BY: NANCY MORGAN, RN, BSN, MBA, WOCN, WCC, CWCMS, DWC
An essential part of weekly wound assessment is measuring the wound. It’s vitally important to use a consistent technique every time you measure. The most common type of measurement is linear measurement, also known as the “clock” method. In this technique, you measure the longest length, greatest width, and greatest depth of the wound, using the body as the face of an imaginary clock. Document the longest length using the face of the clock over the wound bed, and then measure the greatest width. On the feet, the heels are always at 12 o’clock and the toes are always 6 o’clock. Document all measurements in centimeters, as L x W x D. Remember—sometimes length is smaller than width. (more…)
Search Results for: wee
Think a Patient Has Rights? They Left.

by Dr. Michael Miller
There are few absolutes in my universe. I know that my youngest daughter will gleefully and with full malice (but humorously presented) find something to torment me about every time I see her; referrals from family practice docs arrive well marinated in multiple antibiotics with nary a diagnosis in sight (save for the ubiquitous “infection”); and that regardless of what I recommend, offer, beg, plead, or cajole, that the patient has the complete and total power to make their decisions regarding their care and who provides it. Unless they are deemed by multiple authorities to be incapable of making a decision, until the appropriate paperwork or an emergency situation exists mandating immediate lifesaving action, the ball bounces squarely in their court…or so I thought. (more…)
Read MoreHole-ier than Thou, Evidence Based Regardless of the Evidence

by Dr. Michael Miller
There are certain phrases that make the hair on the back of my neck stand up. Someone telling me that they are a good Jew, a good Christian, a good Muslim or the ultimate in self serving lies, “I ONLY practice EVIDENCE BASED MEDICINE”. People who are what they claim they are do not need to announce it. A short conversation, watching them work, others opinions about them all answer the question before it is asked. Like the RN who asked for a recent presentation on the true science behind NPWT (no, you don’t really understand it). She made sure to tell me not only that she practiced only EVIDENCE BASED MEDICINE but then gave me several examples which incidentally had absolutely no scientific evidence (save for articles from lots of dabblers doing lots of crazy things to people and writing about them). I am now awaiting her response as she may have to realize that her version of EVIDENCE BASED is no more real than Kim Kardashian’s celebrity. (more…)
Read MoreIf All You Have is a Hammer, What Happens When You Run Out of Nails?

by Dr. Michael Miller
Over the years of making house calls for wound care, I found that there was a real need for home based mental health and behavioral care, palliative care, podiatry and lots of other things. We cater to those who are home bound based on the classic definition involving the word “Taxing”. One of the more prevalent problems affecting all patients involves the nebulous but ubiquitous, nerve jangling, aptly named, “5th Vital Sign”, namely pain. As a part of my medical group, we have created a program that provides pain management not just to the home bound but all those whose lives and lifestyles are affected adversely by it. The program is a monument to government bureaucracy involving multiple layers of paperwork, mental health evaluations, testing of bodily fluids for both illegal and legal substances and then, the actual evaluation of the patient commences. After all hurdles are vetted and then jumped, then and only then does a prescription for the appropriate nostrum leave the pad. In wound care, we treat based on the etiology, the location, the related factors, the amounts of drainage, the surrounding tissues and so on, ad nauseum. Not surprisingly, in pain management, the scenario is much different. In wound care the mantra of the dabbler is see the hole, fill the hole. In pain management, the goal is to minimize pain to maximize functionality but the overriding questions are how this is accomplished. (more…)
Read MoreToolKit
- Alginate Dressing: download | 46KB
- Ankle Brachial Index: download | 50KB
- Diabetes Foot Examination: download |
- Debridement Tool: download | 125KB
- Job Task Analysis: download | 61KB
- Lanarkshire Oximetry Index: download | 172KB
- Plan-Do-Study-Act (PDSA) – Cycle Planning Sheet: download | 60KB
- PDSA Cycle Progress Sheet: download | 58KB
- PDSA Reporting Form: download | 60KB
- SBAR wound and skin provider communication record: download | 46KB
- Weekly Skin Assessment: download | 2MB
Wound care center honored

Even though the Advanced Wound Care Center at Cookeville Regional Medical Center only opened in the summer of 2015, the team already has exceeded clinical outcomes in 2016.
And it’s those numbers that got the center a Center of Distinction award.
“It’s impressive,” Scott Vinsant, area vice president of Healogics, said. “This shows clinical excellence.”
Healogics, based out of Jacksonville, Fla., is a provider of advanced wound care services and provides speciality wound care for an underserved and growing population. (more…)
Read MoreNYU docs use machine learning

Lymphedema causes unsightly swelling in the arms and legs. But researchers Mei Fu and Yao Wang have an idea for catching early symptoms sooner.
Researchers at NYU’s Tandon School of Engineering have teamed up with those from the university’s Rory Meyers College of Nursing to develop a machine-learning algorithm that could help detect a lymphatic system disease before doctors are able to.
There is no cure for lymphedema, only physical exercises that can keep the symptoms in check.
Early detection of the disease would allow for physical therapy that could theoretically stop the disease’s progress enough to never allow it to develop.
“Machine learning will help us to develop an algorithm to determine a patient’s status or predict if they will have a measurable symptom later on,” explained Mei Fu, an associate professor at NYU’s Rory Meyers College of Nursing, by telephone last week. “Each time the patients enter the data, the algorithm will teach itself. Later on, machine learning will probably help us say which treatment is better for which kind of patients.”
Read more at Technically Brooklyn
Read MoreManaging chronic venous leg ulcers — what’s the latest evidence?

Chronic venous leg ulcers (CVLUs) affect nearly 2.2 million Americans annually, including an estimated 3.6% of people over the age of 65. Given that CVLU risk increases with age, the global incidence is predicted to escalate dramatically because of the growing population of older adults. Annual CVLU treatment-related costs to the U.S. healthcare system alone are upwards of $3.5 billion, which are directly related to long healing times and recurrence rates of over 50%.
CVLUs are not only challenging and costly to treat, but the associated morbidity significantly reduces quality of life. That makes it critical for clinicians to choose evidence-based treatment strategies to achieve maximum healing outcomes and minimize recurrence rates of these common debilitating conditions. These strategies, which include compression therapy, specialized dressings, topical and oral medications, and surgery, are used to reduce edema, facilitate healing, and avert recurrence. (more…)
Read MoreReduction of 50% in Diabetic Foot Ulcers With Stem Cells

MUNICH — Local injection of mesenchymal stem cells derived from autologous bone marrow shows promise in healing recalcitrant neuropathic diabetic foot ulcers, a novel study from Egypt shows.
Presenting the results at the European Association for the Study of Diabetes (EASD) 2016 Annual Meeting, Ahmed Albehairy, MD, from Mansoura University, Egypt, said: “In patients who received the mesenchymal stem cells, ulcer reduction was found to be significantly higher compared with patients on conventional treatment after both 6 weeks and 12 weeks of follow-up. This is despite the fact that initial ulcer size was larger in the stem-cell–treated group.” (more…)
Read MoreUsing fat to help wounds heal without scars
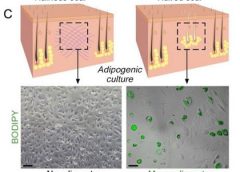
Philadelphia – Doctors have found a way to manipulate wounds to heal as regenerated skin rather than scar tissue. The method involves transforming the most common type of cells found in wounds into fat cells – something that was previously thought to be impossible in humans. Researchers began this work at the Perelman School of Medicine at the University of Pennsylvania, which led to a large-scale, multi-year study in connection with the Plikus Laboratory for Developmental and Regenerative Biology at the University of California, Irvine. They published their findings online in the journal Science on Thursday, January 5th, 2017.Fat cells called adipocytes are normally found in the skin, but they’re lost when wounds heal as scars. The most common cells found in healing wounds are myofibroblasts, which were thought to only form a scar. Scar tissue also does not have any hair follicles associated with it, which is another factor that gives it an abnormal appearance from the rest of the skin. Researchers used these characteristics as the basis for their work – changing the already present myofibroblasts into fat cells that do not cause scarring. (more…)
Read MoreSkin substitutes: Understanding product differences
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make.
Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled procedures and herbal treatments to heal wounds, including xenografts (skin from another species). The practice of applying allografts (human cadaver skin) to wounds was first documented in 1503. In 1871, autologous skin grafting (skin harvested from the the person with the wound) was tried. Next came epithelial- cell seeding, which involves scraping off the superficial epithelium of healthy skin and transplanting the cells onto the wound. (more…)
Read MoreFrequently asked questions about support surfaces

The National Pressure Ulcer Advisory Panel (NPUAP) describes support surfaces as “specialized devices for pressure redistribution designed for management of tissue loads, microclimate, and/or other therapeutic functions.” These devices include specialized mattresses, mattress overlays, chair cushions, and pads used on transport stretchers, operating room (OR) tables, examination or procedure tables, and gurneys. Some support surfaces are part of an integrated bed system, which combines the bed frame and support surface into a single unit. (more…)
Read More