Chronic venous leg ulcers (CVLUs) affect nearly 2.2 million Americans annually, including an estimated 3.6% of people over the age of 65. Given that CVLU risk increases with age, the global incidence is predicted to escalate dramatically because of the growing population of older adults. Annual CVLU treatment-related costs to the U.S. healthcare system alone are upwards of $3.5 billion, which are directly related to long healing times and recurrence rates of over 50%.
CVLUs are not only challenging and costly to treat, but the associated morbidity significantly reduces quality of life. That makes it critical for clinicians to choose evidence-based treatment strategies to achieve maximum healing outcomes and minimize recurrence rates of these common debilitating conditions. These strategies, which include compression therapy, specialized dressings, topical and oral medications, and surgery, are used to reduce edema, facilitate healing, and avert recurrence. (more…)
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make.
Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled procedures and herbal treatments to heal wounds, including xenografts (skin from another species). The practice of applying allografts (human cadaver skin) to wounds was first documented in 1503. In 1871, autologous skin grafting (skin harvested from the the person with the wound) was tried. Next came epithelial- cell seeding, which involves scraping off the superficial epithelium of healthy skin and transplanting the cells onto the wound. (more…)
It’s been a stressful day at work—nothing new. One confused patient pulled off her ostomy bag, you’re having difficulties applying negative-pressure wound therapy on another, and a third patient’s family is angry with you. We all experience stressful days, but unfortunately, sometimes we take our stress out on each other. Too often, this ineffective way of identifying and managing stress leads nurses to engage in lateral violence.
Inappropriate footwear is the most common source of trauma in patients with diabetes. Frequent and proper assessment of appropriate footwear is essential for protecting the diabetic foot from ulceration. Here is a step-by-step process for evaluating footwear. Be sure to evaluate footwear with the patient walking, standing, and sitting.
Have you ever ridden a bicycle with a wobbly wheel? The ride isn’t smooth, and you notice every bump in the road. As you focus on your discomfort, you may be distracted from the beautiful vistas you’re riding past. Think of the bicycle as your overall health, which carries you through life. For most of us, learning how to ride a bike begins in childhood as we learn…
Management of biofilm recommendations The Journal of Wound Care has published “Recommendations for the management of biofilm: a consensus document,” developed through the Italian Nursing Wound Healing Society. The panel that created the document identified 10 interventions strongly recommended for clinical practice; however, panel members noted that, “there is a paucity of reliable, well-conducted clinical trials which have produced clear evidence related to the effects of biofilm presence.”
Wound patient’s bill of rights The Association for Advancement of Wound Care has developed the “Wound Care Patient’s Bill of Rights.” The 10 points include the right to: • know what wound treatment options are available to you • know the benefits, risks, and side effects of your wound care treatments • participate in the development of your treatment plan with your wound care team • have…
Sad but true: Much of what we do as healthcare professionals is based on reimbursement. For nearly all the services and products we use in wound care and ostomy management, Medicare, Medicaid, and insurance companies control reimbursement. For many years, these payers have been deciding which interventions, medications, products, and equipment are the best, and then reimbursing only for those items. If we want to use something not on the list,…
Negative pressure wound therapy (NPWT) uses negative pressure to draw wound edges together, remove edema and infectious material, and promote perfusion and granulation tissue development. The tissue stretch and compression created by negative pressure during NPWT promotes tissue perfusion and granulation tissue development through angiogenesis, cellular proliferation, fibroblast migration, increased production of wound healing proteins, and reduction of wound area. NPWT has been used to improve healing in a variety of wounds, including traumatic…
It’s been a stressful day at work—nothing new. One confused patient pulled off her ostomy bag, you’re having difficulties applying negative-pressure wound therapy on another, and a third patient’s family is angry with you. We all experience stressful days, but unfortunately, sometimes we take our stress out on each other. Too often, this ineffective way of identifying and managing stress leads nurses to engage in lateral violence.
The goal of wound-bed preparation is to create a stable, well-vascularized environment that aids healing of chronic wounds. Without proper preparation, even the most expensive wound-care products and devices are unlikely to produce positive outcomes. To best prepare the wound bed, you need to understand wound healing physiology and wound care basics, as well as how to evaluate the patient’s overall health and manage wounds that don’t respond to treatment. (See…
On April 13, 2016, the National Pressure Ulcer Advisory Panel (NPUAP) announced changes in pressure ulcer terminology and staging definitions. Providers can adapt NPUAP’s changes for their clinical practice and documentation, but it’s important to note that, as of press time, the Centers for Medicare & Medicaid Services (CMS) has not adopted the changes. This means that providers can’t use NPUAP’s updates when completing CMS assessment forms, such as the Minimum…
Nurses and therapists often wonder if their license permits them to perform sharp wound debridement. Scope of practice varies significantly from state to state, so it’s imperative to check your state for specific guidance, but we can address some of the challenges clinicians face in deciding whether they can perform this valuable service for patients. Sharp debridement vs. other forms
The goal of wound-bed preparation is to create a stable, well-vascularized environment that aids healing of chronic wounds. Without proper preparation, even the most expensive wound-care products and devices are unlikely to produce positive outcomes.
To best prepare the wound bed, you need to understand wound healing physiology and wound care basics, as well as how to evaluate the patient’s overall health and manage wounds that don’t respond to treatment. (See Normal wound healing.)(more…)
Negative pressure wound therapy (NPWT) uses negative pressure to draw wound edges together, remove edema and infectious material, and promote perfusion and granulation tissue development. The tissue stretch and compression created by negative pressure during NPWT promotes tissue perfusion and granulation tissue development through angiogenesis, cellular proliferation, fibroblast migration, increased production of wound healing proteins, and reduction of wound area. NPWT has been used to improve healing in a variety of wounds, including traumatic injuries, surgical wounds, pressure ulcers, diabetic foot ulcers, and venous stasis ulcers. (more…)
Antibiotic resistance is a pressing public health threat not only in the United States, but worldwide. According to the World Health Organization (WHO), it is one of the major threats to human health.
Despite these concerns, antibiotics continue to be widely used—and overused. In long-term care, for instance, antibiotics are the most frequently prescribed medications, with as many as 70% of residents receiving one or more courses per year. And antibiotics are consistently ordered for suspected pressure ulcer infections.
Here is what clinicians who care for patients with wounds can do to help reduce antibiotic resistance. (more…)
According to the National Cancer Institute, an estimated 1.6 million new cases of cancer will have been diagnosed in the United States in 2015. During the course of their disease, most cancer patients receive radiation therapy.
Delivering high energy in the form of waves or particles, radiation therapy alters the DNA of cancer cells, causing their death. Radiation can be administered either externally or internally (through materials placed into the body). It’s given in fraction doses, with the total recommended dose divided into daily amounts. Treatment, including the total dose, is determined on an individual basis.
Although improvements have been made in delivery of radiation therapy, approximately 95% of patients who receive it experience a skin reaction. What’s more, radiation therapy commonly is given concurrently with chemotherapy or targeted therapy to improve survival, which increases the toxicity risk. (more…)
Using maggots to treat wounds dates back to 1931 in this country. Until the advent of antibiotics in the 1940s, maggots were used routinely. In the 1980s, interest in them revived due to the increasing emergence of antibiotic-resistant bacteria.
At Select Specialty Hospital Houston in Texas, we recently decided to try maggot therapy for a patient with a particularly difficult wound. In this case study, we share our experience. (more…)
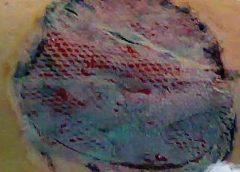
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when cells meet (contact inhibition). The ideal wound edge is attached to and flush with the wound bed, moist and open with the epithelial rim thin, and pale pink to translucent. (more…)
Diabetic foot ulcers stem from multiple factors, including peripheral neuropathy, high plantar pressures, decreased vascularity, and impaired wound healing. Contributing significantly to morbidity, they may cause limb loss and death. (See Foot ulcers and diabetes.)
Initially, hydrocolloid dressings were developed to function as part of the stomal flange. Based on their success in protecting peristomal skin, they were introduced gradually into other areas of wound care. They contain wafers of gel-forming polymers, such as gelatin, pectin, and cellulose agents, within a flexible water-resistant outer layer. The wafers absorb wound exudate, forming a gel and creating a moist healing environment. (more…)
We all lead busy lives, with demanding work schedules and home responsibilities that can thwart our best intentions. Although we know it’s our responsibility to stay abreast of changes in our field, we may feel overwhelmed when we try to make that happen.
Keeping clinicians up-to-date on clinical knowledge is one of the main goals of the Wild On Wounds (WOW) conference, held each September in Las Vegas. Each year, I present the opening session of this conference, called “The Buzz Report,” which focuses on the latest-breaking wound care news—what’s new, what’s now, what’s coming up. I discuss innovative new products, practice guidelines, resources, and tools from the last 12 months in skin, wound, and ostomy management. This article highlights the hottest topics from my 2015 Buzz Report. (more…)


















{kind=link}