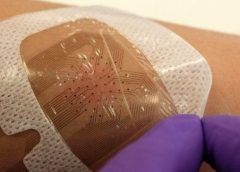
Smart bandages which can detect how well a wound is healing and send a progress report to the doctor will be trialled within the next year, scientists have said. The dressings are fitted with tiny sensors which can pick up blood clotting, or spot infections, and wirelessly send data back to a clinician. Swansea University, which is hoping to trial the bandages within 12 months, said the new technology could offer a personalised approach to medicine.
Currently patients with wounds are advised to return to the doctor in a certain amount of time. But each case may need a longer time to heal, or may have become infected before the visit. (more…)
Read More








