-based tool for tracking healthcare performance
The U.S. Department of Health and Human Services (HHS) has launched a web-based tool for monitoring the performance of the healthcare system. The Health System Measurement Project gives providers and the public the ability to examine datasets from across the federal government that span specific topic areas, such as access to care, vulnerable populations, prevention, and quality. Users can also view indicators by population characteristics, such as age, sex, income level, insurance coverage, and geography.
PEG tubes may increase risk of new pressure ulcers
According to a study published in Archives of Internal Medicine, percutaneous endoscopic gastrostomy (PEG) tubes may increase the risk of pressure ulcers in nursing home patients with advanced cognitive impairment.
Researchers found that hospitalized patients who receive a PEG tube were 2.27 times more likely to develop a new pressure ulcer and those with a pressure ulcer were less likely to have it heal when they had a PEG tube. “Our findings regarding the risk of developing new stage 2 or higher pressure ulcers suggest that PEG feeding tubes are not beneficial, but in fact they may potentially harm patients,” conclude the researchers in “Feeding tubes and the prevention or healing of pressure ulcers.”
AHRQ provides QI toolkit for hospitals
The Agency for Healthcare Research and Quality (AHRQ) offers a toolkit designed to help hospitals understand AHRQ’s quality indicators (QIs). “AHRQ Quality Indicators™ Toolkit for Hospitals” includes steps for improvement, how to sustain change, and different tools for different audiences. Clinicians can also access audio interviews that provide information on how to use the tools and engage stakeholders and staff in QI efforts, and a recording of a webinar on the toolkit.
Silk fibers may be future resource for bone and tissue repair
Researchers at Tufts University have developed the first all-polymeric bone scaffold material that is fully biodegradable and capable of providing significant mechanical support during repair. The material could improve the way bones and tissues are repaired after an accident or following disease effects.
The new technology uses micron-size silk fibers to reinforce a silk matrix, much as steel rebar reinforces concrete. The study, “High-strength silk protein scaffolds for bone repair,” published in Proceedings of the National Academy of Sciences, found that the scaffold material is significantly less strong than normal bone, but it may play a role as a temporary biodegradable support for the patient’s cells to grow.
International guidelines for silver dressings in wounds released
A meeting of an international group of experts, convened by Wounds International, met in December 2011 to compile the consensus guidelines, which describe the patients who are most likely to benefit from silver dressings and how to use the dressings appropriately.
The guidelines recommend that silver dressings be used “in the context of accepted standard wound care for infected wounds or wounds that are at high risk of infection or reinfection.” Another recommendation is to use silver dressings for 2 weeks, then evaluate the wound, patient, and management approach before deciding whether to continue using the dressing or if a more aggressive intervention such as antibiotics would be better.
Cell therapy may benefit patients with lower extremity CLI
Injections of ixmyelocel-T in patients with lower extremity critical limb ischemia (CLI) who aren’t candidates for revascularization can prolong the time until treatment failure, according to a study in Molecular Therapy. Time to treatment failure was defined as major amputation, all-cause mortality, doubling of total wound surface area from baseline, or de novo gangrene. The double-blind, placebo-controlled RESTORE-CLI trial found that the adverse event rates were similar in the two groups.
New skin patch destroys skin cancer cells
A new skin patch destroyed facial basal cell carcinoma cells in 80% of patients, according to a study reported at the Society of Nuclear Medicine’s 2012 Annual Meeting.
Each of the 10 patients with facial basal cell carcinoma received a custom-made and fully sealed phosphorus-32 skin patch, a radiation spot-treatment in the form of a patch. Each patient was treated for 3 hours on the first day; the patches were reapplied on the fourth and seventh days after the first treatment for another 3 hours each. Three years after treatment, 8 of 10 patients were cancer-free.
The patients had lesions near the eyes, the nose, and forehead—areas more difficult to operate on, especially if skin grafting is needed later.
Small study links lymphedema to obesity
The average body-mass index (BMI) in obese patients with lymphedema was significantly greater than BMIs of obese patients without lymphedema, according to correspondence in The New England Journal of Medicine. The authors conclude, “Our findings suggest that obesity…may be a cause of lower-extremity lymphedema.”
“Lower-Extremity Lymphedema and Elevated Body-Mass Index” included 15 obese patients with bilateral lower-extremity enlargement who were referred to the authors’ center. Of the 15, five were diagnosed with lymphedema by lymphoscintigraphy.