The first 24 hours after a patient’s admission are critical in preventing pressure ulcer development or preventing an existing ulcer from worsening. A skin inspection, risk assessment, and temporary care plan should all be implemented during this time frame. Essentially, it’s the burden of the care setting to prove to insurers, regulators, and attorneys the pressure ulcer was present on admission and interventions were put into place to avoid worsening of the condition. Of course, patients also benefit from having their condition identified and treated promptly. (more…)
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC
About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders.
A stoma has no sensory nerve endings and is insensitive to pain. Yet several complications can affect it, making accurate assessment crucial. These complications may occur during the immediate postoperative period, within 30 days after surgery, or later. Lifelong assessment by a healthcare provider with knowledge of ostomy surgeries and complications is important. (more…)
At some point, most of us have encountered a bully—most commonly when we were kids. You might think that as we get older, bullying wouldn’t be a problem we have to deal with. Unfortunately, that’s not the case. In the healthcare field, bullying can be even worse than it was when we were children.
Bullying in health care takes many different forms, including fighting among different types of clinicians, managers bullying subordinates, peer-to-peer bullying and, most commonly, specialists bullying other specialists. Years ago when I realized my dream of becoming a wound care specialist, I thought other specialists would be relieved I was on board to help with the overwhelming task of spreading wound care knowledge and healing wounds. But I found out quickly that I was pretty much alone with those thoughts, and my first encounter with wound care bullies occurred.
I began to ask myself: What did I do wrong? Why are they slamming me? What did I do to them? They don’t even know me; they’ve never even talked to me. This may sound familiar to many of you, whether you’re a wound care specialist, an ostomy specialist, or a diabetes or lymphedema specialist.
Workplace bullying is defined as repeated, unreasonable actions by individuals (or a group) directed toward an employee (or group of employees) that are intended to intimidate, degrade, humiliate, or undermine. Bullying occurs for many reasons; these reasons almost always include insecurity, competition, and the desire to feel more powerful and be in control.
So how do we deal with the bullies?
• Follow the Golden Rule: Treat others as you’d like others to treat you. Don’t stoop to the bully’s level.
• Stay calm and rational. Don’t get emotional. Bullies take pleasure in manipulating people emotionally.
• Don’t lose your confidence or blame yourself. Recognize that this isn’t about you; it’s about the bully. Be proud and confident in your certification credential.
• Focus on your purpose—to provide safe, competent, high-quality care to every patient.
• Document the bullying incident. Start a diary detailing the nature of the bullying, including dates, times, places, what was said or done, and who was present. Start a file with copies of anything in print that shows harassment and bullying; hold onto copies of documents that contradict the bully’s accusations against you.
• If the bullying behavior compromises patient safety and care, report the bully.
Stopping all bullying in health care may seem like an insurmountable goal, but I believe that together we can try to stop the bullying cycle in our specialty. By setting the example and supporting each other, we can turn the focus back to healing and caring for our patients as a team, not as one practitioner against the world.
Actions speak louder than words. As Ralph Waldo Emerson said, “What you do speaks so loudly that I cannot hear what you say.”
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
By Rosalyn Jordan, RN, BSN, MSc, CWOCN, WCC, and Marci Christian, BBE
Any patient with a fecal or urinary ostomy may experience complications on the skin surface around the stoma. These complications may occur lifelong, although they’re more common during the first 5 years after the initial ostomy surgery. Causative factors include infection, trauma, certain diseases, and chemical irritation; most of these problems stem from the pouching system or pouch leakage.
Peristomal skin complications can cause a wide range of signs and symptoms, from skin discoloration to polyp-like growths, from erythema to full-thickness wounds. They can lead to discomfort, pain, poor self-image, social isolation, and impaired quality of life, not to mention additional care costs.
Incidence and types of these complications are hard to compare or contrast across multiple patients. Until recently, no standardized assessment or documentation tools were available to characterize or define complications. For this reason, reported rates ranged widely, from 10% to 70%. And because no designated common language or categories related to peristomal skin complications existed, documentation was inconsistent.
In the late 2000s, a group of nurses experienced in caring for ostomy patients worked with the World Council of Enterostomal Therapists to develop a resource called the Ostomy Skin Tool, which clinicians can use to categorize and describe peristomal skin complications in a consistent, objective manner. The tool also provides a common language for documentation.
The Ostomy Skin Tool has three major assessment domains—discoloration (D), erosion/ulceration (E), and tissue overgrowth (T), known collectively as DET. The DET combined rating ranges from normal, rated 0, to the worst condition possible, rated 15. Mild DET complications are documented as less than 4, moderate as less than 7, and severe as 8 or higher. (See Using the Ostomy Skin Tool by clicking the PDF icon above.)
The tool describes four categories of peristomal complications:
• chemical irritation
• mechanical trauma
• disease-related complications
• infection-related complications.
Chemical irritation
Chemical irritation can stem from irritants (as in contact dermatitis) or allergic reactions (allergic dermatitis). The most likely cause of chemical dermatitis is effluent leakage (feces or urine) from the colostomy, ileostomy, or urostomy, in which effluent comes in contact with peristomal skin. Other potential causes include contact with soap, certain adhesives, and adhesive removers.
The major treatment of chemical irritation is identification and removal of the offending agent, followed by patient and caregiver education on the new pouching procedure the patient must use. Follow-up assessment also is recommended. In a 2010 study that followed 89 patients for 1 year after ostomy surgery, about 50% of subjects experienced peristomal skin complications, most of them from pouch leakage. Another investigator estimated that 85% of ostomy patients experience pouch leakage at some time during their lives. Pouch leakage usually occurs when stool is extremely liquid (for instance, ileostomy effluent). Other causes of pouch leakage include wearing a pouch more than half full of effluent and abdominal contours that aren’t level. Besides changes in the pouching system, treatment may entail adding products to the pouching system or removing certain agents.
Some patients experience allergic dermatitis in reaction to products used in the pouching system (such as skin barriers, belts, pouch closures, or adhesives). However, allergic dermatitis is rare. One 2010 study suggested allergic reactions to these products occur in only about 0.6% of patients with peristomal skin irritation. Most major ostomy product manufacturers provide a patch test on request to help identify allergic conditions. Once the offending product is discontinued, allergic dermatitis should resolve rapidly.
Mechanical trauma
Mechanical trauma usually results from either the pouching system itself or its removal. It also may result from harsh or multiple skin-barrier removals, pressure from convex rings or pouches, and abrasive cleansing techniques. Some researchers believe the stronger the adhesive barrier and the more often a pouch is changed, the greater the risk of epidermal damage.
Mechanical trauma may present as a partial-thickness ulcer caused by pressure, shear, friction, tearing, or skin stripping. Patients with fragile skin are susceptible to mechanical trauma, so less aggressive pouching systems may be preferred for them. Of course, if the pouching system is changed, the patient or caregiver needs to learn about the new system.
Disease-related complications
Disease-related peristomal complications may be linked to preexisting skin conditions, such as psoriasis, eczema (atopic dermatitis), or seborrheic dermatitis. Hyperplasia also may occur. This overgrowth of cells, which may appear as gray or reddish brown pseudoverrucous lesions, usually is linked to urinary ostomies, although it can occur with fecal ostomies as well. Vinegar soaks are the recommended treatment, in addition to a change in the pouching system and corresponding patient education.
Occasionally, other disease-related complications occur, including primary adenocarcinoma of the peristomal skin and peristomal pyoderma gangrenosum, a painful and problematic condition that presents as peristomal ulcers. Ulcer borders are well-defined with a bluish purple coloration at the edges. Infection must be ruled out, as this condition usually is linked to an autoimmune condition. Treatment includes pain management and, in most cases, a topical corticosteroid. Crohn’s disease also may manifest as a peristomal skin ulcer.
Infection-related complications
Infection-related complications may be bacterial or fungal. Two common peristomal skin infections are folliculitis and Candida fungal infections. An infection of the hair follicle that causes pustules, folliculitis usually stems from traumatic hair pulling in the peristomal area during pouch removal. It may warrant a prescribed antibiotic, along with patient teaching regarding proper hair removal using an electric razor.
Candida infections may arise because peristomal skin provides a warm, dark, moist environment that promotes fungal growth. These infections appear as erythema with pustules or papules and satellite lesions. Treatment usually involves antifungal powder and use of the crusting technique to secure the pouching system. (See Using the crusting technique by clicking the PDF icon above.)
Management
Many complications are well advanced by the time patients seek assistance, perhaps because they don’t understand the significance of their symptoms and think they can manage the problem themselves. In some cases, they don’t know where to turn for assistance. Commonly, the complication progresses to the point where the patient goes to the emergency department or (particularly during the immediate postoperative period) needs to be readmitted for treatment. The best way to manage peristomal skin complications is to prevent them in the first place. (See Preventing peristomal skin complications by clicking the PDF icon above.)
Patient education
Over the past 20 years, hospital stays for ostomy surgery patients have decreased from about 2 weeks to less than 5 days. Reduced stays decrease the time available for caregivers to teach patients and family members how to empty and change the pouch. They need alternative education covering (among other topics) how to recognize peristomal skin complications and when to seek help. Not only do these complications require vigilant self-observation, but many patients don’t understand their implications or how rapidly they can worsen. In some cases, the first symptoms are itching and redness under the skin barrier. Fortunately, some patients may know or remember that itching, burning, stinging, reddened, or weeping peristomal skin requires professional attention. They can avoid serious complications by seeking assistance early, such as right after noticing pouch leakage.
Early treatment can reduce the cost of treatment. In a 2012 study, researchers estimated care costs related to peristomal skin complications for a 7-week treatment period, using the Ostomy Skin Tool as a reference. Severe complications (those with a DET score above 8) cost six times more to treat than mild cases (those with a DET score below 4) and 4.5 times more than moderate cases.
Along with early intervention by a trained ostomy care specialist, self-assessment by ostomy patients promotes a better quality of life, reduces pain, and may decrease care costs. Clinicians’ use of the Ostomy Skin Tool to assess and document peristomal skin complications promotes more reliable, objective, comparable assessment data for reporting.
Selected references
Al-Niaimi F, Lyon CC. Primary adenocarcinoma in peristomal skin: a case study. Ostomy Wound Manage. 2010;56(1):45-7.
Burch J. Management of stoma complications. Nurs Times. 2011;107(45):17-8, 20.
Jemec GB, Martins L, Claessens I, et al. Assessing peristomal skin changes in ostomy patients: validation of the Ostomy Skin Tool. Br J Dermatol. 2011; 164;330-5.
Jones T, Springfield T, Brudwick M, Ladd A. Fecal ostomies: practical management for the home health clinician. Home Healthc Nurse. 2011;29(5):306-17.
Martins L, Samai O, Fernandez A, et al. Maintaining healthy skin around an ostomy: peristomal skin disorders and self-assessment. Gastrointest Nurs. 2011;
9(2):9-13.
Martins L, Tavernelli K, Serrano JLC. Introducing a peristomal skin assessment tool: The Ostomy Skin Tool. World Council Enterostomal Therapists J. 2008;28(2):3-13.
Meisner S, Lehur P, Moran B, et al. Peristomal skin complications are common, expensive, and difficult to manage: a population based cost modeling study. PLoS One. 2012;7(5):e37813.
Omura Y, Yamabe M, Anazawa S. Peristomal skin disorders in patients with intestinal and urinary ostomies: influence of adhesive forces of various hydrocolloid wafer skin barriers. J Wound Ostomy Continence Nurs. 2010;37(3):289-98.
Ratliff CR. Early peristomal skin complications reported by WOC nurses. J Wound Ostomy Continence Nurs. 2010;37(5):505-10.
Shabbir J, Britton DC. Stomal complications: a literature overview. Colorectal Dis. 2010;12(10):958- 64.
Wound, Ostomy, Continence Clinical Practice Ostomy Subcommittee. Peristomal skin complications: Best practice for clinicians. Mt. Laurel, NJ; 2007.
The authors work for RecoverCare, LLC, in Louisville, Kentucky. Rosalyn Jordan is director of clinical education and Marci Christian is a clinical associate product specialist.
In most cases, amputation (removal of an extremity, digit, or other body part) is a surgical intervention performed to remove tissue affected by a disease and, in some cases, to provide pain relief. Fecal and urinary diversion surgeries also are considered amputations. Amputations and fecal or urinary diversions (ostomies) require extensive rehabilitation and adaptation to a new way of life, with physiologic and psychological impacts. Although diversions and ostomies usually are less visible to others than other types of amputations, they call for similar patient education, rehabilitatio n, and lifelong counseling.
The primary goal of therapy for ostomates and amputees is to resume their presurgical lifestyle to the greatest extent possible and to adapt to their new circumstances. Preoperative assessment and training interventions have proven valuable. Having a clear understanding of the surgical intervention helps reduce postoperative anxiety and depression, which can pose roadblocks to patients’ adaptation or response to their new situation. Successful interventions should be done by healthcare professionals who are trained in caring for ostomates and amputees.
Ostomates and amputees experience similar psychosocial challenges, body-
image problems, and sexuality concerns. This article focuses on these three issues. For a summary of other issues these patients may experience, see Other problems amputees and ostomates may face by clicking the PDF icon above.
Psychosocial challenges
Ostomates and amputees may experience depression, anxiety, fear, and many other concerns related to the surgical procedure—concerns that center on whether they’ll be able to resume their presurgical lifestyle. Many worry about social isolation and loss of income. Some fear both the primary disease process and the lifestyle changes induced by surgery. Anxiety may impede their social interactions and lead to significant psychological problems. Appropriate and effective counseling and therapy must be planned and provided. (But be aware that untrained or inexperienced healthcare professionals may not be able to provide the guidance the patient needs to feel comfortable; some may be unable even to offer information about available support systems.)
These patients also may find themselves socially isolated, in part due to loss of employment or the socioeconomic consequences of a decreased income. Some experience fear and worry when anticipating lifestyle changes caused by loss in or change of function, adaptation to the prosthesis, and treatment costs.
Maintaining social contact after surgery is extremely important to recovery and adaptation to the amputation or ostomy. The United Ostomy Associations of America and the Amputee Coalition encourage patients to maintain social involvement. Both groups suggest patients discuss their feelings, thoughts, and fears with a trusted family member, friend, or partner. Both organizations sponsor and encourage support-group involvement. In some cases, emotional support from other amputees or ostomates with a similar experience may be appropriate; some patients may be more comfortable sharing thoughts and asking questions in a group of people with similar experiences. Resuming presurgical social events and activities can enhance patients’ adaptation to a new way of life.
Ostomates and amputees have to cope not only with changes in physical appearance but with how their body functions and how they feel and perceive their body. They’re keenly aware of their changed appearance and are concerned about others’ perceptions of them. They may feel anxious and depressed related to body image; the degree of anxiety and depression may relate directly to their presurgical body image and activities. Many become anxious and fearful as they adapt to the prosthesis. (See Stages of grief by clicking the PDF icon above.)
Compared to amputees, ostomates may have more concerns about body image with sexual partners, because the stoma is, in a sense, a hidden amputation. In most cases, the stoma and pouch can be obscured visually from others. The amputee, on the other hand, has fewer options for hiding the missing body part.
To help patients cope with body-image problems, care providers must offer education, therapy, and counseling to help the patient accept and successfully adapt to the body-image change. The first step in this process may simply be to have the patient look at the stoma or stump, progressing to participation in prosthesis care.
Sexuality concerns
Many ostomates and amputees have difficulty resuming sexual activity after surgery. Although the stoma usually remains hidden from others, it’s observable to the ostomate and sex partner. Most patients require an adjustment period before they feel comfortable with a sex partner. They may fear that:
• the partner will reject them or no longer find them attractive
• they will experience loss of function and sensation
• they will experience pain or injury of the stoma.
They also may feel embarrassed, causing them to avoid sex. However, counselors can help couples discuss these concerns and resume a satisfactory sexual relationship. Ostomates and amputees and their partners may need counseling to resume a satisfactory sexual relationship. If they continue to have adjustment difficulties, referral to a trained sex counselor or psychologist may be indicated. Several studies show that appropriate counseling can help prevent complications and allow amputees and ostomates to continue to express their affection physically. (See Talking to patients about sexual problems by clicking the PDF icon above.)
Resuming sexual activity may be easier if the ostomate or amputee had a sex partner before surgery. However, males who experience postsurgical erectile dysfunction are less likely than other males to resume sexual activity. Counseling encourages postsurgical patients to focus more on the pleasurable feelings they and their partners feel, rather than on sexual performance. Body-image problems and inadequate sexual adjustment go hand in hand. (See Helping ostomates resume sex by clicking the PDF icon above.)
Team approach to patient education and counseling
In many parts of the country, a designated healthcare team manages amputees’ care and rehabilitation. But until recently, nurses were the only professionals certified to participate in ostomates’ care and rehabilitation. In fact, ostomates may represent a significant underserved population. A 2012 study found many ostomy patients didn’t receive consistent training and counseling from ostomy certified nurses. Only 13% of respondents reported they had regular visits with an ostomy certified nurse; 32% said they’d never received care from an ostomy nurse. Just over half (56%) indicated they saw an ostomy nurse when they thought it was necessary. The study also reported that 57% hadn’t seen an ostomy certified nurse in more than 1 year.
A team with specialized training to address ostomates’ physical and psychosocial needs might be able to provide the specialized care these patients need. The primary medical caregiver or general practitioner would serve as team leader and make appropriate referrals. The team should include a surgeon, ostomy- and amputee-trained nurses, a prosthetist or other healthcare provider trained in selection and fitting of prosthetic equipment and devices that affect function, a physical therapist, an occupational therapist, a social worker, a vocational counselor, a psychologist, caregiver or family members, support groups, and (last but not least) the patient.
The team approach might reduce hospital stays and promote patients’ return to their home environment. It also might encourage independence and enhance the success of long-term adaptation.
Focus on the future
Healthcare providers should encourage ostomates and amputees to focus on the future, not the past. Feeling comfortable with the prosthesis—the amputee’s artificial limb or the ostomate’s pouching system—is essential to adapting to a “new normal” way of life. Maintaining social relationships is important to adaptation as well. Mastering basic skills and adapting to changes in body function help improve the patient’s quality of life. Follow-up visits, phone contact, and access to a team of well-trained healthcare providers for patient education, rehabilitation, and long-term management are crucial to these patients’ successful adaptation and quality of life.
Selected references
Bhuvaneswar CG, Epstein LA, Stern TA. Reactions to amputation: recognition and treatment. Prim Care Companion J Clin Psychiatry. 2007;9(4):303-8.
Davidson T, Laberge M. Amputation. Gale Encyclopedia of Surgery: A Guide for Patients and Caregivers. 2004. www.encyclopedia.com/doc/1G2-3406200023.html. Accessed December 20, 2012.
Erwin-Toth P, Thompson SJ, Davis JS. Factors impacting the quality of life of people with an ostomy in North America: results from the Dialogue Study. J Wound Ostomy Continence Nurs. 2012;39(4):417-22.
Maguire P, Parkes CM. Surgery and loss of body parts. BMJ. 1998;316(7137):1086-8.
Pittman J, Kozell K, Gray M. Should WOC nurses measure health-related quality of life in patients undergoing intestinal ostomy surgery? J Wound Ostomy Continence Nurs. 2009;36(3):254- 65.
Pittman J. Characteristics of the patient with an ostomy. J Wound Ostomy Continence Nurs. 2011;38(3):271-9.
Racy JC. Psychological adaptation to amputation. In Bowker JH, Michael JW, ed. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2nd ed. Rosemont, IL: American Academy of Orthopedic Surgeons; 1998.
Tunn PU, Pomraenke D, Goerling U, Hohenberger P. Functional outcome after endoprosthetic limb-salvage therapy of primary bone tumours—a comparative analysis using the MSTS score, the TESS and the RNL index. Int Orthop. 2008;32(5):619-25.
Turnbull G. Intimacy After Ostomy Surgery Guide. United Ostomy Associations of America, Inc. Revised 2009. www.ostomy.org. Accessed December 20, 2012.
Turnbull G. Sexuality after ostomy surgery. Ostomy Wound Manage. 2006;52(3):14,16.
Lymphedema is characterized by regional immune dysfunction, distorted limb contours, and such skin changes as papillomas, hyperkeratosis, and increased girth. The condition may involve the limbs, face, neck, trunk, and external genitals; its effects may include psychological distress. For optimal patient management, clinicians must understand what causes lymphedema and how it’s diagnosed and treated.
This two-part series provides an overview of lymphedema. Part 1 covers etiology, pathology, and diagnosis. Part 2, which will appear in the November-
December issue, will focus on treatment.
Causes of lymphedema
Lymphedema occurs when protein-rich fluid accumulates in the interstitium due to impaired lymphatic function. Proteins, other macromolecular wastes, and water constitute lymphatic loads. These wastes rely on specially structured absorptive and transport structures in peripheral regions for their return to central circulation.
When lymph stasis prevails, inflammatory processes and lymphostatic fibrosis trigger tissue-density changes, further entrapping superficial vessels and accelerating mechanical insufficiency. (See Physiologic changes caused by lymphatic disruption by clicking the PDF icon above.)
Classifying lymphedema
Lymphedema can be primary or secondary. Primary lymphedema either is congenital (present at birth) or arises around puberty. In the vast majority of cases, it is associated with structural changes in the lymphatic system and isn’t associated with another disease or condition. Most structural changes (87%) manifest before age 35 and cause hypoplasia of vessels and nodes. Syndromes involving hyperplasia, node fibrosis, or aplasia also may occur, although they’re much less common. Dysplasia (either hypoplasia, hyperplasia, or aplasia) predisposes drainage regions to inadequate lymph collection, resulting in edema and secondary tissue changes, such as chronic inflammation and reactive fibrosis. Genetic variability in lymphatic constitution may explain why seemingly similar patients receiving the same surgical protocol have different lymphedema risks over time. Secondary lymphedema stems from a significant insult to lymphatic tissues, as from lymphadenectomy, radiation therapy, trauma, infection, or cancer. It commonly results from direct trauma to regional nodes or vessel structures. Slow degradation of lymphatic function also occurs when adjacent tissues (such as superficial and deep veins) become diseased, when cellulitis occurs, or when accumulations
of adipose or radiation fibrosis mechanical-ly disrupt drainage of skin lymphatics.
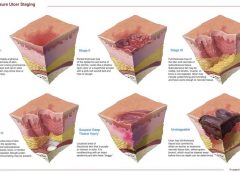
Lymphedema stages
Lymphedema progresses in stages, which involve secondary connective-tissue disease combined with disturbed fluid update and transport. These conditions cause a universal and classic clinical picture.
• Stage 0 (latency stage) is marked by reduced transport capacity and functional reserve. The patient has no visible or palpable edema, but has such subjective complaints as heaviness, tightness, and waterlogged sensations.
• In Stage 1 edema (reversible lymphedema), edema decreases with elevation. Pitting edema is present, but fibrosis is absent.
• During Stage 2 (spontaneously irreversible lymphedema), lymphedema doesn’t resolve entirely, although it may fluctuate. Pitting is more pronounced and fibrosis is present.
• Stage 3 (lymphostatic elephantiasis) is marked by dermal hardening, nonpitting edema, papillomas, hyperkeratosis, and in some cases, extreme girth.
Assessment and diagnosis
Diagnosing lymphedema can be challenging because edema may be associated with other diseases and disorders. For a summary of signs and symptoms, see Clinical findings in lymphedema by clicking the PDF icon above.
Discomfort and skin appearance
Lymphedema rarely causes pain because the skin accommodates gradual, insidious fluid accumulation. However, secondary orthopedic discomfort may result from increased weight of the affected limb due to deconditioning or decreased range of motion.
Because lymphedema usually progresses slowly, gravity and centrifugal forces pull fluids toward distal limb areas, causing an entrenched, stubborn pitting edema. Later, further valvular incompetence contributes to worsening distal edema in the fingers, toes, and dorsal regions of the hand and foot. Prominent lower-extremity structures, such as the malleolus, patella, tibia, anterior tibialis tendon, and Achilles tendon, become progressively less distinct. This creates a columnar limb appearance; the swollen limb has the same girth from distal to proximal aspects, unlike the natural cone shape of a normal limb.
Lymphatic failure doesn’t tax the venous system, so skin color remains normal. Blood supply remains patent, helping to prevent secondary ulcers.
Severity
Lymphedema severity correlates directly with such factors as onset of the condition and extent of cancer therapy, if given (number of nodes resected, number of positive nodes, and use of radiotherapy). Lymphedema may worsen with a greater number of infection episodes, weight gain, injury, diuretics, limb disuse, pneumatic compression therapy (when used for pure lymphedema), and ill-fitting compression garments. The single most important contributor to increasing lymphedema severity is lack of patient education, which can result in improper treatment or none at all.
Opportunistic infections
Lymphedema causes regional immune suppression and leads to an increase in opportunistic infections such as cellulitis. As skin integrity suffers, scaling and dryness allow resident skin pathogens (such as streptococci and staphylococci) to gain access through the defective skin barrier into protein-rich interstitial fluid, creating a medium favorable to bacterial colonization. Lymphocyte migration decreases, and dissected or irradiated nodal sites are slow to detect invaders. Furthermore, stagnant lymph promotes further delays in the immune response. Patients with opportunistic infections may exhibit high fever, local erythema, regional hypersensitivity or acute pain, flulike symptoms, and rapidly advancing “map-like” borders in the skin.
Differential diagnosis
Several methods can aid differential diagnosis. Clinical findings. Lymphedema can be diagnosed from patient history, physical examination, palpation, and inspection. Trauma to lymph nodes (each of which governs a distinct body region) decreases the transport capacity of lymph formed in that region, in turn causing local swelling (lymphedema). Trauma to the axillary or inguinal lymph nodes, which exist on both the left and right of the body and in both the upper and lower regions, predisposes these quadrants to swelling. Therefore, if lymph nodes on only one side are damaged, lymphedema occurs only on that side of the body. Using the universal characteristics cited above as a guide, while ruling out cancer recurrence, acute deep vein thrombosis, or plasma protein abnormalities, yields sufficient data to form a diagnosis. Imaging. Lymphography involves subcutaneous injection of a lymph vessel–
specific dye (Patent Blue V), followed by X-ray. Although it provides high-resolution images of lymphatic structures, this technique is invasive, painful, damaging to lymphatics, and potentially lethal—and therefore is no longer recommended.
Lymphangioscintigraphy (LAS) uses interdigital subcutaneous injection of protein-labeled radioisotopes, followed by
imaging at specific intervals to gather information about uptake and transport time. Images are hazy and false-negatives are common, so well-trained radiotherapists familiar with lymphology and lymphedema should administer and interpret the test. Also, experts don’t agree on standard criteria for LAS administration, so measures may not be similarly conclusive. Limb-measuring instruments and methods. Serial measurement of affected limb circumference using a standard garment tape measure is the most widely accessible approach. Intra-rater reliability is comparable to that of currently used tools; however, these methods can’t be used for early detection, for screening, or when various raters are used to assess the same patient. Circumferences are measured at four points and are considered positive if a distance of 2 cm or more separates the involved from uninvolved extremity in comparison. Water displacement techniques for limb-volume calculation, although accurate, are impractical in most clinical settings and rarely used.
Various devices have been used to obtain measurements. For instance, the Perometer® uses optoelectronic volumetry. By scanning the limb with infrared beams circumferentially, the device accurately records girth at 4-mm intervals along the limb length and transmits these measurements to a computer. The Perometer is used mainly in the research setting. Preoperative and postoperative measurements at intervals can detect lymphedema early.
Impedimed XCA® uses bioelectrical
impedance to calculate ratios of intracellular to extracellular fluid. A weak electrical current is passed through affected and unaffected limbs, allowing comparison of results. Impedance is lower in edematous tissue, supporting an accurate diagnosis.
Next step: Treatment
Once a diagnosis is made, the next step is treatment. Part 2 of this series covers lymphedema treatment.
Selected references
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
Kubik S, Manestar M. Anatomy of the lymph capillaries and precollectors of the skin. In: Bollinger A, Partsch H, Wolfe JHN, eds. The Initial Lymphatics. Stuttgart: Thieme-Verlag; 1985:66-74.
Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)—2009. Int Angiol. 2010 Oct;29(5):454-70.
Lerner R. Chronic lymphedema. In: Prasad H, Olsen ER, Sumpio BE, Chang JB, eds. Textbook of Angiology. Springer; 2000.
Mayrovitz HN. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology. 2009 June;42(2):88-98
Pecking AP, Alberini JL, Wartski M, et al. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008 Mar;41(1):1-10.
Stanton AW, Northfield JW, Holroyd, B, et al. Validation of an optoelectronic volumeter (Perometer). Lymphology. 1997 June;30(2):77-97
Weissleder H, Schuchhardt C. Lymphedema: Diagnosis and Therapy. 4th ed. Viavital Verlag GmbH; 2007.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Starting your own consulting business is an exciting and rewarding experience: You’re the boss; you’re in charge. The question is, do you have what it takes? Along with the excitement of being the boss comes the responsibility of decisions and commitment. Your decisions will affect whether the business is a failure or a success.
To succeed in consulting, you must be an expert at recognizing problems and shaping solutions to those problems, and you must possess excellent time-management and networking skills. If you think you have what it takes to be a consultant, read on. This article gives an overview of the process.
Nature of the business
Businesses hire consultants for their expertise to help them identify problems, supplement staff, institute change, provide an objective viewpoint, or teach.
Examples of specific services you can offer include single patient reviews, serving as a member of the wound care team, making wound rounds on all patients, providing education, patient teaching, protocol development, and troubleshooting. These services are provided in many settings—long-term care, home care, long-term acute care, rehabilitation hospitals, acute-care hospitals, insurance companies, and primary-care provider groups. (more…)
Hansen’s disease, also called leprosy, is treatable today – and that’s partly thanks to a curious tree and the work of a pioneering young scientist in the 1920s. Centuries prior to her discovery, sufferers had no remedy for leprosy’s debilitating symptoms or its social stigma.
This young scientist, Alice Ball, laid fundamental groundwork for the first effective leprosy treatment globally. But her legacy still prompts conversations about the marginalization of women and people of color in science today.
Alice Augusta Ball, born in Seattle, Washington, in 1892, became the first woman and first African American to earn a master’s degree in science from the College of Hawaii in 1915, after completing her studies in pharmaceutical chemistry the year prior.
After she finished her master’s degree, the college hired her as a research chemist and instructor, and she became the first African American with that title in the chemistry department.
Doctors now understand that leprosy, also called Hansen’s disease, is minimally contagious. But in 1865, the fear and stigma associated with leprosy led authorities in Hawaii to implement a mandatory segregation policy, which ultimately isolated those with the disease on a remote peninsula on the island of Molokai. In 1910, over 600 leprosy sufferers were living in Molokai.
Doctors had attempted to use nearly every remedy imaginable to treat leprosy, even experimenting with dangerous substances such as arsenicand strychnine. But the lone consistently effective treatment was chaulmoogra oil.
Chaulmoogra oil is derived from the seeds of the chaulmoogra tree. Health practitioners in India and Burma had been using this oil for centuries as a treatment for various skin diseases. But there were limitations with the treatment, and it had only marginal effects on leprosy.
The oil is very thick and sticky, which makes it hard to rub into the skin. The drug is also notoriously bitter, and patients who ingested it would often start vomiting. Some physicians experimented with injections of the oil, but this produced painful pustules.
Dr. Isabel Kerr, a European missionary, administering to a patient a chaulmoogra oil treatment in 1915, prior to the invention of the Ball Method. George McGlashan Kerr, CC BY
The Ball Method
If researchers could harness chaulmoogra’s curative potential without the nasty side effects, the tree’s seeds could revolutionize leprosy treatment. So, Hollmann turned to Ball. In a 1922 article, Hollmann documents how the 23-year-old Ball discovered how to chemically adapt chaulmoogra into an injection that had none of the side effects.
The Ball Method, as Hollmann called her discovery, transformed chaulmoogra oil into the most effective treatment for leprosy until the introduction of sulfones in the late 1940s.
In 1920, the Ball Method successfully treated 78 patients in Honolulu. A year later, it treated 94 more, with the Public Health Service noting that the morale of all the patients drastically improved. For the first time, there was hope for a cure.
Ball’s death meant she didn’t have the opportunity to publish her research. Arthur Dean, chair of the College of Hawaii’s chemistry department, took over the project.
Dean mass-produced the treatment and published a series of articles on chaulmoogra oil. He renamed Ball’s method the “Dean Method,” and he never credited Ball for her work.
Ball’s other colleagues did attempt to protect Ball’s legacy. A 1920 article in the Journal of the American Medical Association praises the Ball Method, while Hollmann clearly credits Ball in his own 1922 article.
Ball is described at length in a 1922 article in volume 15, issue 5, of Current History, an academic publication on international affairs. That feature is excerpted in a June 1941 issue of Carter G. Woodson’s “Negro History Bulletin,” referring to Ball’s achievement and untimely death.
Joseph Dutton, a well-regarded religious volunteer at the leprosy settlements on Molokai, further referenced Ball’s work in a 1932 memoir broadly published for a popular audience.
Historians such as Paul Wermager later prompted a modern reckoning with Ball’s poor treatment by Dean and others, ensuring that Ball received proper credit for her work. Following Wermager’s and others’ work, the University of Hawaii honored Ball in 2000 with a bronze plaque, affixed to the last remaining chaulmoogra tree on campus.
In 2019, the London School of Hygiene and Tropical Medicine added Ball’s name to the outside of its building. Ball’s story was even featured in a 2020 short film, “The Ball Method.”
The Ball Method represents both a scientific achievement and a history of marginalization. A young woman of color pioneered a medical treatment for a highly stigmatizing disease that disproportionately affected an already disenfranchised Indigenous population.
In 2022, then-Gov. David Ige declared Feb. 28 Alice Augusta Ball Day in Hawaii. It was only fitting that the ceremony took place on the Mānoa campus in the shade of the chaulmoogra tree.
The word “leprosy” conjures images of biblical plagues, but the disease is still with us today. Caused by infectious bacteria, some 200,000 new cases are reported each year, according to the World Health Organization. In the United States, leprosy has been entrenched for more than a century in parts of the South where people came into contact with armadillos, the principle proven linkage from animal to humans. However, the more recent outbreaks in the Southeast, especially Florida, have not been associated with animal exposure.
The Conversation talked with Robert A. Schwartz, professor and head of dermatology at Rutgers New Jersey Medical School, to explain what researchers know about the disease.
What is leprosy and why is it resurfacing in the US?
Leprosy is caused by two different but similar bacteria — Mycobacterium leprae and Mycobacterium lepromatosis — the latter having just been identified in 2008. Leprosy, also known as Hansen’s disease, is avoidable. Transmission among the most vulnerable in society, including migrant and impoverished populations, remains a pressing issue.
Leprosy is beginning to occur regularly within parts of the southeastern United States. Most recently, Florida has seen a heightened incidence of leprosy, accounting for many of the newly diagnosed cases in the U.S.
Traditional risk factors include zoonotic exposure and having recently lived in leprosy-endemic countries. Brazil, India and Indonesia have each noted more than 10,000 new cases since 2019, according to the World Health Organization data, and more than a dozen countries have reported between 1,000 to 10,000 new cases over the same time period.
From that time until the mid-20th century, limited treatments were available, so the bacteria could infiltrate the body and cause prominent physical deformities such as disfigured hands and feet. Advanced cases of leprosy cause facial features resembling that of a lion in humans.
Many mutilating and distressing skin disorders such as skin cancers and deep fungal infections were also confused with leprosy by the general public.
Fear of contagion has led to tremendous stigmatization and social exclusion. It was such a serious concern that the Kingdom of Jerusalem had a specialized hospital to care for those suffering from leprosy.
How infectious is leprosy?
Research shows that prolonged in-person contact via respiratory droplets is the primary mode of transmission, rather than through normal, everyday contact such as embracing, shaking hands or sitting near a person with leprosy. People with leprosy generally do not transmit the disease once they begin treatment.
Armadillos represent the only known zoonotic reservoir of leprosy-causing bacteria that threaten humans. These small mammals are common in Central and South America and in parts of Texas, Louisiana, Missouri and other states, where they are sometimes kept as pets or farmed as meat. Eating armadillo meat is not a clear cause of leprosy, but capturing and raising armadillos, along with preparing its meat, are risk factors.
The transmission mechanism between zoonotic reservoirs and susceptible individuals is unknown, but it is strongly suspected that direct contact with an infected armadillo poses a significant risk of developing leprosy. However, many cases reported in the U.S. have demonstrated an absence of either zoonotic exposure or person-to-person transmission outside of North America, suggesting that transmission may be happening where the infected person lives. But in many cases, the source remains an enigma.
Leprosy primarily affects the skin and peripheral nervous system, causing physical deformity and desensitizing one’s ability to feel pain on affected skin.
It may begin with loss of sensation on whitish patches of skin or reddened skin. As the bacteria spread in the skin, they can cause the skin to thicken with or without nodules. If this occurs on a person’s face, it may rarely produce a smooth, attractive-appearing facial contour known as lepra bonita, or “pretty leprosy.” The disease can progress to causing eyebrow loss, enlarged nerves in the neck, nasal deformities and nerve damage.
The onset of symptoms can sometimes take as long as 20 years because the infectious bacteria have a lengthy incubation period and proliferate slowly in the human body. So presumably many people are infected long before they know that they are.
Fortunately, worldwide efforts to screen for leprosy are being enhanced thanks to organizations like the Order of Saint Lazarus, which was originally founded in the 11th century to combat leprosy, and the Armauer Hansen Research Institute, which conducts immunologic, epidemiological and translational research in Ethiopia. The nongovernmental organization Bombay Leprosy Project in India does the same.
How treatable is it?
Leprosy is not only preventable but treatable. Defying stigma and advancing early diagnosis via proactive measures are critical to the mission of controlling and eradicating it worldwide.
Notably, the World Health Organization and other agencies provide multi-drug therapy at no cost to patients.
In addition, vaccine technology to combat leprosy is in the clinical trials stage and could become available in coming years. In studies involving nine-banded armadillos, this protein-based vaccine delayed or diminished leprous nerve damage and kept bacteria at bay. Researchers believe that the vaccine can be produced in a low-cost, highly efficient manner, with the long-term prospect of eradicating leprosy.
If health care professionals, biomedical researchers and lawmakers do not markedly enhance their efforts to eliminate leprosy worldwide, the disease will continue to spread and could become a far more serious problem in areas that have been largely free of leprosy for decades.
The World Health Organization launched a plan in 2021 for achieving zero leprosy.
Flesh-eating bacteria sounds like the premise of a bad horror movie, but it’s a growing – and potentially fatal – threat to people.
In September 2023, the Centers for Disease Control and Prevention issued a health advisory alerting doctors and public health officials of an increase in flesh-eating bacteria cases that can cause serious wound infections.
There are several types of bacteria that can infect open wounds and cause a rare condition called necrotizing fasciitis. These bacteria do not merely damage the surface of the skin – they release toxins that destroy the underlying tissue, including muscles, nerves and blood vessels. Once the bacteria reach the bloodstream, they gain ready access to additional tissues and organ systems. If left untreated, necrotizing fasciitis can be fatal, sometimes within 48 hours.
The bacterial species group A Streptococcus, or group A strep, is the most common culprit behind necrotizing fasciitis. But the CDC’s latest warning points to an additional suspect, a type of bacteria called Vibrio vulnificus. There are only 150 to 200 cases of Vibrio vulnificus in the U.S. each year, but the mortality rate is high, with 1 in 5 people succumbing to the infection.
How do you catch flesh-eating bacteria?
Vibrio vulnificus primarily lives in warm seawater but can also be found in brackish water – areas where the ocean mixes with freshwater. Most infections in the U.S. occur in the warmer months, between May and October. People who swim, fish or wade in these bodies of water can contract the bacteria through an open wound or sore.
Vibrio vulnificus can also get into seafood harvested from these waters, especially shellfish like oysters. Eating such foods raw or undercooked can lead to food poisoning, and handling them while having an open wound can provide an entry point for the bacteria to cause necrotizing fasciitis. In the U.S., Vibrio vulnificus is a leading cause of seafood-associated fatality.
Why are flesh-eating bacteria infections rising?
Vibrio vulnificus is found in warm coastal waters around the world. In the U.S., this includes southern Gulf Coast states. But rising ocean temperatures due to global warming are creating new habitats for this type of bacteria, which can now be found along the East Coast as far north as New York and Connecticut. A recent study noted that Vibrio vulnificus wound infections increased eightfold between 1988 and 2018 in the eastern U.S.
Climate change is also fueling stronger hurricanes and storm surges, which have been associated with spikes in flesh-eating bacteria infection cases.
Aside from increasing water temperatures, the number of people who are most vulnerable to severe infection, including those with diabetes and those taking medications that suppress immunity, is on the rise.
What are symptoms of necrotizing fasciitis? How is it treated?
Early symptoms of an infected wound include fever, redness, intense pain or swelling at the site of injury. If you have these symptoms, seek medical attention without delay. Necrotizing fasciitis can progress quickly, producing ulcers, blisters, skin discoloration and pus.
Treating flesh-eating bacteria is a race against time. Clinicians administer antibiotics directly into the bloodstream to kill the bacteria. In many cases, damaged tissue needs to be surgically removed to stop the rapid spread of the infection. This sometimes results in amputation of affected limbs.
Researchers are concerned that an increasing number of cases are becoming impossible to treat because Vibrio vulnificus has evolved resistance to certain antibiotics.
People who have a fresh cut, including a new piercing or tattoo, are advised to stay out of water that could be home to Vibrio vulnificus. Otherwise, the wound should be completely covered with a waterproof bandage.
People with an open wound should also avoid handling raw seafood or fish. Wounds that occur while fishing, preparing seafood or swimming should be washed immediately and thoroughly with soap and water.
Anyone can contract necrotizing fasciitis, but people with weakened immune systems are most susceptible to severe disease. This includes people taking immunosuppressive medications or those who have pre-existing conditions such as liver disease, cancer, HIV or diabetes.
It is important to bear in mind that necrotizing fasciitis presently remains very rare. But given its severity, it is beneficial to stay informed.