One of the worst fears of a wound care clinician is inadvertently compressing a leg with critical limb ischemia—a condition marked by barely enough blood flow to sustain tissue life. Compression (as well as infection or injury) could lead to necrosis, the need for amputation, or even death. The gold standard of practice is to obtain an ankle-brachial index (ABI) before applying compression. However, recent research and expert opinion indicate an elevated or normal ABI is deceptive in patients with advanced diabetes. What’s worse, in the diabetic foot, skin may die from chronic capillary ischemia even when total blood perfusion is normal. For information on how to perform an ABI and interpret results, click on this link. (more…)
Digital cameras have many helpful features, but the most important considerations for choosing a camera are hardware features. Focus on the following when choosing a camera:
Resolution. The resolution determines picture quality. The National Pressure Ulcer Advisory Panel recommends using a digital camera with a minimum of 3 megapixels
for wound photography. A megapixel is 1 million pixels. The more pixels used to produce a photo, the less grainy it will appear and the clearer any enlargements made from it will be. In essence, the more megapixels a camera produces, the clearer and more detailed the photograph will be. (more…)
Clinical practice guidelines help ensure we are applying the latest knowledge and expertise when we’re caring for patients. Here are a few recent guidelines that you may find useful.
Measurement of ankle-brachial index
An American Heart Association scientific statement, “Measurement and interpretation of the ankle-brachial index (ABI),” published in Circulation, outlines the use of ABI, terminology, how to calculate the value, training, standards, and suggestions for future research.
Recommendations for obtaining an ABI measurement include:
• Use the Doppler method to determine the systolic blood pressure in each arm and each ankle.
• Use the appropriate cuff size, with a width of at least 40% of the limb circumference.
• Place the ankle cuff just above the malleoli with the straight wrapping method.
• Cover open lesions with the potential for contamination with an impermeable dressing.
• Avoid using a cuff over a distal bypass.
The article also recommends measurement and interpretation of ABI be part of the standard curriculum for nursing and medical students. For more information about ABI, read “Bedside ankle-brachial index testing: Time-saving tips” in this issue of Wound Care Advisor.
Childhood obesity continues to be a significant problem in the United States, requiring innovative approaches for prevention and management. Those who are obese run the risk of poorer wound healing.
“Approaches to the prevention and management of childhood obesity: The role of social networks and the use of social media and related electronic technologies: A scientific statement from the American Heart Association,” published in Circulation, evaluates the role of social networks and social media in relation to childhood obesity and presents five steps for using social networks: 1 Define the goal of the intervention. 2 Identify the social network. 3 Develop and pilot test the intervention. 4 Implement the intervention. 5 Spread the intervention.
The guidelines conclude that social media holds promise as a tool, but more research is needed.
Guidelines for managing patients with stable ischemic heart disease
Many patients with wound or ostomy needs have comorbid heart disease. Be sure you are aware of the most current information for managing these patients by accessing “2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease,” published in Circulation.
The guidelines acknowledge the vital importance of shared decision making between the healthcare provider and the patient. The information is divided into four sections with supporting algorithms:
• approaches to diagnosis
• risk assessment
• treatment
• follow-up.
Access the top 10 things to know and the executive summary.
In each case, the synthesis includes information in the following categories:
• areas of agreement and difference
• comparison of recommendations
• strength of evidence and recommendation grading schemes
• methodology
• source(s) of funding
• benefits and harms
• abbreviations
• status.
Access these and other guideline syntheses from AHRQ.
Bonus resource: Ethical case study of a patient refusing skin ulcer treatment
Free, one-time registration is required to view the entire video and all other
content on the Medscape website.
Patients have a right to make their own decisions, but what happens when a decision is so painful for staff that it affects morale? Arthur Caplan, PhD, Division of Medical Ethics at the NYU Langone Medical Center in New York, discusses such a case: “Patients have the right to choose death from bedsores.”
A hot flush of embarrassment creates a bead of sweat on my forehead. “I’ve got to get this measurement,” I plead to myself. One glance at the clock tells me this bedside ankle-brachial index (ABI) procedure has already taken more than 30 minutes. My stomach sinks as I realize I’ll have to abandon the test as inconclusive. (more…)
By Carrie Carls, BSN, RN, CWOCN, CHRN; Michael Molyneaux, MD; and William Ryan, CHT
Every year, 1.9% of patients with diabetes develop foot ulcers. Of those, 15% to 20% undergo an amputation within 5 years of ulcer onset. During their lifetimes, an estimated 25% of diabetic patients develop a foot ulcer. This article discusses use of hyperbaric oxygen therapy (HBOT) in treating diabetic foot ulcers, presenting several case studies.
HBOT involves intermittent administration of 100% oxygen inhaled at a pressure greater than sea level. It may be given in a:
• multi-place chamber (used to treat multiple patients at the same time), compressed to depth by air as the patient breathes 100% oxygen through a face mask or hood (more…)
Before discharge, a new ostomy patient and caregiver have a lot to learn, including how to empty the pouch, establish a schedule for pouch changes, measure the stoma to ensure protection from effluent, and use accessory supplies appropriately.
Lymphedema is characterized by regional immune dysfunction, distorted limb contours, and such skin changes as papillomas, hyperkeratosis, and increased girth. The condition may involve the limbs, face, neck, trunk, and external genitals; its effects may include psychological distress. For optimal patient management, clinicians must understand what causes lymphedema and how it’s diagnosed and treated.
This two-part series provides an overview of lymphedema. Part 1 covers etiology, pathology, and diagnosis. Part 2, which will appear in the November-
December issue, will focus on treatment.
Causes of lymphedema
Lymphedema occurs when protein-rich fluid accumulates in the interstitium due to impaired lymphatic function. Proteins, other macromolecular wastes, and water constitute lymphatic loads. These wastes rely on specially structured absorptive and transport structures in peripheral regions for their return to central circulation.
When lymph stasis prevails, inflammatory processes and lymphostatic fibrosis trigger tissue-density changes, further entrapping superficial vessels and accelerating mechanical insufficiency. (See Physiologic changes caused by lymphatic disruption by clicking the PDF icon above.)
Classifying lymphedema
Lymphedema can be primary or secondary. Primary lymphedema either is congenital (present at birth) or arises around puberty. In the vast majority of cases, it is associated with structural changes in the lymphatic system and isn’t associated with another disease or condition. Most structural changes (87%) manifest before age 35 and cause hypoplasia of vessels and nodes. Syndromes involving hyperplasia, node fibrosis, or aplasia also may occur, although they’re much less common. Dysplasia (either hypoplasia, hyperplasia, or aplasia) predisposes drainage regions to inadequate lymph collection, resulting in edema and secondary tissue changes, such as chronic inflammation and reactive fibrosis. Genetic variability in lymphatic constitution may explain why seemingly similar patients receiving the same surgical protocol have different lymphedema risks over time. Secondary lymphedema stems from a significant insult to lymphatic tissues, as from lymphadenectomy, radiation therapy, trauma, infection, or cancer. It commonly results from direct trauma to regional nodes or vessel structures. Slow degradation of lymphatic function also occurs when adjacent tissues (such as superficial and deep veins) become diseased, when cellulitis occurs, or when accumulations
of adipose or radiation fibrosis mechanical-ly disrupt drainage of skin lymphatics.
Lymphedema stages
Lymphedema progresses in stages, which involve secondary connective-tissue disease combined with disturbed fluid update and transport. These conditions cause a universal and classic clinical picture.
• Stage 0 (latency stage) is marked by reduced transport capacity and functional reserve. The patient has no visible or palpable edema, but has such subjective complaints as heaviness, tightness, and waterlogged sensations.
• In Stage 1 edema (reversible lymphedema), edema decreases with elevation. Pitting edema is present, but fibrosis is absent.
• During Stage 2 (spontaneously irreversible lymphedema), lymphedema doesn’t resolve entirely, although it may fluctuate. Pitting is more pronounced and fibrosis is present.
• Stage 3 (lymphostatic elephantiasis) is marked by dermal hardening, nonpitting edema, papillomas, hyperkeratosis, and in some cases, extreme girth.
Assessment and diagnosis
Diagnosing lymphedema can be challenging because edema may be associated with other diseases and disorders. For a summary of signs and symptoms, see Clinical findings in lymphedema by clicking the PDF icon above.
Discomfort and skin appearance
Lymphedema rarely causes pain because the skin accommodates gradual, insidious fluid accumulation. However, secondary orthopedic discomfort may result from increased weight of the affected limb due to deconditioning or decreased range of motion.
Because lymphedema usually progresses slowly, gravity and centrifugal forces pull fluids toward distal limb areas, causing an entrenched, stubborn pitting edema. Later, further valvular incompetence contributes to worsening distal edema in the fingers, toes, and dorsal regions of the hand and foot. Prominent lower-extremity structures, such as the malleolus, patella, tibia, anterior tibialis tendon, and Achilles tendon, become progressively less distinct. This creates a columnar limb appearance; the swollen limb has the same girth from distal to proximal aspects, unlike the natural cone shape of a normal limb.
Lymphatic failure doesn’t tax the venous system, so skin color remains normal. Blood supply remains patent, helping to prevent secondary ulcers.
Severity
Lymphedema severity correlates directly with such factors as onset of the condition and extent of cancer therapy, if given (number of nodes resected, number of positive nodes, and use of radiotherapy). Lymphedema may worsen with a greater number of infection episodes, weight gain, injury, diuretics, limb disuse, pneumatic compression therapy (when used for pure lymphedema), and ill-fitting compression garments. The single most important contributor to increasing lymphedema severity is lack of patient education, which can result in improper treatment or none at all.
Opportunistic infections
Lymphedema causes regional immune suppression and leads to an increase in opportunistic infections such as cellulitis. As skin integrity suffers, scaling and dryness allow resident skin pathogens (such as streptococci and staphylococci) to gain access through the defective skin barrier into protein-rich interstitial fluid, creating a medium favorable to bacterial colonization. Lymphocyte migration decreases, and dissected or irradiated nodal sites are slow to detect invaders. Furthermore, stagnant lymph promotes further delays in the immune response. Patients with opportunistic infections may exhibit high fever, local erythema, regional hypersensitivity or acute pain, flulike symptoms, and rapidly advancing “map-like” borders in the skin.
Differential diagnosis
Several methods can aid differential diagnosis. Clinical findings. Lymphedema can be diagnosed from patient history, physical examination, palpation, and inspection. Trauma to lymph nodes (each of which governs a distinct body region) decreases the transport capacity of lymph formed in that region, in turn causing local swelling (lymphedema). Trauma to the axillary or inguinal lymph nodes, which exist on both the left and right of the body and in both the upper and lower regions, predisposes these quadrants to swelling. Therefore, if lymph nodes on only one side are damaged, lymphedema occurs only on that side of the body. Using the universal characteristics cited above as a guide, while ruling out cancer recurrence, acute deep vein thrombosis, or plasma protein abnormalities, yields sufficient data to form a diagnosis. Imaging. Lymphography involves subcutaneous injection of a lymph vessel–
specific dye (Patent Blue V), followed by X-ray. Although it provides high-resolution images of lymphatic structures, this technique is invasive, painful, damaging to lymphatics, and potentially lethal—and therefore is no longer recommended.
Lymphangioscintigraphy (LAS) uses interdigital subcutaneous injection of protein-labeled radioisotopes, followed by
imaging at specific intervals to gather information about uptake and transport time. Images are hazy and false-negatives are common, so well-trained radiotherapists familiar with lymphology and lymphedema should administer and interpret the test. Also, experts don’t agree on standard criteria for LAS administration, so measures may not be similarly conclusive. Limb-measuring instruments and methods. Serial measurement of affected limb circumference using a standard garment tape measure is the most widely accessible approach. Intra-rater reliability is comparable to that of currently used tools; however, these methods can’t be used for early detection, for screening, or when various raters are used to assess the same patient. Circumferences are measured at four points and are considered positive if a distance of 2 cm or more separates the involved from uninvolved extremity in comparison. Water displacement techniques for limb-volume calculation, although accurate, are impractical in most clinical settings and rarely used.
Various devices have been used to obtain measurements. For instance, the Perometer® uses optoelectronic volumetry. By scanning the limb with infrared beams circumferentially, the device accurately records girth at 4-mm intervals along the limb length and transmits these measurements to a computer. The Perometer is used mainly in the research setting. Preoperative and postoperative measurements at intervals can detect lymphedema early.
Impedimed XCA® uses bioelectrical
impedance to calculate ratios of intracellular to extracellular fluid. A weak electrical current is passed through affected and unaffected limbs, allowing comparison of results. Impedance is lower in edematous tissue, supporting an accurate diagnosis.
Next step: Treatment
Once a diagnosis is made, the next step is treatment. Part 2 of this series covers lymphedema treatment.
Selected references
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
Kubik S, Manestar M. Anatomy of the lymph capillaries and precollectors of the skin. In: Bollinger A, Partsch H, Wolfe JHN, eds. The Initial Lymphatics. Stuttgart: Thieme-Verlag; 1985:66-74.
Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)—2009. Int Angiol. 2010 Oct;29(5):454-70.
Lerner R. Chronic lymphedema. In: Prasad H, Olsen ER, Sumpio BE, Chang JB, eds. Textbook of Angiology. Springer; 2000.
Mayrovitz HN. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology. 2009 June;42(2):88-98
Pecking AP, Alberini JL, Wartski M, et al. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008 Mar;41(1):1-10.
Stanton AW, Northfield JW, Holroyd, B, et al. Validation of an optoelectronic volumeter (Perometer). Lymphology. 1997 June;30(2):77-97
Weissleder H, Schuchhardt C. Lymphedema: Diagnosis and Therapy. 4th ed. Viavital Verlag GmbH; 2007.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
In the current healthcare environment, wound care practitioners need to capitalize on all available reimbursement avenues for care delivery and wound care supplies and dressings. And when it comes to reimbursement, there’s one constant: The rules change constantly. Whether these changes always benefit the patient is questionable. Nowhere is this more evident than in acute-care settings. Clinicians constantly are challenged to make sure their patient-care decisions comply with current Medicare reimbursement guidelines. (And if you’re not sure about today’s guidelines, be prepared for the guidelines to change tomorrow.) (more…)
The guideline updates IDSA’s 2004 diabetic foot infections guideline. It focuses on appropriate therapy, including debridement of dead tissue, appropriate antibiotic therapy, removing pressure on the wound, and assessing (and potentially improving) blood flow to the foot. The guideline also provides suggestions regarding when and how long antibiotics should be administered for soft-tissue and bone infections.
When diagnosing a diabetic patient with foot infection, the guideline recommends clinicians evaluate the patient at three levels—the patient as a whole, the affected foot or limb, and the infected wound. The guideline also provides advice on when and how to culture diabetic foot wounds.
Access a podcast on the guideline, which is available in a smartphone format and as a pocket-size quick-reference edition.
Combining bariatric surgery with medical therapy improves glycemic control
In obese patients with uncontrolled type 2 diabetes, bariatric surgery and 12 months of medical therapy significantly improved glycemic control compared to those who received only medical therapy, according to a study in The New England Journal of Medicine. “Bariatric surgery versus intensive medical therapy in obese patients with diabetes” was a randomized, nonblinded, single-center trial that included 150 patients in three groups: medical therapy only, medical therapy and Roux-en-Y gastric bypass, and medical therapy and sleeve gastrectomy.
Although glycemic control improved for all three groups, those who received bariatric surgery had better control. Use of drugs to lower glucose, lipid, and blood-pressure levels decreased significantly after both surgical procedures but increased in patients receiving medical therapy only. No deaths or life-threatening complications occurred.
HHS launches web-based tool for tracking healthcare performance
The U.S. Department of Health and Human Services (HHS) has launched a web-based tool for monitoring the performance of the healthcare system. The Health System Measurement Project gives providers and the public the ability to examine datasets from across the federal government that span specific topic areas, such as access to care, vulnerable populations, prevention, and quality. Users can also view indicators by population characteristics, such as age, sex, income level, insurance coverage, and geography.
PEG tubes may increase risk of new pressure ulcers
According to a study published in Archives of Internal Medicine, percutaneous endoscopic gastrostomy (PEG) tubes may increase the risk of pressure ulcers in nursing home patients with advanced cognitive impairment.
Researchers found that hospitalized patients who receive a PEG tube were 2.27 times more likely to develop a new pressure ulcer and those with a pressure ulcer were less likely to have it heal when they had a PEG tube. “Our findings regarding the risk of developing new stage 2 or higher pressure ulcers suggest that PEG feeding tubes are not beneficial, but in fact they may potentially harm patients,” conclude the researchers in “Feeding tubes and the prevention or healing of pressure ulcers.”
AHRQ provides QI toolkit for hospitals
The Agency for Healthcare Research and Quality (AHRQ) offers a toolkit designed to help hospitals understand AHRQ’s quality indicators (QIs). “AHRQ Quality Indicators™ Toolkit for Hospitals” includes steps for improvement, how to sustain change, and different tools for different audiences. Clinicians can also access audio interviews that provide information on how to use the tools and engage stakeholders and staff in QI efforts, and a recording of a webinar on the toolkit.
Silk fibers may be future resource for bone and tissue repair
Researchers at Tufts University have developed the first all-polymeric bone scaffold material that is fully biodegradable and capable of providing significant mechanical support during repair. The material could improve the way bones and tissues are repaired after an accident or following disease effects.
The new technology uses micron-size silk fibers to reinforce a silk matrix, much as steel rebar reinforces concrete. The study, “High-strength silk protein scaffolds for bone repair,” published in Proceedings of the National Academy of Sciences, found that the scaffold material is significantly less strong than normal bone, but it may play a role as a temporary biodegradable support for the patient’s cells to grow.
International guidelines for silver dressings in wounds released
A meeting of an international group of experts, convened by Wounds International, met in December 2011 to compile the consensus guidelines, which describe the patients who are most likely to benefit from silver dressings and how to use the dressings appropriately.
The guidelines recommend that silver dressings be used “in the context of accepted standard wound care for infected wounds or wounds that are at high risk of infection or reinfection.” Another recommendation is to use silver dressings for 2 weeks, then evaluate the wound, patient, and management approach before deciding whether to continue using the dressing or if a more aggressive intervention such as antibiotics would be better.
Cell therapy may benefit patients with lower extremity CLI
Injections of ixmyelocel-T in patients with lower extremity critical limb ischemia (CLI) who aren’t candidates for revascularization can prolong the time until treatment failure, according to a study in Molecular Therapy. Time to treatment failure was defined as major amputation, all-cause mortality, doubling of total wound surface area from baseline, or de novo gangrene. The double-blind, placebo-controlled RESTORE-CLI trial found that the adverse event rates were similar in the two groups.
New skin patch destroys skin cancer cells
A new skin patch destroyed facial basal cell carcinoma cells in 80% of patients, according to a study reported at the Society of Nuclear Medicine’s 2012 Annual Meeting.
Each of the 10 patients with facial basal cell carcinoma received a custom-made and fully sealed phosphorus-32 skin patch, a radiation spot-treatment in the form of a patch. Each patient was treated for 3 hours on the first day; the patches were reapplied on the fourth and seventh days after the first treatment for another 3 hours each. Three years after treatment, 8 of 10 patients were cancer-free.
The patients had lesions near the eyes, the nose, and forehead—areas more difficult to operate on, especially if skin grafting is needed later.
Small study links lymphedema to obesity
The average body-mass index (BMI) in obese patients with lymphedema was significantly greater than BMIs of obese patients without lymphedema, according to correspondence in The New England Journal of Medicine. The authors conclude, “Our findings suggest that obesity…may be a cause of lower-extremity lymphedema.”
“Lower-Extremity Lymphedema and Elevated Body-Mass Index” included 15 obese patients with bilateral lower-extremity enlargement who were referred to the authors’ center. Of the 15, five were diagnosed with lymphedema by lymphoscintigraphy.
Wound care has come a long way in just a few decades. With our expanded knowledge of wound healing and recent advances in treatment, we’re now able to assess wounds more accurately, recognize wound-related problems sooner, provide better interventions, and reduce morbidity.
To bring you up to date on current evidence-based wound management, this article focuses on assessing patients with chronic wounds, optimizing wound healing with effective wound-bed preparation, and selecting an appropriate dressing.
Wound chronicity and cause
Developing an appropriate plan of care hinges on conducting a thorough, accurate evaluation of both the patient and the wound. The first step is to determine whether the wound is acute or chronic.
• A chronic wound is one that fails to heal within a reasonable time—usually
3 months.
• An acute wound heals more quickly, causing minimal functional loss in the part of the body with the wound.
Identifying the cause of the wound also is essential. If the wound etiology is unknown, explore the patient’s medical history (including medication history) for clues to possible causes. Also review the patient’s history for conditions that could impede wound healing. (See What factors hamper healing? by clicking the PDF icon above)
Other important aspects of assessment include evaluating the patient’s nutritional status, quantifying the level of pain (if present), and gauging the patient’s self-care abilities.
General physical appearance
Conduct a general head-to-toe physical examination, focusing on the patient’s height, weight, and skin characteristics.
Height, weight, and weight trend
On admission, the patient’s height and weight should be measured to ensure appropriate nutritional and pharmacologic management. After a weight gain or loss, various factors may complicate wound healing. For instance, involuntary weight loss and protein-energy malnutrition may occur in both acute-care and long-term-care patients.
Especially note trends in your patient’s weight. For a long-term-care patient, a 5% weight loss over 30 days or a 10% loss over 180 days is considered involuntary. Arrange for a nutritional consult for any patient with an involuntary weight loss, as adequate nutrition is essential for general well-being and wound healing. (See A wound on the mend by clicking the PDF icon above.)
Skin color
Evaluate the patient’s skin color in light of ethnic background. If you note erythema—especially on a pressure point over a bony prominence—examine this area carefully for nonblanching erythema. Keep in mind that darkly pigmented skin doesn’t show such erythema and subsequent blanching, yet the patient may still be in jeopardy. So in dark-skinned patients, check for differences in skin color, temperature, or firmness compared to adjacent tissue; these differences may signify skin compromise.
Skin texture and turgor
Generally, healthy skin feels smooth and firm and has an even surface and good turgor (elasticity). To test turgor, gently grasp and pull up a fold of skin on a site such as the anterior chest below the clavicle. Does the skin return to place almost immediately after you release it, or does it stand up (“tent”)? Tenting indicates dehydration. But keep in mind that skin loses elasticity with age, so elderly patients normally have decreased turgor.
Skin temperature
With normal circulatory status, the skin is warm and its temperature is similar bilaterally. Areas of increased warmth or coolness suggest infection or compromised circulation. Be sure to check the temperature of skin surrounding the wound.
Wound assessment
Proper wound assessment can significantly influence patient outcome. Measure the wound carefully and document the condition of the wound bed. Remember that accurate descriptions are essential for guiding ongoing wound care. Repeat wound measurement and wound-bed assessment at least weekly, after the wound bed has been cleaned and debrided.
Keep in mind that assessing a chronic wound can be challenging. Wounds commonly have irregular shapes that can change quickly. Also, the multiple clinicians caring for the same patient may each describe the wound a bit differently.
Wound location
Note the precise anatomic location of the wound, as this can influence the wound care plan. A venous ulcer on the lower leg, for instance, requires different care than an arterial ulcer in the same site or a pressure ulcer on the ischium.
Circumference and depth
Use a paper or plastic measuring device to measure wound circumference and depth in centimeters (cm) or millimeters (mm). To promote accurate assessment of healing, be sure to use the same reference points each time you measure the wound.
You can use several methods to measure circumference. The most commonly used method of measurement is done in the head to toe direction. Measure the wound at its greatest length in that direction & measure the width at a 90 degree angle, at the widest point of the wound. Then multiply these two measurements (greatest length x greatest width) to obtain the total wound area. Although such linear measurements are imprecise, they yield gross information relative to wound healing when repeated over time.
Classify wound depth as partial thickness or full thickness.
• Partial-thickness wounds are limited to the skin layers and don’t penetrate the dermis. They usually heal by reepithelialization, in which epidermal cells regenerate and cover the wound. Abrasions, lacerations, and blisters are examples of partial-thickness wounds.
• Full-thickness wounds involve tissue loss below the dermis.
(Note: Pressure ulcers usually are classified by a four-stage system and diabetic foot ulcers by a grading system. Both systems are beyond this article’s scope.)
Measure and record wound depth based on the deepest area of tissue loss. To measure depth, gently place an appropriate device (such as a foam-tipped applicator) vertically in the deepest part of the wound, and mark the applicator at the patient’s skin level. Then measure from the end of the applicator to the mark to obtain depth.
Surrounding skin and tissue
Inspect for and document any erythema, edema, or ecchymosis within 4 cm of the wound edges, and reevaluate for these signs frequently. Because compromised skin near the wound is at risk for breakdown, preventive measures may be necessary.
Appearance of wound-bed tissue
Document viable tissue in the wound bed as granulation, epithelial, muscle, or subcutaneous tissue. Granulation tissue is connective tissue containing multiple small blood vessels, which aid rapid healing of the wound bed; appearing red or pink, it commonly looks shiny and granular. Epithelial tissue consists of regenerated epidermal cells across the wound bed; it may be shiny and silvery.
Check for nonviable tissue (also called necrotic, slough, or fibrin slough tissue), which may impede wound healing. It may vary in color from black or tan to yellow, and may adhere firmly or loosely to the wound bed. (See Picturing a necrotic wound by clicking the PDF icon above.)
Be sure to document the range of colors visible throughout the wound. Identify the color that covers the largest percentage of the wound bed. This color—and its significance—guide dressing selection.
Wound exudate
Document the amount, color, and odor of exudate (drainage) in the wound. Exudate with high protease levels and low growth factor levels may impede healing.
If the wound is covered by an occlusive dressing, assess exudate after the wound has been cleaned. Describe the amount of exudate as none, minimal, moderate, or heavy.
Describe exudate color as serous, serosanguineous, sanguineous, or purulent. Serous exudate is clear and watery, with no debris or blood present. Serosanguineous exudate is clear, watery, and tinged pink or pale red, denoting presence of blood. Sanguineous exudate is bloody, indicating active bleeding. Purulent exudate may range from yellow to green to brown or tan.
Describe wound odor as absent, faint, moderate, or strong. Note whether the odor is present only during dressing removal, if it disappears after the dressing is discarded, or if it permeates the room.
Wound edges
Wound edges indicate the epithelialization trend and suggest the possible cause and chronicity of the wound. The edges should attach to the wound bed. Edges that are rolled (a condition called epibole) indicate a chronic wound, in which epithelial cells are unable to adhere to a moist, healthy wound bed and can’t migrate across and resurface the wound.
Undermining and tracts
Gently probe around the wound edges and in the wound bed to check for undermining and tracts. Undermining, which may occur around the edges, presents as a space between the intact skin and wound bed (resembling a roof over part of the wound). It commonly results from shear forces in conjunction with sustained pressure. A tract, or tunnel, is a channel extending from one part of the wound through subcutaneous tissue or muscle to another part.
Measure the depth of a tract or undermining by inserting an appropriate device into the wound as far as it will go without forcing it. Then mark the skin on the outside where you can see or feel the applicator tip. Document your findings based on a clock face, with 12 o’clock representing the patient’s head and 6 o’clock denoting the feet. For instance, you might note “2.0-cm undermining from 7:00 to 9:00 position.”
Pain level
Ask the patient to quantify the level of pain caused by the wound, using the pain scale designated by your facility. Find out which pain-management techniques have relieved your patient’s pain in the past; as appropriate, incorporate these into a pain-management plan. Reevaluate the patient’s pain level regularly.
Wound-bed preparation
An evolving science, wound-bed preparation is crucial for minimizing or removing barriers to healing. The goal is to minimize factors that impair healing and maximize the effects of wound care. The key elements of wound-bed preparation are controlling bioburden and maintaining moisture balance. (For online resources on wound-bed preparation and other wound-care topics, see Where to get more information by clicking the PDF icon above.)
Controlling bioburden
Necrotic tissue and exudate harbor bacteria. A wound’s bioburden—the number of contaminating microbes—contributes to poor healing. All chronic wounds are considered contaminated or colonized, but not necessarily infected. In a colonized wound, healing is impeded as bacteria compete for nutrients; also, bacteria have harmful byproducts. To control bioburden, the wound must be cleaned and necrotic tissue must be debrided.
Cleaning the wound. Clean the wound before assessing it and applying a dressing. Use a noncytotoxic agent (typically, potable water, normal saline irrigating solution, or an appropriate wound-cleaning agent). Antiseptic solutions generally aren’t recommended for wound irrigation or dressings because they’re toxic to fibroblasts and other wound-repairing cells. If you must use such a solution, make sure it’s well diluted.
To ensure gentle cleaning or irrigation, pour solution over the wound bed or gently flush the wound with solution (using a 60-mL catheter-tip syringe) until the drainage clears. Know that pressurized irrigation techniques and whirlpool therapy aren’t recommended for wound cleaning because they disturb cell proliferation in the wound bed.
Debriding the wound. Debridement removes slough and necrotic tissue. Nonselective debridement techniques remove any type of tissue within the wound bed, whereas selective methods remove only necrotic tissue. (See Wound debridement techniques by clicking the PDF icon below.)
Maintaining moisture balance
To maintain moisture balance in the wound bed, you must manage exudate and keep the wound bed moist. The proper dressing (which may stay in place for days or longer) supports moist wound healing and exudate management. To minimize fluid pooling, a drain may be inserted into the wound. Negative-pressure wound therapy also may aid removal of excess exudate.
Choosing an appropriate dressing
The wound dressing plays a major role in maintaining moisture balance. Dressing selection is challenging because of the large number and variety of dressings available. Each product has specific actions, benefits, and drawbacks, so determining which dressing best suits the patient’s needs is a multifaceted process.
Dressing choice depends on such factors as wound type and appearance, exudate, presence or absence of pain, and required dressing change frequency. (See Dressings Options by clicking the PDF icon above.)
In a traditional dressing, gauze is applied in layers. The initial (contact) layer in the wound bed absorbs drainage and wicks it to the next layer; most often, this layer consists of woven cotton gauze or synthetic gauze. Remove the gauze gently, because it may be stuck to the wound or incision (especially if the gauze is cotton). For easier removal, moisten the dressing with normal saline solution to loosen it.
With a traditional dressing, the cover layer or secondary dressing is an abdominal pad with a “no-strike-through” layer next to the outside of the dressing. Be aware that wet-to-dry dressings are highly discouraged for their nonselective debriding effect and inability to provide a moist wound bed.
Reassess the patient’s wound at least weekly (after preparing the wound bed and dressing the wound) to determine healing progress. Keep in mind that wound-care management is a collaborative effort. Once you’ve assessed the patient, discuss your findings and subsequent wound management with other members of the team.
Wound care wisdom
Getting wiser about wound care will help your patients achieve good outcomes. Poor wound healing can be frustrating to patients, family members, and healthcare providers alike. Chronic wounds may necessitate lifestyle changes and lead to severe physical consequences ranging from infection to loss of function and even death. By performing careful assessment, tailoring patients’ wound care to wound etiology, and using evidence-based protocols to manage wounds, you can promote speedier wound healing, help lower morbidity, and improve quality of life.
Selected references
Bryant RA, Nix DP. Acute and Chronic Wounds: Current Management Concepts. 4th ed. St. Louis, MO: Mosby; 2011.
Gardener SE, Frantz R, Hillis SL, Park H, Scherubel M. Diagnostic validity of semiquantitative swab cultures. Wounds. 2007;(19)2:31-38.
Krasner DL, Rodeheaver GT, Sibbald RG. Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. 4th ed. Wayne, PA: HMP Communications; 2007.
Langemo DK, Brown G. Skin fails too: acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19(4):206-211.
Langemo DK, Anderson J, Hanson D, Hunter S, Thompson P. Measuring wound length, width, and area: which technique? Adv Skin Wound Care. 2008;21:42-45.
Milne C, Armand OC, Lassie M. A comparison of collagenase to hydrogel dressings in wound debridement. Wounds. 2010:22(11):270-274.
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Washington, DC: National Pressure Ulcer Advisory Panel; 2009.
Ovington LG. Hanging wet-to-dry dressings out to dry. Adv Skin Wound Care. 2002;15(2):79-86.
Sibbald RG, Coutts P, Woo KY. Reduction of bacterial burden and pain in chronic wounds using a new polyhexamethylene biguanide antimicrobial foam dressing—clinical trial results. Adv Skin Wound Care. 2011;24(2):78-84.
Solway DR, Consalter M, Levinson DJ. Microbial cellulose wound dressing in the treatment of skin tears in the frail elderly. Wounds. 2010:22(1):17-19.
Wound Ostomy and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers. Mt. Laurel, NJ: Author; 2010
Patricia A. Slachta is a Clinical Nurse Specialist at The Queens Medical Center in Honolulu, Hawaii and an adjunct nursing instructor at the Technical College of the Lowcountry in Beaufort, South Carolina.
By: Darlene Hanson, MS, RN, Pat Thompson, MS, RN, Diane Langemo, PhD, RN, FAAN, Susan Hunter, MS, RN, and Julie Anderson, PhD, RN, CCRC
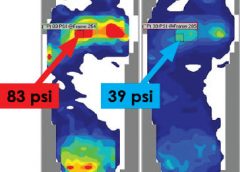
Faced with the nursing diagnosis of Impaired skin integrity, we’ve all written care plans that state our goal as “redistributing or reducing pressure.” But how do we do that? Which measures do we take? And how do we know that our interventions have relieved pressure? Do we rely solely on a skin assessment? A patient’s self-assessment of comfort? What if the patient can’t feel pressure relief because of neurologic impairment?
The answers to these questions may be that nurses should use pressure mapping, a tool used by occupational and physical therapists to determine seat-interface pressures and by other healthcare professionals to perform foot assessments. (more…)