By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS
Imagine your physician has just told you that your rectal pain and bleeding are caused by invasive colon cancer and you need prompt surgery. She then informs you that surgery will reroute your feces to an opening on your abdominal wall. You will be taught how to manage your new stoma by using specially made ostomy pouches, but will be able to lead a normal life.
Like most people, you’d probably be in shock after hearing this. More than 700,000 people in the United States are living with ostomies. Every year, at least 100,000 ostomy surgeries are done, preceded by a conversation much like the one above. So how do patients recover from the shock of learning about their pending surgery—and then return to a full life? (more…)
By Janice M. Beitz, PhD, RN, CS, CNOR, CWOCN, CRNP
Quality patient education is essential for comprehensive health care and will become reimbursable under healthcare reform in 2014. However, it’s difficult to provide effective education when time for patient interactions is limited. You can enhance your instruction time—and make your teaching more memorable—by using the techniques of analogy and metaphor. (more…)
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC
About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders.
A stoma has no sensory nerve endings and is insensitive to pain. Yet several complications can affect it, making accurate assessment crucial. These complications may occur during the immediate postoperative period, within 30 days after surgery, or later. Lifelong assessment by a healthcare provider with knowledge of ostomy surgeries and complications is important. (more…)
Study finds less-invasive method for identifying osteomyelitis is effective
Researchers have found that using hybrid 67Ga single-photon emission computed tomography and X-ray computed tomography (SPECT/CT) imaging combined with a bedside percutaneous bone puncture in patients with a positive scan is “accurate and safe” for diagnosing osteomyelitis in patients with diabetes who have a foot ulcer without signs of soft-tissue infection.
The new method, which avoids an invasive bone biopsy, has a sensitivity of 88% and a specificity of 93.6%. In the study of 55 patients, antibiotic treatment was avoided in 55% of suspected cases.
MRSA strains will likely continue to coexist in hospitals and communities
The strains of methicillin-resistant Staphylococcus aureus (MRSA) differ in the hospital and community settings, and both are likely to coexist in the future, according to a study in PLOS Pathogens.
C. difficile prevention actions fail to stop spread
Despite increasing activities to prevent the spread of Clostridium difficile, infection from C. difficile remains a problem in healthcare facilities, according to a survey of infection preventionists by the Association for Professionals in Infection Control and Epidemiology (APIC).
The survey found that 70% of preventionists have adopted additional interventions in their healthcare facilities since March 2010, but only 42% have seen a decline in C. difficile infection rates; 43% saw no decline.
A total of 1,087 APIC members completed the survey in January 2013. The survey also found that more than 92% of respondents have increased emphasis on environmental cleaning and equipment decontamination practices, but 64% said they rely on observation, rather than more accurate and reliable monitoring technologies, to assess cleaning effectiveness.
In addition, 60% of respondents have antimicrobial stewardship programs at their facilities, compared with 52% in 2010. Such programs promote the appropriate use of antibiotics, which can help reduce the risk of C. difficile infection.
Mast cells may not play significant role in wound healing
“Evidence that mast cells are not required for healing of splinted cutaneous excisional wounds in mice,” published in PLOS One, analyzed wound healing in three types of genetically mast-deficient mice and found they reepithelialized their wounds at rates similar to control mice. At the time of closure, the researchers found that scars in all the mice groups were similar in both “quality of collagen deposition and maturity of collagen fibers.” The findings fail to support the previously held belief that mast cells are important in wound healing.
Study identifies effective casting for diabetes-related plantar foot ulcers
Nonremovable casts that relieve pressure are more effective than removable casts or dressings alone for the treatment of plantar foot ulcers caused by diabetes, according to an analysis of clinical trials.
The authors of “Pressure-relieving interventions for treating diabetic foot ulcers,” published by The Cochrane Library, reviewed 14 randomized clinical trials that included 709 participants. Nonremovable pressure-relieving casts were compared to dressings alone, temporary therapeutic shoes, removable pressure-relieving devices, and surgical lengthening of the Achilles tendon.
The study also notes that when combined with Achilles tendon lengthening, nonremovable devices were more successful in one forefoot ulcer study than the use of a nonremovable cast alone.
Most studies were from the United States (five) and Italy (five), with Germany, the Netherlands, Australia, and India each contributing one study.
Prescriber preference drives use of antibiotics in long-term care
The study of 66,901 patients from 630 long-term care facilities found that 77.8%
received a course of antibiotics. The most common length (41%) was 7 days, but the length exceeded 7 days in 44.9% of patients. Patient characteristics were similar among short-, average-, and long-duration prescribers.
The study authors conclude: “Future trials should evaluate antibiotic stewardship interventions targeting prescriber preferences to systematically shorten average treatment durations to reduce the complications, costs, and resistance associated with antibiotic overuse.”
Electrophysical therapy may be helpful for diabetic foot ulcers
The authors of the study in International Wound Journal reviewed eight trials with a combined total of 325 patients. Five studies were on electrical stimulation, two on phototherapy, and one on ultrasound. Because of the small number of trials, the possibility of harmful effects can’t be ruled out, and the authors recommend “high-quality trials with larger sample sizes.”
Significant geographic variations in spending, mortality exist for diabetic patients with foot ulcers and amputations
The study in Journal of Diabetes and Its Complications found that higher spending wasn’t associated with a significant reduction in 1-year patient mortality. In addition, rates of hospital admission were associated with higher per capita spending and higher mortality rates for patients.
Home-based exercise program improves life for lymphedema patients
An individualized, home-based progressive resistance exercise program improves upper-limb volume and circumference and quality of life in postmastectomy patients with lymphedema, according to a study published in the Journal of Rehabilitation Research and Development.
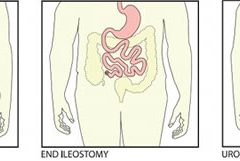
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Chronic venous insufficiency (CVI) is the most common cause of lower extremity wounds. The venous tree is defective, incapable of moving all the blood from the lower extremity back to the heart. This causes pooling of blood and intravascular fluid at the lowest gravitational point of the body—the ankle.
This article has two parts. Part 1 enhances your understanding of the disease and its clinical presentation. Part 2, which will appear in a later issue, explores the differential diagnosis of similar common diseases, the role that coexisting peripheral artery disease (PAD) may play, disease classification of venous insufficiency, and a general approach to therapy.
The most common form of lower extremity vascular disease, CVI affects 6 to 7 million people in the United States. Incidence increases with age and other risk factors. One study of 600 patients with CVI ulcers revealed that 50% had these ulcers for 7 to 9 months, 8% to 34% had them for more than 5 years, and 75% had recurrent ulcers.
Thrombotic complications of CVI include thrombophlebitis, which may range from superficial to extensive. If the thrombophlebitis extends up toward the common femoral vein leaving the leg, proximal ligation may be needed to prevent clot extension or embolization.
Understanding normal anatomy and physiology
Lower extremity veins flow horizontally from the superficial veins to the perforating veins and then into the deep veins. Normally, overall venous blood flows vertically against gravity from the foot and ankle upward toward the inferior vena cava (IVC). This antigravity flow toward the IVC results from muscular contraction around nonobstructed veins and one-way valves that close as blood passes them. These valves prevent abnormal backward blood flow toward the foot and ankle region.
The lower extremities have four types of veins. Superficial veins are located within the subcutaneous tissue between the dermis and muscular fascia. Examples are the greater and lesser (smaller) saphenous veins. Perforating veins connect the superficial veins to the deep veins of the leg. The deep veins are located below the muscular fascia. The communicating veins connect veins within the same system.
The greater saphenous vein is on the leg’s medial (inner) side. It originates from the dorsal veins on top of the foot and eventually drains into the common femoral vein in the groin region. By way of perforating veins, the greater saphenous vein drains into the deep venous system of both the calf and thigh.
The lesser saphenous vein is situated on the lateral (outer) side of the leg and originates from the lateral foot veins. As it ascends, it drains into the deep system at the popliteal vein behind the knee. Communicating veins connect the greater saphenous vein medially and the lesser saphenous vein laterally.
Intramuscular veins are the deep veins within the muscle itself, while the intermuscular veins are located between the muscle groups. The intermuscular veins are more important than other veins in development of chronic venous disease. Below the knee, the intermuscular veins are paired and take on the name of the artery they accompany—for example, paired anterior tibial, paired posterior tibial, and paired peroneal veins. Eventually, these veins form the popliteal vein behind the knee, which ultimately drains into the femoral vein of the groin.
As the common femoral vein travels below the inguinal ligament of the groin, it’s called the external iliac vein. Eventually, it becomes the common iliac vein, which drains directly into the IVC.
Pathophysiology
Abnormally elevated venous pressure stems from the leg’s inability to adequately drain blood from the leg toward the heart. Blood drainage from the leg requires the muscular pumping action of the leg onto the veins, which pump blood from the leg toward the heart as well as from the superficial veins toward the deep veins. Functioning one-way valves within the veins close when blood passes them, preventing blood from flowing backward toward the ankle. This process resembles what happens when you climb a ladder with intact rungs: As you step up from one rung to the next, you’re able to ascend.
CVI and the “broken rung” analogy
If the one-way valves are damaged or incompetent, the “broken rung” situation occurs. Think how hard it would be to climb a ladder with broken rungs: You might be able to ascend the ladder, but probably you would fall downward off the ladder due to the defective, broken rungs.
Normally, one-way valves ensure that blood flows from the lower leg toward the IVC and that the superficial venous system flows toward the deep venous system. The venous system must be patent (open) so blood flowing from the leg can flow upward toward the IVC. Blockage of a vein may result from an acute thrombosis (clot) in the superficial or deep systems. With time, blood may be rerouted around an obstructed vein. If the acute thrombosis involves one or more of the one-way valves, as the obstructing thrombosis opens up within the vein’s lumen, permanent valvular damage may occur, leading to post-thrombotic syndrome—a form of CVI.
CVI may result from an abnormality of any or all of the processes needed to drain blood from the leg—poor pumping action of the leg muscles, damage to the one-way valves, and blockage in the venous system. CVI commonly causes venous hypertension due to reversal of blood flow in the leg. Such abnormal flow may cause one or more of the following local effects:
leg swelling
tissue anoxia, inflammation, or necrosis
subcutaneous fibrosis
Compromised flow of venous blood or lymphatic fluid from the extremity.
“Water balloon” analogy
The effect of elevated venous pressure or hypertension is worst at the lowest gravitational point (around the ankle). Pooling of blood and intravascular fluid around the ankle causes a “water balloon” effect. A balloon inflated with water has a thin, easily traumatized wall. When it bursts, a large volume of fluid drains out. Due to its thicker wall, a collapsed balloon that contains less fluid is more difficult to break than one distended with water.
In a leg with CVI, subcutaneous fluid that builds up requires a weaker force to break the skin and ulcerate than does a nondistended leg with less fluid. This principle is the basis for compression therapy in treating and preventing CVI ulcers.
Effects of elevated venous pressure or hypertension
Increased pressure in the venous system causes:
abnormally high pressure in the superficial veins—60 to 90 mm Hg, compared to the normal pressure of 20 to 30 mm Hg
dilation and distortion of leg veins, because blood refluxes abnormally away from the heart and toward the lower leg and may move from the deep venous system into the superficial veins.
Abnormal vein swelling from elevated pressure in itself may impair an already abnormally functioning one-way valve. For instance, the valve may become more displaced due to the increase in intraluminal fluid, which may in turn worsen hypertension and cause an increase in leg swelling. Increased pressure from swollen veins also may dilate the capillary beds that drain into the veins; this may cause leakage of fluid and red blood cells from capillaries into the interstitial space, exacerbating leg swelling. Also, increased venous pressure may cause fibrinogen to leak from the intravascular plasma into the interstitial space. This leakage may create a fibrin cuff around the capillary bed, which may decrease the amount of oxygen entering the epidermis, increase tissue hypoxia, trigger leukocyte activation, increase capillary permeability, and cause local inflammation. These changes may lead to ulceration, lipodermatosclerosis, or both.
Visible changes may include dilated superficial veins, hemosiderin staining due to blood leakage from the venous tree, atrophie blanche, and lipodermatosclerosis. (See CVI glossary by clicking the PDF icon above.) Both atrophie blanche and lipodermatosclerosis result from local tissue scarring secondary to an inflammatory reaction of the leg distended with fluid.
Lipodermatosclerosis refers to scarring of subcutaneous tissue in severe venous insufficiency. Induration is associated with inflammation, which can cause the skin to bind to the subcutaneous tissue, causing narrowing of leg circumference. Lymphatic flow from the leg also may become compromised and inhibited in severe venous hypertension, causing additional leg swelling.
Patient history
In a patient with known or suspected CVI, a thorough history may lead to a working diagnosis. Be sure to ask the patient these questions:
Do you have pain?
Is your pain worse toward the end of the day?
Is the pain relieved with leg elevation at night?
Is it relieved with leg elevation during the day?
Do you have leg pain that awakens you at night?
How would you describe the pain?
Does the skin on your leg feel tight or irritated?
Have you noticed visible changes of your leg?
Do you have a leg ulcer?
Also determine if the patient has comorbidities that may exacerbate CVI, including PAD, renal failure, venous thrombosis, lymphedema, diabetes mellitus, heart failure, or malnutrition. (See CVI risk factors by clicking the PDF icon above .)
Common CVI symptoms
Approximately 20% of CVI patients have symptoms of the disease without physical findings. These symptoms may include:
tired, “heavy” legs that feel worse toward the end of the day
discomfort that worsens on standing
legs that feel best in the morning after sleeping or after the legs have been
elevated during the day.
Although patients may report leg discomfort, the history indicates that it doesn’t awaken them at night. Be aware that discomfort from CVI differs from that caused by PAD. With PAD, patients may report pain on exercise (claudication), pain with elevation (nocturnal pain), or constant pain (resting pain).
Signs of CVI (with or without ulcers) include:
leg swelling (seen in 25% to 75% of patients)
skin changes (such as hemosiderin staining or dermatitis)
telangiectasia, reticular veins, or both; while these are the most common signs, they represent an overall less severe finding
varicose veins with or without bleeding, occurring in one-third of patients with CVI.
Venous ulcers
Venous ulcers are the most common type of lower extremity ulcer. They’re commonly found on the medial aspect of the lower extremity, from the ankle to the more proximal calf area. Usually, they arise along the course of the greater saphenous vein, but also may be lateral and may occur at multiple locations. They aren’t found above the knee or on the forefoot. Venous ulcers are shallower than arterial ulcers and have considerable exudate consistent with drainage from a ruptured water balloon. They may extend completely around the leg.
CVI: From a heavy sensation to visible changes
In patients with CVI, blood flows within a lower extremity in an abnormal, reverse direction, causing build-up of blood and intravascular fluid around the ankle. Initially, this may cause only a sensation of heavy legs toward the end of the day, with no visible changes. Eventually, it may lead to venous ulcers or other visible changes. This abnormal blood flow results from dysfunction of the normal mechanisms that drain blood from the leg against gravity into the IVC.
Sardina D. Skin and Wound Management Course; Seminar Workbook. Wound Care Education Institute; 2011:92-112.
Donald A. Wollheim is a practicing wound care physician in southeastern Wisconsin. He also is an instructor for Wound Care Education Institute and Madison College. He serves on the Editorial Board for Wound Care Advisor.
Clinical practice guidelines help ensure we are applying the latest knowledge and expertise when we’re caring for patients. Here are a few recent guidelines that you may find useful.
Measurement of ankle-brachial index
An American Heart Association scientific statement, “Measurement and interpretation of the ankle-brachial index (ABI),” published in Circulation, outlines the use of ABI, terminology, how to calculate the value, training, standards, and suggestions for future research.
Recommendations for obtaining an ABI measurement include:
• Use the Doppler method to determine the systolic blood pressure in each arm and each ankle.
• Use the appropriate cuff size, with a width of at least 40% of the limb circumference.
• Place the ankle cuff just above the malleoli with the straight wrapping method.
• Cover open lesions with the potential for contamination with an impermeable dressing.
• Avoid using a cuff over a distal bypass.
The article also recommends measurement and interpretation of ABI be part of the standard curriculum for nursing and medical students. For more information about ABI, read “Bedside ankle-brachial index testing: Time-saving tips” in this issue of Wound Care Advisor.
Childhood obesity continues to be a significant problem in the United States, requiring innovative approaches for prevention and management. Those who are obese run the risk of poorer wound healing.
“Approaches to the prevention and management of childhood obesity: The role of social networks and the use of social media and related electronic technologies: A scientific statement from the American Heart Association,” published in Circulation, evaluates the role of social networks and social media in relation to childhood obesity and presents five steps for using social networks: 1 Define the goal of the intervention. 2 Identify the social network. 3 Develop and pilot test the intervention. 4 Implement the intervention. 5 Spread the intervention.
The guidelines conclude that social media holds promise as a tool, but more research is needed.
Guidelines for managing patients with stable ischemic heart disease
Many patients with wound or ostomy needs have comorbid heart disease. Be sure you are aware of the most current information for managing these patients by accessing “2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease,” published in Circulation.
The guidelines acknowledge the vital importance of shared decision making between the healthcare provider and the patient. The information is divided into four sections with supporting algorithms:
• approaches to diagnosis
• risk assessment
• treatment
• follow-up.
Access the top 10 things to know and the executive summary.
In each case, the synthesis includes information in the following categories:
• areas of agreement and difference
• comparison of recommendations
• strength of evidence and recommendation grading schemes
• methodology
• source(s) of funding
• benefits and harms
• abbreviations
• status.
Access these and other guideline syntheses from AHRQ.
Bonus resource: Ethical case study of a patient refusing skin ulcer treatment
Free, one-time registration is required to view the entire video and all other
content on the Medscape website.
Patients have a right to make their own decisions, but what happens when a decision is so painful for staff that it affects morale? Arthur Caplan, PhD, Division of Medical Ethics at the NYU Langone Medical Center in New York, discusses such a case: “Patients have the right to choose death from bedsores.”
Editor’s note: Part 1 of this series, published in the September-October issue, discussed lymphedema pathology and diagnosis. This article, Part 2, covers treatment.
Traditional treatment approaches
Traditionally, lymphedema treatment has been approached without a clear understanding of the underlying structure and function of lymphatic tissues. Ineffective traditional treatments include elevation, elastic garments, pneumatic pumps, surgery, diuretics, and benzopyrones (such as warfarin). Because many traditional treatments are still overused and some may be appropriate for limited use, it’s important for clinicians to understand these approaches.
Elevation
As a sole therapy for lymphedema, elevation of the affected part provides only short-lived results. Ever-increasing macromolecular wastes retain water against the effects of gravity. Increased interstitial colloid osmotic pressure must be addressed by interventions targeted at improving lymphatic function—not just a position change. Otherwise, lymphedema will progress. Furthermore, elevation alone is impractical, promotes deconditioning, and alters lifestyle for prolonged periods.
Elastic garments
Elastic garments prove inadequate because they attempt to treat lymphedema with compression alone. Medically correct garments are engineered with thoughtful attention to high-quality textiles and offer gradient support, which promotes proximal flow. However, without precise tissue stimulation leading to improved lymphangioactivity (lymph-vessel pulsation), macromolecular wastes can’t be removed.
Interstitial pressure increases caused by compression garments impede further fluid accumulation. When these garments are removed, the spontaneous girth increase causes an imprecise fit, and the garment rapidly leads to a countertherapeutic effect. Furthermore, compression garments don’t combat the osmotic forces generated by ever-increasing interstitial wastes. Except in patients diagnosed with stage 0 or stage 1 lymphedema, disease progression involving metaplasia ensues. Although elastic compression garments are a cornerstone of long-term management, they shouldn’t be used as a stand-alone treatment.
Pneumatic compression pump
Formerly, the pneumatic compression pump (PCP) was considered the standard of care for lymphedema. However, when inflated, the pump doesn’t increase the frequency of lymph-vessel contraction or enhance lymph capillary absorption. What’s more, accelerated fibrosis development and rapid tissue refilling occur when a PCP is removed. Also, PCP use disregards the ipsilateral territory of the excised regional nodes, effectively dumping fluid from the leg into the trunk. A PCP is appropriate only when nothing else is available, as it may worsen the patient’s condition.
Surgery
Surgical approaches to treating lymphedema involve either excisional (debulking) or microsurgical techniques. The most extensive surgical technique, the radical Charles procedure, completely debulks all involved tissue down to the muscle fascia. Split-thickness grafts are then harvested from excised skin and donor sites, and applied to the fascia to achieve so-called limb reduction.
Most debulking procedures have been applied to lower-extremity lymphedema and offer poor cosmetic results. Less radical surgeries favor long incisions, preserving the skin but excising subcutaneous edematous portions to reduce girth. Although less cosmetically alarming, these procedures effectively amputate the subcutaneous space where lymph vessels reside. Other surgical approaches are beyond the scope of this article.
Generally, surgery isn’t a good approach for any patient, as it’s linked to significant morbidity, such as skin necrosis, infection, and sensory changes. In the future, less invasive procedures may be available that yield significant improvement without these adverse effects.
Diuretics
Although diuretics are prescribed appropriately to address water-rich edemas of venous origin, they disregard the fact that lymphedema is a protein-rich edema. Long-term, high-dose diuretic therapy leads to treatment-resistant limbs, similar to those that have received intensive pneumatic compression.
Benzopyrones
Benzopyrones such as warfarin decrease swelling by combating protein accumulation in fluid. Such drugs have undergone clinical trials abroad. Their mechanism is to promote macrophage migration into interstitial fluid, as well as subsequent proteolysis. Due to significant risk of liver damage or failure, benzopyrones haven’t been approved for treating lymphedema.
Complete decongestive therapy: The current treatment approach
Currently, the gold standard for lymphedema treatment is complete decongestive therapy (CDT). Michael Foeldi and Etelka Foeldi, who originated this method, discovered a unique symbiotic relationship among five distinct modalities that addresses the challenges of lymphedema treatment. In 1989, CDT was brought to the United States by Robert Lerner and has become the mainstay of lymphedema treatment here.
CDT is a two-phase approach involving an intensive clinical effort followed by a semi-intensive home-care program geared toward autonomous management, stabilization, and continual improvement. It involves manual lymph drainage (MLD), compression bandaging, exercise, skin and nail hygiene, and self-care education. (See Phases of complete decongestive therapy by clicking the PDF icon above.)
Manual lymph drainage
A type of soft-tissue mobilization, MLD provides skin traction, stimulating superficial lymph vessels and nodes. Lymph capillaries contain large inter-endothelial inlets called swinging tips, akin to overlapping shingles. Each overlapping cell is tethered to the interstitial matrix by anchoring filaments, so that fluid increases cause immediate distention and lymph inflow. Manual skin traction using MLD promotes greater lymph fluid uptake by stretching these filamentous structures, opening the swinging tips.
MLD also provides extrinsic stimulation of the lymphangion (the segment of a lymph vessel between a distal and proximal valve), drawing fluid into the system at the capillary level and promoting flow at the vessel level toward regional lymph nodes. Usually, these segments contract and relax in a rhythmic fashion six times per minute. MLD triples this output to 18 or 20 times per minute, greatly enhancing systemic transport.
MLD requires intensive daily treatment sessions to strengthen collateral flow as a pathway to circumventing surgical or developmental lymphatic disruption. Treatment strategies further recruit more deeply situated lymphatics such as the thoracic duct, as well as lumbar trunks that empty at the juncture of the internal jugular and subclavian veins to improve global uptake. MLD thus stimulates deeper vessel angioactivity to help drain the superficial vessels that drain toward them.
Compression bandaging
Compression bandaging provides tissue support after MLD to prevent reflux, slow new fluid formation, and mechanically soften fibrotic areas. Bandaging techniques provide a high working pressure to harness the muscle and joint pumps as a propellant for lymph while resisting retrograde flow created by gravity and centrifugal forces during movement. Pure cotton materials coupled with specialized padding create a soft, castlike environment, which confines swollen tissues without constriction. By relying on high working pressure and low resting pressures to decrease limb swelling, this strategy achieves greater control over intensity (level of compression/pressure exerted), with little to no soft-tissue injury or discomfort.
The patient wears this bulky inelastic complex after each MLD treatment until the next day’s session to ensure limb-volume reduction in a stable, linear fashion. Once a plateau is reached, tissue stabilization and self-care education are the goals of additional sessions.
Exercise
Exercise always must be done with adequate support to counteract fluid formation. During the intensive CDT phase, limbs are bandaged to provide complete around-the-clock containment. Gentle exercises encourage blood flow into the muscle; during muscle contraction, this creates a favorable internal pressure that effectively squeezes the subcutaneous space between the bandage wall and muscle. Because every bandage strives to provide a gradient of support, fluid tends to drain proximally to the bandage—in most cases, to the trunk.
Skin and nail hygiene
Without intact, well-hydrated skin, cellulitic infections occur in many lymphedema patients whose immune response has been diminished by regional lymphadenectomy or inherited deficiencies. To prevent infection caused by avoidable external events, patients receive clear guidelines to reinforce appropriate behavior. As most cellulitis results from resident skin pathogens (streptococci and staphylococci), maintaining a low skin pH helps control colonization. Ways to avoid recurrent infections include maintaining an acid mantle on the skin using low-pH-formulated lotions and avoiding injury from daily tasks that may scratch, puncture, burn, or abrade the skin. Patients should receive lists of self-care precautions at the time of treatment.
Self-care education
Because lymphedema is a chronic condition, patients must receive self-care education for daily management to avoid lymphedema destabilization, which can lead to tissue saturation and subsequent skin changes. Therapists must provide patients with appropriate self-care tools and knowledge to maintain adequate treatment results. Teaching topics include how to apply and remove compression garments and bandages and how to exercise safely, preserve skin integrity, monitor for infection, and respond appropriately to infection and significant changes in limb mobility.
An underrecognized and mistreated problem
Lymphedema remains an underrecognized and mistreated condition, even though CDT yields safe, reliable results. Early detection, accurate staging, proper diagnosis, and appropriate treatment can slow the inevitable progression of lymphedema. Wound care specialists should adapt wound therapy to address not just the wound but the edematous environment responsible for delayed wound resolution.
Selected references
Al-Niaimi F, Cox N. Cellulitis and lymphedema: a vicious cycle. J Lymphoedema. 2009;4:38-42.
Browse N, Burnand KG, Mortimer PS. Diseases of the Lymphatics. London: Hodder Arnold; 2003.
Casley-Smith JR, Casley-Smith JR. Modern Treatment for Lymphoedema. 5th ed. The Lymphoedema Association of Australia; 1997.
Cooper R, White R. Cutaneous infections in lymphoedema. J Lymphoedema. 2009:4:44-8.
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. Consensus Document of the International Society of Lymphology. Lymphology. 2009 Jun;42(2):51-60.
Leduc A, Bastin R, Bourgeois P. Lymphatic reabsorption of proteins and pressotherapies. Progress in Lymphology XI. 1988:591-2.
National Lymphedema Network Medical Advisory Committee. Position Statement: Lymphedema Risk Reduction Practices. Revised May 2012. http://www.lymphnet.org/pdfDocs/nlnriskreduction.pdf. Accessed September 5, 2012.
Pappas CJ, O’Donnell TF Jr. Long-term results of compression treatment for lymphedema. J Vasc Surg. 1992 Oct;16(4):555-62.
Whittlinger H. Textbook of Dr. Vodder’s Manual Lymphatic Drainage. Vol 1. 7th ed. New York, NY: Thieme; 2003.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Lymphedema is characterized by regional immune dysfunction, distorted limb contours, and such skin changes as papillomas, hyperkeratosis, and increased girth. The condition may involve the limbs, face, neck, trunk, and external genitals; its effects may include psychological distress. For optimal patient management, clinicians must understand what causes lymphedema and how it’s diagnosed and treated.
This two-part series provides an overview of lymphedema. Part 1 covers etiology, pathology, and diagnosis. Part 2, which will appear in the November-
December issue, will focus on treatment.
Causes of lymphedema
Lymphedema occurs when protein-rich fluid accumulates in the interstitium due to impaired lymphatic function. Proteins, other macromolecular wastes, and water constitute lymphatic loads. These wastes rely on specially structured absorptive and transport structures in peripheral regions for their return to central circulation.
When lymph stasis prevails, inflammatory processes and lymphostatic fibrosis trigger tissue-density changes, further entrapping superficial vessels and accelerating mechanical insufficiency. (See Physiologic changes caused by lymphatic disruption by clicking the PDF icon above.)
Classifying lymphedema
Lymphedema can be primary or secondary. Primary lymphedema either is congenital (present at birth) or arises around puberty. In the vast majority of cases, it is associated with structural changes in the lymphatic system and isn’t associated with another disease or condition. Most structural changes (87%) manifest before age 35 and cause hypoplasia of vessels and nodes. Syndromes involving hyperplasia, node fibrosis, or aplasia also may occur, although they’re much less common. Dysplasia (either hypoplasia, hyperplasia, or aplasia) predisposes drainage regions to inadequate lymph collection, resulting in edema and secondary tissue changes, such as chronic inflammation and reactive fibrosis. Genetic variability in lymphatic constitution may explain why seemingly similar patients receiving the same surgical protocol have different lymphedema risks over time. Secondary lymphedema stems from a significant insult to lymphatic tissues, as from lymphadenectomy, radiation therapy, trauma, infection, or cancer. It commonly results from direct trauma to regional nodes or vessel structures. Slow degradation of lymphatic function also occurs when adjacent tissues (such as superficial and deep veins) become diseased, when cellulitis occurs, or when accumulations
of adipose or radiation fibrosis mechanical-ly disrupt drainage of skin lymphatics.
Lymphedema stages
Lymphedema progresses in stages, which involve secondary connective-tissue disease combined with disturbed fluid update and transport. These conditions cause a universal and classic clinical picture.
• Stage 0 (latency stage) is marked by reduced transport capacity and functional reserve. The patient has no visible or palpable edema, but has such subjective complaints as heaviness, tightness, and waterlogged sensations.
• In Stage 1 edema (reversible lymphedema), edema decreases with elevation. Pitting edema is present, but fibrosis is absent.
• During Stage 2 (spontaneously irreversible lymphedema), lymphedema doesn’t resolve entirely, although it may fluctuate. Pitting is more pronounced and fibrosis is present.
• Stage 3 (lymphostatic elephantiasis) is marked by dermal hardening, nonpitting edema, papillomas, hyperkeratosis, and in some cases, extreme girth.
Assessment and diagnosis
Diagnosing lymphedema can be challenging because edema may be associated with other diseases and disorders. For a summary of signs and symptoms, see Clinical findings in lymphedema by clicking the PDF icon above.
Discomfort and skin appearance
Lymphedema rarely causes pain because the skin accommodates gradual, insidious fluid accumulation. However, secondary orthopedic discomfort may result from increased weight of the affected limb due to deconditioning or decreased range of motion.
Because lymphedema usually progresses slowly, gravity and centrifugal forces pull fluids toward distal limb areas, causing an entrenched, stubborn pitting edema. Later, further valvular incompetence contributes to worsening distal edema in the fingers, toes, and dorsal regions of the hand and foot. Prominent lower-extremity structures, such as the malleolus, patella, tibia, anterior tibialis tendon, and Achilles tendon, become progressively less distinct. This creates a columnar limb appearance; the swollen limb has the same girth from distal to proximal aspects, unlike the natural cone shape of a normal limb.
Lymphatic failure doesn’t tax the venous system, so skin color remains normal. Blood supply remains patent, helping to prevent secondary ulcers.
Severity
Lymphedema severity correlates directly with such factors as onset of the condition and extent of cancer therapy, if given (number of nodes resected, number of positive nodes, and use of radiotherapy). Lymphedema may worsen with a greater number of infection episodes, weight gain, injury, diuretics, limb disuse, pneumatic compression therapy (when used for pure lymphedema), and ill-fitting compression garments. The single most important contributor to increasing lymphedema severity is lack of patient education, which can result in improper treatment or none at all.
Opportunistic infections
Lymphedema causes regional immune suppression and leads to an increase in opportunistic infections such as cellulitis. As skin integrity suffers, scaling and dryness allow resident skin pathogens (such as streptococci and staphylococci) to gain access through the defective skin barrier into protein-rich interstitial fluid, creating a medium favorable to bacterial colonization. Lymphocyte migration decreases, and dissected or irradiated nodal sites are slow to detect invaders. Furthermore, stagnant lymph promotes further delays in the immune response. Patients with opportunistic infections may exhibit high fever, local erythema, regional hypersensitivity or acute pain, flulike symptoms, and rapidly advancing “map-like” borders in the skin.
Differential diagnosis
Several methods can aid differential diagnosis. Clinical findings. Lymphedema can be diagnosed from patient history, physical examination, palpation, and inspection. Trauma to lymph nodes (each of which governs a distinct body region) decreases the transport capacity of lymph formed in that region, in turn causing local swelling (lymphedema). Trauma to the axillary or inguinal lymph nodes, which exist on both the left and right of the body and in both the upper and lower regions, predisposes these quadrants to swelling. Therefore, if lymph nodes on only one side are damaged, lymphedema occurs only on that side of the body. Using the universal characteristics cited above as a guide, while ruling out cancer recurrence, acute deep vein thrombosis, or plasma protein abnormalities, yields sufficient data to form a diagnosis. Imaging. Lymphography involves subcutaneous injection of a lymph vessel–
specific dye (Patent Blue V), followed by X-ray. Although it provides high-resolution images of lymphatic structures, this technique is invasive, painful, damaging to lymphatics, and potentially lethal—and therefore is no longer recommended.
Lymphangioscintigraphy (LAS) uses interdigital subcutaneous injection of protein-labeled radioisotopes, followed by
imaging at specific intervals to gather information about uptake and transport time. Images are hazy and false-negatives are common, so well-trained radiotherapists familiar with lymphology and lymphedema should administer and interpret the test. Also, experts don’t agree on standard criteria for LAS administration, so measures may not be similarly conclusive. Limb-measuring instruments and methods. Serial measurement of affected limb circumference using a standard garment tape measure is the most widely accessible approach. Intra-rater reliability is comparable to that of currently used tools; however, these methods can’t be used for early detection, for screening, or when various raters are used to assess the same patient. Circumferences are measured at four points and are considered positive if a distance of 2 cm or more separates the involved from uninvolved extremity in comparison. Water displacement techniques for limb-volume calculation, although accurate, are impractical in most clinical settings and rarely used.
Various devices have been used to obtain measurements. For instance, the Perometer® uses optoelectronic volumetry. By scanning the limb with infrared beams circumferentially, the device accurately records girth at 4-mm intervals along the limb length and transmits these measurements to a computer. The Perometer is used mainly in the research setting. Preoperative and postoperative measurements at intervals can detect lymphedema early.
Impedimed XCA® uses bioelectrical
impedance to calculate ratios of intracellular to extracellular fluid. A weak electrical current is passed through affected and unaffected limbs, allowing comparison of results. Impedance is lower in edematous tissue, supporting an accurate diagnosis.
Next step: Treatment
Once a diagnosis is made, the next step is treatment. Part 2 of this series covers lymphedema treatment.
Selected references
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
Kubik S, Manestar M. Anatomy of the lymph capillaries and precollectors of the skin. In: Bollinger A, Partsch H, Wolfe JHN, eds. The Initial Lymphatics. Stuttgart: Thieme-Verlag; 1985:66-74.
Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)—2009. Int Angiol. 2010 Oct;29(5):454-70.
Lerner R. Chronic lymphedema. In: Prasad H, Olsen ER, Sumpio BE, Chang JB, eds. Textbook of Angiology. Springer; 2000.
Mayrovitz HN. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology. 2009 June;42(2):88-98
Pecking AP, Alberini JL, Wartski M, et al. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008 Mar;41(1):1-10.
Stanton AW, Northfield JW, Holroyd, B, et al. Validation of an optoelectronic volumeter (Perometer). Lymphology. 1997 June;30(2):77-97
Weissleder H, Schuchhardt C. Lymphedema: Diagnosis and Therapy. 4th ed. Viavital Verlag GmbH; 2007.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Jim, a 52-year-old patient with colon cancer, received a new ostomy. He needed a custom fit for his appliance, which took 10 days. During this time, trying to obtain a good seal and treat the peristomal area wasn’t easy. Despite my best efforts, Jim’s skin was denuded from contact with stool. Although he was in great discomfort, he wanted to wait until my next visit to tell me about the problem. Fortunately, his wife was worried and contacted me directly.
Jim lives in a neighborhood with a low crime rate, so I’m able to see him within a few hours of his wife’s call, even though it’s late at night. As it turns out, I make extra visits to help him manage his stoma until the customized appliance is ready.As with any home care situation, I’m ready to do my best for my patient.
Many home-care patients like Jim benefit from the interventions of a wound care clinician (WCC). More than one-third of all home-care admissions are wound related, and home wound care has become one of the fastest growing needs and skills in home-care services. So if you’re a WCC, you may want to consider home care as a practice option.
Delivering wound care in the home differs dramatically from delivering it in the hospital. Given the complexity of wound care and the multiple factors that affect healing, home wound care is a challenge. Some patients have chronic conditions, such as diabetes or wounds or open sores that don’t heal easily. In other cases, the patient or caregiver is unable to change dressings. That’s where the WCC comes in.
Special needs of home-care patients
Like other patients across the continuum of care, home-care wound patients require accurate and thorough wound assessment, as well as documentation that provides information about wound status and aids development of a plan that supports healing.
Of course, the plan of care must address the whole patient, not just the “hole” in the patient. The WCC must take into account comorbidities, individual wound-care requirements, assistance the patient may need due to physical or mental deficits, and nutritional support. Additional factors that affect wound-care strategies include wound characteristics, family support, and insurance guidelines and reimbursement.
Role of the WCC
The WCC’s role in home care includes providing clinical expertise, working with other healthcare team members, and providing education.
The WCC provides clinical expertise regarding wound and ostomy care to ensure delivery of the highest quality of care. This expertise helps reduce the need for readmissions to the emergency department (ED) for wound-related complications. The WCC also plays a vital role in product awareness, formu-lary development, and maintenance of cost-effective, evidence-based practice in the agency.
Working with other healthcare team members, the WCC serves as patient advocate, strengthening the relationship between patient and healthcare team members while promoting care coordination to help the patient achieve goals. Effective communication with the patient’s primary care provider is essential to delivering the best-quality, research-based wound care. A tool for strengthening such communication is the SBAR (Situation-Background-Assessment-Recommendation) technique. SBAR structures conversations so all parties provide complete yet concise information. (See SBAR wound and skin provider communication record by clicking the PDF icon above).
The WCC educates patients and family members about wound healing, dressing applications, and other interventions. Teaching families allows them to be involved in the patient’s care and start to take ownership of it. The WCC also educates home health aides, who can play a vital role in preventing such problems as pressure ulcers and may be responsible for ensuring staff members are aware of the products, procedures, and dressings available.
Challenges of home care
If you’re a WCC and considering home care as a career option, know that practicing in the home can be a real eye opener. For starters, consider geography. Shortly after I started as a wound care nurse/consultant in home care, I was visiting patients all over New Jersey, some days driving 200 miles. As I quickly discovered, once you enter the home, don’t assume you’ll simply change a dressing and then be on your way. Instead, you may find you are, in essence, the family case manager who’s expected to “fix everything.” This role requires equal doses of planning and creativity.
What’s more, expect to do some improvising. In acute-care settings, all the supplies you may need to prevent infection—gowns, gloves, masks—usually are within arm’s reach. But in home care, these supplies may be absent, meaning you’ll need to set up the cleanest environment you can under the circumstances. That might mean using disposable drapes and dressings. Be sure to carry large amounts of hand sanitizer.
Dressing selection is perhaps the biggest challenge in home wound care because
it involves not just wound-specific issues but financial and practical considerations. The ideal dressing in the home is one that needs to be changed only every other day, at most. Evidence shows it’s not practical to try to change dressings two or three times daily at home unless the family is providing care.
Develop a checklist
Because the home environment may lack all the resources you need, remembering everything you need to do before you leave the patient’s home may be challenging. To help keep things on track, develop a checklist of reminders that covers these points:
Have necessary medical appointments been arranged? Does the patient have transportation to appointments?
Are there sufficient supplies in the home?
Is there enough medicine? If not, who will pick up the medicine?
Are consults needed, such as social worker or physical therapist?
Who will help with any activities of daily living that the patient is unable to do?
Does the patient with diabetes have a glucometer?
Hours and safety concerns
Typical home wound-care hours are 8:30 a.m. to 4:30 p.m. But realistically, expect variations. For instance, as you’re about to leave, the patient might say, “My wife isn’t feeling well. Could you take her blood pressure?” This means you’ll stay a little longer.
When planning home visits, be aware of safety concerns. If visiting after hours could put you in danger, it’s safer to instruct the patient to call an ambulance and go to the local ED.
Reimbursement
Reimbursement is an important factor in wound care in the home. To be eligible for home care through Medicare, patients must be homebound—meaning they don’t routinely travel to run errands or visit or they’re not able to obtain or receive needed medical services. (With private insurance and workers’ compensation, eligibility requirements may be less restrictive.)
Know that a Medicare patient receives home care as an “episode.” Episodes are 60-day periods; within each 60-day episode, a $592 cap is allotted should a patient require supplies for wound or ostomy care needs. Except for negative-pressure wound therapy, a home care agency can’t bill Medicare for products used; instead, the home-care agency is responsible for the cost of all topical wound-care products and dressings. Agencies may keep patients on service even if they exceed the allowed amount, although patients reaching maximum benefits commonly are discharged from service. Home-care agencies have no choice but to discharge Medicare patients they find aren’t truly homebound.
Also, be aware that Medicare views home health service as an interim service. When a patient is no longer making progress, Medicare expects that the family will provide the patient’s care or the patient will enter a skilled care facility. So it’s important to work hard to obtain good outcomes—not just for the patient but to maintain Medicare reimbursement. Like many private insurance companies, Medicare reimbursement is based on pay for performance; if an agency doesn’t deliver optimal outcomes, it receives lower reimbursement, increasing its financial burden.
A worthwhile option
WCCs use their knowledge and clinical expertise to improve patient outcomes and teach patients, families, and other healthcare team members. They also give the agency recommendations for care and supplies that are evidence based and reflect current best practices in wound care. Accomplishing these goals in a timely fashion under various constraints can be challenging. But if you choose to work in the home, try to keep a smile on your face and joy in your voice for each patient and family. If you like challenges and want a job where you can apply your creativity and function independently, becoming a home-care WCC might be the right choice for you.
Connie Johnson provides wound care in the home and in acute-care settings.
Often nurses get named in a lawsuit when they are involved in clearly negligent conduct that causes an injury to or the death of a patient. Examples include administering the wrong medication to the wrong patient or not positioning a patient correctly in the operative suite prior to surgery. Sometimes, however, the negligent behavior of a nurse is not as clear to the nurse involved in the care of the patient.
That was apparently the circumstance in the reported case, Olsten Health Services, Inc v. Cody.¹ In September 2000, Mr. Cody was the victim of a crime that resulted in paraplegia. He was admitted to a rehabilitation center and discharged on November 15, 2000. His physician ordered daily home health care services in order to monitor his “almost healed” Stage 2 pressure ulcer.² The home health care agency assigned a registered nurse (RN) to Mr. Cody and, after Mr. Cody’s healthcare insurance company would not approve daily visits, a reduced visit plan was approved by Mr. Cody’s physician.
A progressive problem
On November 16, 2000, the nurse visited Mr. Cody for the first time. During that visit, she did an admission assessment and noted that the pressure ulcer, located at the area
of the tailbone, measured 5 cm by 0.4 cm wide and 0.2 cm deep. She believed the pressure ulcer could be completely healed within 3 weeks. The nurse called Mr. Cody’s physician and left him a voice message concerning her visit and her findings.
On November 19, a second visit took place and the nurse observed and documented that Mr. Cody’s pressure ulcer was “100%” pink and no odor was detected.
On November 20, she attempted another visit but did not see Mr. Cody because the front gate surrounding his home was locked. The nurse buzzed the gate doorbell several times to no avail. She left a note on the front gate for the Cody family and left a voice message for Mr. Cody’s physician.
The next visit took place on November 21. The pressure ulcer was now only “90% pink” and had a “fetid” odor; this condition did not improve over the next 24 hours. The nurse documented this fact in her nurses’ notes. Again, she left a voice mail message for the physician concerning these findings.
The nurse could not get into the house on November 23, the next scheduled visit, so she again left a note on the house gate and left a voice mail message for the physician.
On November 24, the home health care nurse saw Mr. Cody and observed the pressure ulcer to be “90% pink” but the “fetid” odor was still present. In addition, Mr. Cody’s right lower extremity was swollen. She was concerned that the wound care that was to be done by the family or the health aide was not being done. Even so, she did not contact Mr. Cody’s physician or the patient again until November 27.
Mr. Cody’s pressure ulcer on November 27 had no odor but the home health aide who was also caring for Mr. Cody told the nurse that he was “very cold and having chills.” The nurse did not document this reported observation in her nurses’ notes.
Attempts to visit Mr. Cody on November 28 and 29 were again unsuccessful because of the locked gate at the front of the house. No one answered the buzzer, either. The nurse left another note on the house gate and left a voice mail message for the physician.
When the nurse saw Mr. Cody on November 30, she observed that the ulcer had “serious changes”: an increase in the serous drainage from the wound; the wound had a “fetid” odor; 80% of the wound was necrotic; the necrotic tissue was “undermined”; and the wound was significantly larger—9 cm by 8 cm wide and 1 cm deep.3 She left a voice mail message for Mr. Cody’s physician, but did not alter her visits to Mr. Cody’s home or attempt to see him over the next 2 days.
Admission to hospital
When the nurse did visit Mr. Cody on December 1, the pressure ulcer consisted of 40% necrotic tissue. She then told the family to take Mr. Cody to the physician’s office. Later that same day he was admitted to the hospital with a Stage 4 pressure ulcer that reached his tailbone. After 3 weeks of treatment, the ulcer measured 20 cm by 30 cm.
Mr. Cody endured many procedures during the following years to treat his
ulcer, but it never really healed. A “flap” enclosure was done to try to cover the wound.
Lawsuit
Mr. Cody sued the home health care company, alleging that the employees breached the standard of care by failing to appropriately diagnose and treat/or to prevent the formation or aggravation of pressure ulcers, resulting in severe and significant injury to him.
Verdict
The Florida Court of Appeals affirmed the trial court’s verdict in favor of Mr. Cody—a $3,050,000 verdict in economic damages4—on several legal bases, the most important for the purposes of this article being that the home health care agency and its employees were negligent in the care of Mr. Cody.
Key testimony
Key testimony in reaching this verdict came from the expert testimony of an RN and certified wound care expert. The nurse expert testified unequivocally that the home health care nurse breached the standard of nursing care. She said that not contacting the physician personally about Mr. Cody’s condition and the family being overwhelmed about his condition, but instead leaving voice mail messages on an answering machine, did not meet the standard of nursing care in this situation.
Additionally, the nurse expert testified that the nurse caring for Mr. Cody failed to recognize the symptoms of his deteriorating condition and did not intervene when necessary to avoid the infection he suffered from the deteriorating wound, and that her failure to do so resulted in the development of the Stage 4 ulcer that never healed.
Take-away points
So, what does this case tell you as a wound care professional caring for someone who has a pressure ulcer?
Meet the standard of care. You must always meet the standard of care when caring for a patient. That means your care must be what other ordinary, reasonable, and prudent nurses caring for a patient with a decubitus ulcer would do in the same or similar circumstances in the same or similar community. Clearly, the nurse did not meet this standard in her care of Mr. Cody.
Document accurately and completely. Remember that the nurse did not document Mr. Cody’s condition when the home health aide reported it to her. This omission may not only have compromised Mr. Cody’s care. If the communication during the trial became an “I told her”/”I don’t remember being told” debate when each party testified about the communication, it surely caused a rift between the aide and the nurse during the trial proceedings. Such a disagreement between defendant employees always helps a plaintiff’s case.
Know that photographs can be used in court. This case used a specific form of evidence, demonstrative evidence: photographs taken of the pressure ulcer, which were admitted into evidence during the trial. The photographs were testified to by the wound care expert. In addition to her testimony, this evidence further showed the “natural and continual progression” of the ulcer as it existed on December 1, 2000.
Understand the importance of expert testimony. In professional negligence cases, expert testimony is essential to establish the standard of care and to provide an opinion as to whether the standard of care was met or breached, the breach of which led to the injury to the patient. Typically, the attorney of a nurse cited in this type of case would want to use a certified wound care expert to support the care given. Apparently, the home care agency’s expert witness was not as convincing as the expert witness’s testimony for Mr. Cody.
Indeed, in this case, the expert witness’s testimony was invaluable and essentially secured a verdict for the plaintiff. Not only was the expert witness board certified but her testimony was credible, based on the evidence presented, and given after a careful review of Mr. Cody’s medical records, admission and discharge summaries from hospitals and health centers that provided care to Mr. Cody, the depositions of several doctors and nurses, and Mr. Cody’s deposition.
Know your limits. The nurse’s conduct also stresses the importance of another legal principle—knowing the limits of your abilities and capabilities. Nowhere in the reported opinion are the RN’s qualifications listed or a reason given as to why she was selected to care for Mr. Cody. It is assumed she was not certified. Even basic nursing guidelines for wound care and communication to the physician were not followed. Why, then, did she agree to take this assignment? She did so not only at her own folly but to the detriment of Mr. Cody.
Protect your patient. Last, and by no means least, this case stands for the principle that if you simply document something in the patient’s record that
is important regarding the patient’s well-being and you just leave voice mail messages for a physician about that “something,” such conduct is not adequate. By simply leaving messages and notes, this RN violated an age-old principle in the law of professional negligence.5
Your duty in any situation in which the patient is at risk for a foreseeable and unreasonable risk of harm is to prevent that harm from happening insofar as humanly possible. What those specific steps might be will depend on the circumstances and your patient’s condition. Remember, liability is always fact-specific. Although legal principles exist, how each applies to a particular situation may vary.
Mr. Cody was clearly at risk for a foreseeable and unreasonable risk of harm—the further deterioration of his pressure ulcer. The nurse would only have had to intervene sooner by, for example (and as testified to by the expert witness), personally talking with his physician, visiting the patient more frequently when the deterioration began, contacting social services to help the family with its “overwhelmed” feelings, and following up with the home health aide’s observations of Mr. Cody.
Think about this, too: Nowhere in the court of appeals’ record was it indicated that Mr. Cody’s family or the physician ever received the notes or voice mail messages left by the nurse.6 At a minimum, wouldn’t you as the nurse want to follow up and check if those communications had been received?
4. Id. at 2. The doctrine of comparative negligence was used in this case. This doctrine, adopted by most states, reduces a plaintiff’s recovery of money proportionally to the plaintiff’s degree of fault in causing the injury that is the basis of the suit (Blacks Law Dictionary, Second Pocket Edition, Bryan Garner, ed. St. Paul, MN: West; 2001). In this case, the home health care agency’s fault was attributed to be 70%. Mr. Cody’s degree of fault was assessed by the jury at 30%, most probably due to the inability of the home care nurse to be given access into the house on the days she visited and the family not providing the wound care required by Mr. Cody’s decubitus ulcer.
5. This age-old principle was established in a 1965 Illinois case, Darling v. Charleston Community Hospital, 211 N.E. 2d 353 (IL Supreme CT) 1965.
6. Tammelleo D. Treatment of decubitus ulcers botched: verdict for $3,050,000. Nurs Law Regan Rep. 2008;49(1):1.
Nancy J. Brent is an attorney in Wilmette, Illinois. The information in this article is for educational purposes only and does not constitute legal advice.
The alarm clock goes off too early, and you jump-start the day with a cup of coffee and a short stack of reasons why you hate your job. Sound familiar? Although you can’t expect to love every aspect of your job, you should expect to get some degree of fulfillment from your career. If you don’t, maybe your job isn’t the problem. Maybe you just need a little career resuscitation to turn things around. First, let’s be clear. I’m not urging you to stay in a job that exposes you to unsafe conditions, a toxic environment, or a toxic boss. Call the code and get out, because emotional and physical well-being comes first. However, know that blaming our jobs for our dissatisfaction may be easier than taking a closer look at the chaos in our lives. It’s even easier not to fix what’s wrong, instead consoling ourselves with the company of like-suffering people. And misery does love company.
If you can’t have the job you love, love the job you have. The daily grind of Herculean demands can wear down even the most conscientious clinicians—to the point where we’re no longer seeking job satisfaction but struggling just to make it through the day. But you can turn things around. To enhance your job satisfaction, try these sure-fire methods. (Okay, maybe they’re not sure-fire, but they’re sure worth a try.)
Know when to say no
When your life feels out of balance, any demand will feel as if it’s sucking the living daylights out of you. You’ll be tempted to blame your job, when the truth is you’re giving in to a bottomless pit called “trying to please everyone else.” Learn to say no to the things you don’t want and say yes to more of what you do want. Say no to anything that’s not a priority (making cupcakes for the second-grade class). Say yes to quality time with your family and quality time for you (that painting class you’ve always wanted to take). Key question: How would the quality of your life improve if you started to say no to demands that don’t enhance its quality, and say yes to the things you want more of?
Learn to see the big picture again
Recognize that, in ways you can’t see or perhaps even imagine, you’ve forever touched and changed the lives of the patients you’ve cared for. The ability to touch and heal another person is a gift that’s available to few people in other professions, who struggle to find meaning in what they do. Key questions: In what ways have you helped your patients? What special qualities and skills are uniquely yours to give? How can you make the most of the opportunity to make a difference in patients’ lives?
Attract the positive
When we’re miserable, other miserable people gravitate to us. Soon a collective mindset takes root and the negative “group think” becomes a life-form unto
itself, festering and insatiable. So be careful of the company you keep. Surround yourself with positive people—clinicians committed to making a difference. This will reenergize you and give you a new perspective on your job.
Learn to be what you want
To be more passionate about your job,
focus on the aspects of the job that excite you the most. Passion is an energy form that attracts more of the same. Say, for instance, you’d love to buy a red convertible. One day you go out for a drive and you see red convertibles everywhere! Have more red convertibles suddenly driven off the assembly line? No; your mind is preselecting, or noticing the convertibles, for you. In the same way, you can preselect either more passion or more misery.
Pay it forward
Keep in mind that novice clinicians proceed through a learning curve. Rather than moan about how inexperienced they are, take one under your wing and turn her or him into the sort of clinician you’d want at your bedside if you were ill. You’ll rediscover your profession through this clinician’s eyes.
Communicate cleanly and ask for what you want
People can’t read your mind. To get more of what you want and less of what you don’t want, learn to communicate in a clean, neutral way. Let’s say you consistently wind up with the more difficult patient assignments. And let’s assume your boss does that because you’re the most clinically experienced clinician—not because she’s the devil incarnate. You can respond in one of two ways.
• Gripe to a coworker: “Can you believe she gave me that workload again?”
• Communicate with your boss cleanly and neutrally: “Lately it seems you’ve given me the more difficult patient assignments, and I appreciate your faith in me. Is there some way we can give other clinicians a chance to gain more experience caring for difficult patients? I’d be happy to act as a resource for them.”
See the difference? The first response does nothing to change the situation; it simply fuels the collective misery mindset. The second response communicates to the boss in a respectful, appreciative way (yes, bosses need appreciation, too!) and seeks a solution that pleases everyone.
Take action and follow your STAR
Using the mnemonic device “STAR” can guide you toward actions that increase your job satisfaction.
Success on your terms. We all define success differently. If you grew up in a family of college professors, chances are the healthcare field didn’t fit your family’s definition of success; your job dissatisfaction may stem from your inner turmoil over not meeting your family’s expectations. To key into these expectations, recall the “you should” and “you ought to” messages you heard as a child.
Key question: Take a moment to think about what success in your career would look and feel like. Then complete this sentence: “I know I will be successful when I have/I am _________.”
True north as your guide. A large part of how we judge ourselves, our worth, our success, and our happiness hinges on how other people see us. But true success, true happiness, and true job satisfaction are determined from within, by your inner compass. The captain of a ship must always know where true north is, because it never changes (much like our core values). He must know the difference between true north and compass north. Unlike true north, compass north is affected by the earth’s magnetic pull. In life, compass north is the magnetic pull of “you should do this” and “you ought to do that” messages. For instance, if you’re a skilled wound care clinician but have always been particularly passionate about lymphedema, you may dislike your job. That’s because you’ve ignored your true north (inner truth) and given in to compass north (fear of walking away from those current skills, and so forth). Don’t be afraid to follow your true north.
Key question: What steps can you take right now that will move you closer to your true north?
Assess and understand who you are. Most of us can articulate what our strengths are. But that’s not enough. To get more enjoyment from your job, you must stretch and exercise your strengths and look for ways to use them. If the opportunities aren’t there, create them.
Let’s say you’re the one everyone turns to for help when there’s a patient with a lower extremity ulcer. To leverage that strength, offer to hold an education program.
Key questions: List your strengths, and then ask yourself: How can I leverage these? If you’re too humble to recognize your strengths, give yourself 20 lashes (figuratively speaking); then ask a trusted colleague, “What do you see as my strengths?”
Risk it all (within reason). When we play it safe, our lives and careers can be pretty dull. We’re meant to push the envelope and stretch our capabilities. It puts the juice back in our lives and helps us grow and feel more alive. Nothing shakes out the cobwebs and brings excitement back to your career more than taking a risk. With every risk comes the threat of failure, but know that failure is just another form of data that helps you readjust and move forward. Don’t give failure more power than your successes.
Key questions: If you weren’t afraid, what risks would you consider taking to enhance your career? What’s holding you back?
Embrace change
An Eastern saying goes something like this: You can stand by a river, but you can never put your feet in the same place twice. The river is your life. It’s not stagnant; it’s ever changing. Nothing in life stays the same—not personal circumstances, relationships, or careers. You aren’t the clinician you were 10 years ago or even last year. So tweak your professional life to better reflect the clinician you are today. With a little attention, you could make your job the career of your dreams.
Joan C. Borgatti, MEd, RN, is the owner of Borgatti Communications in Wellesley Hills, Mass., which provides writing, editing, and coaching services. You may e-mail her at [email protected].