Achieving excellent wound care outcomes can be challenging, given the growing number of high-risk patients admitted to healthcare facilities today. Many of these patients have comorbidities, such as obesity, diabetes, renal disease, smoking, chronic obstructive pulmonary disease, and poor nutritional status. These conditions reduce wound-healing ability. (more…)
By Janice M. Beitz, PhD, RN, CS, CNOR, CWOCN, CRNP
Quality patient education is essential for comprehensive health care and will become reimbursable under healthcare reform in 2014. However, it’s difficult to provide effective education when time for patient interactions is limited. You can enhance your instruction time—and make your teaching more memorable—by using the techniques of analogy and metaphor. (more…)
Navigating through the thousands of wound care products can be overwhelming and confusing. I suspect that if you checked your supply rooms and treatment carts today, you would find stacks of unused products. You also would probably find that many products were past their expiration dates and that you have duplicate products in the same category, but with different brand names. Many clinicians order a product by brand name, not realizing that plenty of the product is already in stock under a different brand name. (more…)
Colleen Jackson recently was promoted to a manager position on her unit. At first, she was thrilled with the opportunity to advance her leadership skills, but now she’s having second thoughts. She doesn’t feel confident in her new role and worries how her team views her. She confesses to her manager, “I keep thinking someone will figure out how much I really don’t know and question whether I should’ve been given the position. Sometimes I feel like an imposter. When I mention this to my friends, they tell me to ‘fake it until you make it.’ But I’m not so sure about that!”
Colleen isn’t alone in feeling like an imposter. In imposter syndrome, a person doesn’t feel good enough, is unsure of what she’s doing, and feels she can’t live up to others’ expectations. She may be afraid she’ll be found out as an imposter at any moment. The syndrome is most common among women leaders who feel they don’t deserve the success they’ve achieved despite external evidence of their competence. It’s more likely in perfectionists who constantly compare themselves to others.
Certain situations, such as taking on a new role, can lead to imposter syndrome. For instance, Colleen may think that because she was seen as qualified for her new role, others expect her to immediately have expert knowledge. If, like Colleen, you feel you don’t deserve the career success you’ve had, you may experience deep feelings of inauthenticity and fear you’ll be found out as a fake. (See Inside the imposter syndrome.)
In small doses, feelings of inadequacy may not be a bad thing, because they remind us to work on building our competency. But people with imposter syndrome feel a level of self-doubt that can lead to overwork and a paralyzing fear of failure. The fear of being unmasked causes incredible stress. Colleen and others like her may have unrealistic expectations of themselves in a new role—expectations that can compromise their success.
Overcoming imposter syndrome
For people with imposter syndrome, the response to their success may rest too heavily on others’ approval, recognition, and opinions. A wise mentor once told me we can easily overestimate how much time others spend thinking about us and our behaviors. Most people, she observed, are self-absorbed. This is important to consider, because the idea that Colleen is an imposter probably has never crossed her team members’ minds.
Imposter syndrome can create performance anxiety and lead to perfectionism, burnout, and depression. So learning how to manage these feelings is important. Cathy Robinson-Walker, MBA, MCC, who coaches nurse leaders, provides advice to help cope with imposter syndrome. Her recommendations include the six actions steps below.
Discuss your feelings with a trusted mentor.
Sharing your insecurities with someone you trust and respect can help you separate what’s real from your perceptions of insecurity. A trusted mentor might inform Colleen she’s making good progress as a beginning leader and that no one expects her to be an expert at this point. The mentor can provide guidance about specific areas where Colleen might need additional growth and how to best go about this.
Pay attention to your own self-talk and consider whether your thoughts are empowering or disabling.
Do you often say to yourself, “I achieved this only because I work harder than anyone else, not because I’m more competent”? Valerie Young, author of The Secret Thoughts of Successful Women: Why Capable People Suffer from the Impostor Syndrome and How to Thrive in Spite of It, makes a strong case that your internal script is a well-rehearsed pattern that serves as a key to feelings of being an imposter. She cautions that individuals with imposter syndrome may sabotage themselves as a way of holding back, due to feelings of being a fraud.
Instead, choose a different script and talk yourself down during times of self-doubt. Instead of thinking, “I’m the wrong person for this job,” retrain yourself to say, “I have a lot to offer in this position.”
Make of list your strengths.
Take the time to make a written list your strengths and what you contribute. Ask others for input, and refer to the list in times of self-doubt. If you’re in a new role, remember that you were chosen for a reason. In Colleen’s case, her supervisor saw her leadership potential. Also realize that most people overestimate their abilities; people with imposter syndrome underestimate theirs.
Accept that perfection is unrealistic and costly.
Trying to be perfect and feeling you need to “know it all” is unrealistic and can be costly on a personal level. Perfectionists typically believe anything short of a flawless performance all the time is unacceptable. But none of us can live a mistake-free life; we all make errors. Those with imposter syndrome hold themselves to impossibly high standards and feel shame, insecurity, and low self-esteem when they don’t meet their own expectations. But progress, not perfection, is what really matters.
Know you’ll need to develop your competencies at certain times in your career.
Throughout your career, you’ll go through periods when you’re on a steep learning curve and will need to further develop your competencies. You may feel like a novice and have to work hard to build new competencies.
Be honest about what you know and don’t know, and seek advice from experts on your unit or in your organization. The simple act of saying, “This is new for me, and I’m working hard to learn this role” can be empowering. Colleen, for instance, might be surprised at others’ reactions to hearing this from her. They might perceive her as a more authentic leader.
Be willing to be uncomfortable and move through your fear.
In Fear of Flying, author Erica Jong urges readers engaging in new experiences to feel the fear and do it anyway. Fear is a useful emotion, as long as it doesn’t escalate to the level of paralyzing behaviors. Practice and preparation can help ease new leaders’ fears. The fear of new challenges will never truly go away, but it can be managed.
Building competence leads to competency
People with imposter syndrome generally are intelligent, thoughtful, and capable but lack self-confidence. Over time, clinicians like Colleen will grow out of feeling like an imposter as they build their competency and become more comfortable in their roles. Eleanor Roosevelt said, “I believe that anyone can conquer fear by doing the things he fears to do, provided he keeps doing them until he gets a record of successful experience behind him.” If you feel like an imposter, this is good advice to ponder.
Selected references
Clance PR, Imes S. The imposter phenomenon in high achieving women: dynamics and therapeutic intervention. Psycho Theor, Res and Prac.1978;15(3):241-7.
Jong E. Fear of Flying. Austin, TX: Holt, Reinhart & Winston; 1973.
Robinson-Walker C. The imposter syndrome. Nurs Leader. 2011;9(4):12-13.
Young V. The Secret Thoughts of Successful Women: Why Capable People Suffer from the Impostor Syndrome and How to Thrive in Spite of It. New York: Crown Business; 2011.
Rose O. Sherman is an associate professor of nursing and director of the Nursing Leadership Institute at the Christine E. Lynn College of Nursing at Florida Atlantic University in Boca Raton. You can read her blog at www.emergingrnleader.com.
Knowledge is exploding online, making it essential that you’re comfortable using the Internet. You can also go online to save time and find a job, among other tasks. (See Online value.)
However, you also need to keep in mind that anyone can put information on the Internet. As the caption of a cartoon by Peter Steiner, published in The New Yorker says, “On the Internet, nobody knows you’re a dog.” (more…)
What an honor it is to be the wound care “superhero”—the guru, the healer, the go-to person. Unfortunately, this honor may be accompanied by wound care overload—too much to do in too little time.
Once someone is crowned the superhero specialist, others may try to transfer every aspect of wound and skin care to that person—all treatment plans, assessments, documentation, prevention, education, and accountability. Superheroes don’t cry, so they don’t complain about the workload. Yet, the overload must be controlled. (more…)
One of the worst fears of a wound care clinician is inadvertently compressing a leg with critical limb ischemia—a condition marked by barely enough blood flow to sustain tissue life. Compression (as well as infection or injury) could lead to necrosis, the need for amputation, or even death. The gold standard of practice is to obtain an ankle-brachial index (ABI) before applying compression. However, recent research and expert opinion indicate an elevated or normal ABI is deceptive in patients with advanced diabetes. What’s worse, in the diabetic foot, skin may die from chronic capillary ischemia even when total blood perfusion is normal. For information on how to perform an ABI and interpret results, click on this link. (more…)
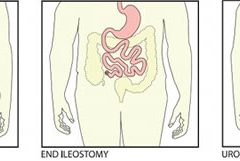
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
As clinicians, we’re proud of the expert care we provide patients. But we also know that just doing our job isn’t enough to advance our careers. Mastering good communication skills is essential for all clinicians at all career stages—especially with today’s flatter organizational structures and more participatory management styles. Knowing how to communicate in a professional manner can give you the edge you need for career advancement.
Opportunity rarely knocks any more. Instead it may present as a phone call, voice mail, e-mail, or text message. Be sure to use proper etiquette with all communication forms.
Speaking with managers
When dealing with your manager, use a solution-focused approach. Don’t be a complainer. Some communication experts point out that people complain about things they can do something about—not things they have no power over. For example, they don’t complain about their foot size because there’s nothing they can do about it. Yet people often complain about their jobs because they’re unwilling to take the risk of making a change.
We need to take charge of our lives. We can accept the fact—without complaining—that we’re making the choice to stay where we are. Or we can make a request or take action to achieve a desired outcome. Suppose you work on a clinical unit and disagree with the way your manager makes clinical assignments. You have several options:
Complain to coworkers and make the workplace miserable for others.
Speak with your manager and make suggestions for improvement.
Leave your job and go elsewhere if you can’t work with your manager to make things better.
If you decide to stay in your job, accept the fact that you’ve made that choice. Take responsibility for it and stop complaining.
Speaking on the phone with physicians
For clinicians who are not physicians, the key to effective communication with physicians is to remember you’re an important member of the healthcare team. An effective way to guide your communication with physicians and other colleagues is to use a tool such as SBAR (Situation, Background, Assessment, Recommendation). Say, for instance, you want to suggest the doctor order an anxiolytic for your patient. Here’s how you might do it using SBAR:
Situation: “Mrs. Smith is complaining of severe anxiety.” Background: “She is 1 day post-op from a lumbar laminectomy.” Assessment: “She is alert and oriented and her vital signs are stable. She has no numbness or tingling in her extremities.” Recommendation: “She said she takes lorazepam 2 mg orally at when she’s anxious. Would you like to order something for her?”
Before ending the conversation, repeat and clarify the medication order (if the doctor gives one).
Telephone
The sound of your voice and your manners are essential components of phone etiquette. Smile—the smile on your face comes through in your voice. Here are five more tips:
Get yourself organized before placing the call.
Minimize background noise.
Immediately identify yourself. Don’t assume the recipient will recognize your voice.
Concentrate on listening and avoid multitasking.
Schedule phone conversations to avoid playing phone tag.
Voice mail
Voice mail is an efficient way to communicate. Again, five tips:
Always be prepared to leave a message. Jot down your key message points before you call, to avoid stuttering and stammering.
Be concise and to the point.
State your name and the date, time, and purpose of your call.
Enunciate clearly and speak slowly.
State your name and phone number twice at the end of the message so the recipient doesn’t need to replay your message.
E-mail
In many business settings, e-mail has almost replaced letters and memos. In many cases, an e-mail is a recipient’s first impression of you, so follow these tips:
Make the subject line specific. This helps the reader prioritize the message and file it for easy retrieval.
Use a greeting and a close. It’s more polite and less impersonal.
Keep your message concise.
Keep your tone polite and businesslike.
Use your e-mail signature function, which provides several ways to contact you.
Text messages
This form of communication can be the most challenging and unpredictable. Some people send text messages routinely, while others may be unfamiliar with this method. You can’t go too far wrong if you take this advice:
Get to the point quickly. No one wants to read a long message on a mobile phone.
Don’t text during meetings. It’s rude to do so, and others can hear you clicking away or see the light from your screen.
Consider the recipient before using text abbreviations. Some people may not understand text lingo.
Consider the time when sending a text. Although you may be awake at 5 a.m., the sound of your incoming message might disturb a sleeping recipient.
Don’t expect an immediate response to your text. If the message is time sensitive, pick up the phone instead.
Improving the way we speak with managers and physicians can go a long way toward career advancement and professional satisfaction. Common courtesy is just as essential in e-mail, voice mail, and text messages as in face-to-face communication. When you follow the guidelines I’ve given, you’ll elevate your professional communications a few notches.
Selected references
Canfield J, Switzer J. The Success Principles: How to Get from Where You Are to Where You Want to Be. New York, NY: Morrow; 2006.
Kramer M, Schmalenberg, C. Confirmation of a healthy work environment. Crit Care Nurse. 2008 Apr;28(2):56-63.
Pagana K. The Nurse’s Communication Advantage: How Business Savvy Communication Can Advance Your Nursing Career. Indianapolis, IN: Sigma Theta Tau International; 2011.
Pagana K. The Nurse’s Etiquette Advantage: How Professional Etiquette Can Advance Your Nursing Career. Indianapolis, IN: Sigma Theta Tau International; 2008.
A keynote speaker, Kathleen D. Pagana is a professor emeritus at Lycoming College in Williamsport, Pennsylvania, and president of Pagana Keynotes and Presentations. She is the author of The Nurse’s Communication Advantage and The Nurse’s Etiquette Advantage. To contact her, visit www.KathleenPagana.com.
Here are resources that can help you in your busy clinical practice by giving you information quickly.
Pressure ulcer resources
Instead of searching through Google or another search engine for pressure ulcer resources, start with this comprehensive list on the Centers for Medicare & Medicaid Services website.
Examples of resources included are:
“Preventing pressure ulcers in hospitals: A toolkit for improving quality of care.” This toolkit from the Agency for Healthcare Research and Quality (AHRQ) is designed to help hospitals in implementing pressure ulcer prevention strategies.
“On-time pressure ulcer healing project.” Another AHRQ initiative, this resource is designed for those working in long-term care facilities.
“Pressure ulcer prevention.” This table from the Institute for Healthcare Improvement lists possible mentors you can work with in the area of ulcer prevention.
“Shawnee Medical Center wound care quick reference guide.” This is a handy one-page reference guide that includes photographs and recommendations.
“How-to guide: Prevent pressure ulcers—pediatric supplement.” This guide, tailored for pediatrics, describes key evidence-based care components for preventing pressure ulcers and describes how to implement these interventions.
You can also access case studies from a variety of facilities around the United States.
The National Lymphedema Network is a nonprofit organization founded in 1988 to provide education and other information to healthcare professionals and patients with lymphedema, as well as the general public. The site includes an explanation of lymphedema that may be helpful for you to use in teaching your patients. It also includes access to some of the articles from the newsletter LymphLink.
Many patients with chronic wounds have diabetes. To ensure those patients receive the best possible care, you can refer to the 2013 Standards of Medical Care in Diabetes from the American Diabetes Association, which were published in the January issue of Diabetes Care.
The journal provides a summary of the revisions and an executive summary of the standards related to each area, including diagnosis, testing, prevention, monitoring, and pharmacologic and nonpharmacologic management.
The guidelines include valuable information related to neuropathy screening and treatment and foot care. Recommendations for foot care include performing an annual comprehensive foot examination to identify risk factors predictive of ulcers and amputations. The foot examination should include inspection, assessment of foot pulses, and testing for loss of protective sensation.
Most of us have had days when we jump from meeting to meeting and at the end of the day wonder, “Did I get anything accomplished or am I more behind than ever?”
Many clinicians tell me that although their wound team meets regularly, the meetings aren’t meaningful enough, leaving the team still facing issues with their wound care program. As a consultant, when I review the wound team agenda, it’s typically missing one or more of four key ingredients:
appropriate member representation
proactive approach that highlights prevention
review of the plan of care and update of the medical record
review of supplies and products. Here’s a closer look at each of these ingredients.
Build a top team
Having the appropriate members on the wound care team is the first ingredient for success. A comprehensive, interdisciplinary team approach is the key to preventing skin breakdown and ensuring good clinical outcomes for residents with skin breakdown. Teams should include representation from nursing, dietary, and physical and occupational therapy, as well as a nurse practitioner or physician.
Nursing representation should include nurses from all three shifts and nursing assistants, who are too often missing from the team. Keep in mind that when it comes to preventing pressure ulcers, nursing assistants carry out most of interventions (for example, turning, incontinence management, heel lift). Even when a patient has a wound, the only intervention carried out by the nurses is the topical treatment; nursing assistants perform all other interventions necessary to ensure healing. Clinicians who empower nursing assistants to have a strong influence with the wound care team—and the program—tend to have very successful prevention programs and good clinical outcomes.
Think prevention
The second key ingredient is prevention. Most wound team meetings only discuss the patients with wounds, missing the bigger goal of preventing wounds in the first place. Once the patients with wounds are discussed, the team should review all high-risk patients to ensure proper preventative measures are in place and care planned. All patients should be quickly reviewed for evidence of:
decline or change in mobility and activity
new onset or change in continence status
decline in nutritional status
decline or change in cognition.
Any triggers in these areas should prompt a review of the plan of care to ensure they are being effectively addressed.
Review and update the plan
The third key ingredient for success is to use meeting time to review and update the plan of care. I’ve observed highly productive meetings and great discussions of the care the facility is providing. Then I review the medical record and discover that none of the interventions discussed are on the plan of care. Always review the patient’s plan of care to ensure it’s accurate, reflects all interventions, and is up to date. This will give you peace of mind that the medical record reflects all the good work you’re doing and helps make the team meetings feel productive.
Discuss products and supplies
The fourth key ingredient is to take the time to quickly discuss current wound care supplies and products with the team. Ask the team if the current supplies are user-friendly, are adequate, provide good outcomes, and are in good working condition.
Many times staff will not say how they’re struggling with, modifying, or not using something until they’re asked. Remember that the most expensive product is the one that doesn’t work or doesn’t get used.
A recipe for success
Using these four key ingredients will lead you to a successful wound team meeting—and a successful program. The mix may not solve your too-many-meetings days, but will give you peace of mind that at least one meeting is productive.
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has been specializing in wound prevention and management since 1990.
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)