
By Nancy Morgan, MBA, BSN, RN, WOC, WCC, CWCMS, DWC
Each month Apple Bites brings you a tool you can apply in your daily practice.
Description
- Dressing with calcium and sodium fibers made from seaweed
- Spun into rope or flat dressing form
More results...
Practical Issues in Wound, Skin and Ostomy Management

By Donna Sardina, RN, MHA, WCC, CWCMS, DWC
Starting your own consulting business is an exciting and rewarding experience: You’re the boss; you’re in charge. The question is, do you have what it takes? Along with the excitement of being the boss comes the responsibility of decisions and commitment. Your decisions will affect whether the business is a failure or a success.
To succeed in consulting, you must be an expert at recognizing problems and shaping solutions to those problems, and you must possess excellent time-management and networking skills. If you think you have what it takes to be a consultant, read on. This article gives an overview of the process.
Businesses hire consultants for their expertise to help them identify problems, supplement staff, institute change, provide an objective viewpoint, or teach.
Examples of specific services you can offer include single patient reviews, serving as a member of the wound care team, making wound rounds on all patients, providing education, patient teaching, protocol development, and troubleshooting. These services are provided in many settings—long-term care, home care, long-term acute care, rehabilitation hospitals, acute-care hospitals, insurance companies, and primary-care provider groups. (more…)

An angry patient is like an artichoke. An artichoke is prickly and rough on the outside, but by taking time to learn how to peel its rough leaves, you reveal the tender inside. When nurtured under the right conditions, this tender inside grows to bloom into a beautiful purple flower. Patient anger is like the prickly green leaves of the artichoke, it’s a barrier to seeing “inside” and to effectively meeting the patient’s needs (more…)
Read MoreIn a study of 10 venous ulcers not responding to treatment, the use of noncontact ultrasound significantly reduced the wound area over 4 weeks of treatment.
It has been unclear exactly how ultrasound achieves its positive results. The
authors of “A prospective pilot study of ultrasound therapy effectiveness in refractory venous leg ulcers,” an article published online on February 1 by the International Wound Journal, found that patients treated with ultrasound and compression therapy had reduced inflammatory cytokines and bacterial counts, but the reduction wasn’t statistically significant.
The study found another important benefit for patients-reduced pain.
Traditionally the standard of practice for wound care patients has been to review albumin blood levels as a measure of nutritional status and the effect of nutritional interventions. But as noted in The Role of Nutrition in Pressure Ulcer Prevention and Treatment: National Pressure Ulcer Advisory Panel White Paper, recent studies show that hepatic proteins (albumin, transthyretin, and transferrin) correlate with the severity of an underlying disease, not nutritional status. Moreover, many factors can alter albumin levels even when protein intake is adequate, including infection, acute stress, surgery, cortisone excess, and hydration status.
For these reasons, the National Pressure Ulcer Advisory Panel (NPUAP) and the Academy of Nutrition and Dietetics (previously known as The American Dietetic Association) recommend against using serum proteins as a nutritional assessment tool. Evaluation of lab values is just one part of the nutritional assessment process and should be considered along with other factors such as ensuring that the patient receives what is prescribed; daily food/fluid intake; changes in weight status, diagnosis, and medications; and clinical improvement in the wound.
For more information read “Serum proteins as markers of malnutrition: What are we treating?” and “Albumin as an indicator of nutritional status: Professional refresher.”
“Wound care outcomes and associated cost among patients treated in US outpatient wound centers: Data from the US Wound Registry” a study using data from the US Wound Registry to determine outcomes and costs for outpatient wound care, found the mean patient age was 61.7 years, slightly more than half (52.3%) were male, most (71.3%) were white, and more than half (52.6%) were Medicare beneficiaries.
Other interesting findings:
The authors of the article, published in March’s Wounds, analyzed 5,240 patients with 7,099 wounds in 59 hospital-based outpatient wound centers in 18 states over 5 years.
The pilot study “Lanarkshire Oximetry Index as a diagnostic tool for peripheral arterial disease in type 2 diabetes,” published in Angiology, compared the gold standard ankle brachial index (ABI) to the Lanarkshire Oximetry Index (LOI) in 161 patients with type 2 diabetes. Researchers assessed the patients for peripheral artery disease (PAD, defined as ABI < 0.9) using both ABI and LOI.
Using a LOI cut-off value of 0.9., the sensitivity and specificity for PAD were 93.3% and 89.1%, respectively. The study concluded that LOI is a “potentially useful alternative diagnostic test for PAD” in patients with type 2 diabetes.
LOI is a noninvasive procedure similar to ABI; both indices indicate whether it’s safe to apply compression to the limb of a patient who has lower leg ulceration or venous hypertension. With LOI, a pulse oximeter is used in place of a hand-held Doppler to determine the index.
It’s not too early to begin planning for World Diabetes Day, November 14. Started by the World Health Organization (WHO) and the International Diabetes Federation (IDF), the day is designed to raise global awareness of diabetes.
Access materials, including posters, a campaign book, and the Word Diabetes Day Logo, from IDF’s website, which also has activity ideas.
WHO estimates that more than 346 million people worldwide have diabetes, and the number is expected to double by 2030. World Diabetes Day is celebrated on November 14 to mark the birthday of Frederick Banting who, along with Charles Best, was instrumental in the discovery of insulin in 1922.
February’s issue of Diabetes/Metabolism Research and Reviews includes “Specific guidelines for the diagnosis and treatment of peripheral arterial disease in a patient with diabetes and ulceration of the foot 2011,” which is based on two companion International Working Group on the Diabetic foot papers. The guidelines state that if a patient’s PAD is impairing wound healing, revascularization through bypass or endovascular technique must be considered except in a few cases such as severely frail patients. Limb salvage rates after revascularization procedures are about 80-85%, and there is ulcer healing in > 60% at 12 months.
Other points of particular interest to wound care professionals:
“A call to action: Women and peripheral artery disease: A scientific statement from the American Heart Association” summarizes evidence in this area and addresses risk-management issues. The statement notes that women (particularly black females) are more likely than men to experience graft failure of limb loss and calls for more research related to PAD and gender.
Read More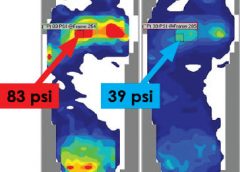
By: Darlene Hanson, MS, RN, Pat Thompson, MS, RN, Diane Langemo, PhD, RN, FAAN, Susan Hunter, MS, RN, and Julie Anderson, PhD, RN, CCRC
Faced with the nursing diagnosis of Impaired skin integrity, we’ve all written care plans that state our goal as “redistributing or reducing pressure.” But how do we do that? Which measures do we take? And how do we know that our interventions have relieved pressure? Do we rely solely on a skin assessment? A patient’s self-assessment of comfort? What if the patient can’t feel pressure relief because of neurologic impairment?
The answers to these questions may be that nurses should use pressure mapping, a tool used by occupational and physical therapists to determine seat-interface pressures and by other healthcare professionals to perform foot assessments. (more…)
Read MoreMoisture-related skin breakdown has been called many things-perineal dermatitis, irritant dermatitis, contact dermatitis, heat rash, and anything else caregivers could think of to describe the damage occurring when moisture from urine or stool is left on the skin. At a 2005 consensus conference, attendees chose the term incontinence-associated dermatitis (IAD).
IAD can be painful, hard to properly identify, complicated to treat, and costly. It’s part of a larger group of moisture-associated skin damage that also includes intertrigo and periwound maceration. IAD prevalence and incidence vary widely with the care setting and study design. Appropriate diagnosis, prompt treatment, and management of the irritant source are crucial to long-term treatment.
IAD stems from the effects of urine, stool, and containment devices on the skin. The skin’s pH contributes to its barrier functions and defenses against bacteria and fungus; ideal pH is 5.0 to 5.9. Urine pH ranges from 4.5 to 8.0; the higher range is alkaline and contributes to skin damage.
Skin moisture isn’t necessarily damaging. But when moisture that contains irritating substances, such as alkaline urine, contacts the skin for a prolonged period, damage can occur. Urine on the skin alters the normal skin flora and increases permeability of the stratum corneum, weakening the skin and making it more susceptible to friction and erosion. Fecal incontinence leads to active fecal enzymes on the skin, which contribute to skin damage. Fecal bacteria can penetrate the skin, increasing the risk of secondary infection. Wet skin has a lower temperature than dry skin; wet skin under a pressure load has less blood flow than dry skin.
Containment devices, otherwise known as adult diapers or briefs, are multilayer disposable garments containing a superabsorbent polymer. The polymer is designed to wick and trap moisture in the containment device. This ultimately affects the skin by trapping heat and moisture, which may cause redness and inflammation that can progress to skin erosion. This trapping can lead to increased pressure against the skin, especially if the device has absorbed liquid and remains in contact with the skin.
IAD is categorized as mild, moderate, or severe. (See Picturing IAD by clicking the PDF icon above.)
Screen the patient’s skin for persistent redness, inflammation, rash, pain, and itching at least daily. To differentiate IAD from pressure ulcers, keep in mind that:
The three essentials of IAD prevention are to cleanse, moisturize, and protect.
If the treatment protocol fails, the patient should be referred to an appropriate skin care specialist promptly.
To help prevent urine or stool from contacting the patient’s skin, consider using a male external catheter, a female urinary pouch, a fecal pouch, or a bowel management system. Avoid containment devices. If the patient has a containment pad, make sure it’s highly absorbent and not layered, to decrease pressure under the patient.
A comprehensive multidisciplinary approach to IAD is essential to the success of any skin care protocol. Identify skin care champions within your facility and educate them on IAD. Incorporating administrators, physicians, nursing staff, therapists, and care assistants makes implementation of protocols and algorithms within an institution seamless.
Administrators support the skin care program in the facility, including authorizing a budget so product purchases can be made. The certified wound clinician is the team expert regarding skin care, incontinence, prevention, and product recommendation. The physician oversees protocol development and evaluates and prescribes additional treatment when a patients fails to respond to treatment algorithms. Nursing staff identify patients at risk, incorporate the algorithm into the patient’s plan of care, and direct care
assistants. Therapists address function, strength, and endurance issues to improve the patient’s self-care abilities in activities of daily living to manage or prevent episodes of incontinence.
In severe inflammation, topical dressings, such as alginates and foam dressings, may be used along with topical corticosteroids. In complex IAD, antifungals or antibiotics may be required if a secondary fungal or bacterial infection is suspected.
Additional diagnostic tests may be done to identify and treat secondary infections. These tests may include skin scraping, potassium hydroxide test or Gram’s stain for fungal components, or a swab culture and sensitivity for bacterial infections. If your patient has a suspected secondary fungal or bacterial infection, use appropriate treatments for the full course of recommended therapy. In severe secondary fungal infection, an oral agent may be added to topical therapy. If cost is a concern, consider using a pharmacy knowledgeable about compounding for topical combination therapies.
For assessment and treatment of under-lying incontinence, refer the patient to a continence specialist if appropriate. Teach the patient strategies for managing incontinence through dietary measures, toileting programs, pelvic-floor muscle training, clothing modification, and mobility aids.
Selected references
Beguin A, Malaquin-Pavan E, Guihaire C, et al., Improving diaper design to address incontinence associated dermatitis. BMC Geriatrics. 2010;10:86. http://www.biomedcentral.com/1471-2318/10/86. Accessed March 15, 2012.
Black JM, Gray M, Bliss DZ, et al. MASD part 2: incontinence-associated dermatitis and intertriginous dermatitis. J Wound Ostomy Continence Nurs. 2011; 38(4):359-370.
Bliss DZ, Zehrer C, Savik K, et al. An economic evaluation of four skin damage prevention regimens in nursing home residents with incontinence: economics of skin damage prevention. J Wound Ostomy Continence Nurs. 2007;34(2):143-152.
Denat Y, Khorshid L. The effect of 2 different care products on incontinence-associated dermatitis in patients with fecal incontinence. J Wound Ostomy Continence Nurs. 2011;38(2):171-176.
Doughty DB. Urinary and Fecal Incontinence: Current Management Concepts. 3rd ed. St. Louis, MO: Mosby Elsevier; 2006.
Gray, M. Optimal management of incontinence-associated dermatitis in the elderly. Am J Clin Dermatol. 2010;11(3):201-210.
Gray M, Beeckman D, Bliss DZ, et al. Incontinence-associated dermatitis: a comprehensive review and update. J Wound Ostomy Continence Nurs. 2012;39(1):61-74
Gray M, Bliss DZ, Doughty DB, et al. Incontinence-associated dermatitis: a consensus. J Wound Ostomy Continence Nurs. 2007;34(1):45-54.
Gray M, Bohacek L, Weir D, et al. Moisture vs pressure: making sense out of perineal wounds. J Wound Ostomy Continence Nurs. 2007;34(2):134-42.
Institute for Clinical Systems Improvement. Health care protocol: Pressure ulcer prevention and treatment. Bloomington, MN: Institute for Clinical Systems Improvement. January 2012. http://www.icsi.org/pressure_ulcer_treatment_protocol__review_and_comment_/pressure_ulcer_treatment__protocol__.html. Accessed March 15, 2012.
Junkin J, Lerner-Selekof JL. Prevalence of incontinence and associated skin injury in the acute care inpatient. J Wound Ostomy Continence Nurs. 2007;34(3):260-269.
Landefeld CS, Bowers BJ, Feld AD, et al. National Institutes of Health state-of-the-science conference statement: prevention of fecal and urinary incontinence in adults. Ann Intern Med. 2008;148(6):449-458.
Langemo D, Hanson D, Hunter S, et al. Incontinence and incontinence-associated dermatitis. Adv Skin Wound Care. 2011;24(3):126-142.
Scheinfeld NS. Cutaneous candidiasis workup. 2011 update. http://emedicine.medscape.com/article/1090632-workup. Accessed March 15, 2012.
U.S. Census Bureau. The older population 2010. November 2011. www.census.gov/prod/cen2010/briefs/c2010br-09.pdf. Accessed March 15, 2012.
Nancy Chatham is an advanced practice nurse at Passavant Physician Associates in Jacksonville, Illinois. Carrie Carls is the nursing director of advanced wound healing and hyperbaric medicine at Passavant Area Hospital in Jacksonville, Illinois.
Read MoreAhhh—the front seat, shotgun, the good spot, the privilege-to-sit-in and most coveted of all positions when riding in a car. Those are great words if you’re the caller to stake your claim for the front seat, but not so great if you’re the one stuck in the back seat.
In the world of health care, wound and skin care unfortunately never gets to ride shotgun. It seems like we always get the back seat unless there’s a problem. Think back to your college days. Do you remember Wound and Skin Care 101 and the torture of memorizing all 2,000 wound care products on the market, the endless case studies and wound differentiation quizzes? No? Well neither do I. If your schooling was like mine, you learned about sterile dressing changes, wet-to-dry dressings, Montgomery straps, and if you were lucky, how to apply an ostomy bag.
Granted, I went to nursing school in the 1970s. But things haven’t changed much. Wound care still gets the back seat when it comes to educational priorities. A survey by Ayello, Baranoski, and Salati of 692 registered nurses found that 70% considered their basic wound care education to be insufficient and fewer than 50% of new nurses believed they could consistently identify pressure ulcer stages. Another survey of nursing textbooks revealed students could be exposed to as few as 45 lines of text on pressure ulcers.
It’s not just lack of nursing education, but also poor physician education. As reported in a poster by Garcia and colleagues, only 8 of 50 medical residents scored more than 50% on a 20-question test measuring pressure ulcer knowledge, with a high score of 65% (range, 13.04% to 76.09% correct).
It’s time for a change, and I’m excited to be a part of a new tool to help move wound and skin care education to the front seat: Wound Care Advisor, the official journal of the National Alliance of Wound Care (NAWC). With its “Don’t just tell me, but show me” approach, the journal will feature plenty of photographs, step-by-step instructions, and video how-to’s. If you’re like me and prone to attention deficit, you’re in luck. We’ll keep things practical and to the point, with a “learn it today and do it tomorrow” mantra.
Another cutting-edge feature of the journal is the electronic-only format; this isn’t a print journal. The no-paper format will help us declutter our lives and minimize our ecological footprint. Not to worry, though: With our print-on-demand feature, you can always print out individual articles or even the entire journal if you want.
In keeping with NAWC principles, Wound Care Advisor is geared toward all care settings and a multidisciplinary audience. This isn’t just the NAWC journal; it’s your journal. We need you to help us move wound care from the back seat to the front seat of the car by sharing your knowledge and passion for wound and skin care. Call or e-mail us your case studies, best practices, tools, forms, wound photos, or even feedback about the journal.
I truly believe that together, you, I, NAWC, and Wound Care Advisor can move wound and skin care education to the front seat. I look forward to working with you on the ride to the coveted shotgun seat.
Donna Sardina, MHA, RN, WCC, CWCMS
Editor-in-Chief
Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Selected references
Ayello EA, Baranoski S. Examining the problem of pressure ulcers. Adv Skin Wound Care. 2005; 18:192-194.
Ayello EA, Baranoski S, Salati DS. A survey of nurses’ wound care knowledge. Adv Skin Wound Care. 2005;18(5 Pt 1):268-275.
Ayello EA, Meaney G. Replicating a survey of pressure ulcer content in nursing textbooks. J Wound Ostomy Continence Nurs. 2003;30(5): 266-271.
Garcia AD, Perkins C, Click C, Bergstrom N, Taffet G. Pressure ulcers education in primary care residencies. Poster session presented at 19th Annual Clinical Symposium on Advances in Skin & Wound Care. September 30-October 3, 2004; Phoenix, Arizona.

By combining bioactive peptides, researchers have successfully stimulated wound healing in an in vitro and in vivo study. The studies, published in PLoS ONE, show that the combination of two peptides stimulates growth of blood vessels and promotes tissue re-growth of tissue. Further research into these peptides could potentially lead to new therapies for chronic and acute wounds.
The researchers evaluated a newly-created peptide, UN3, in pre-clinical models with the goal of simulating impaired wound healing as in patients suffering from peripheral vascular diseases or uncontrolled diabetes. They discovered that the peptide increased the development of blood vessel walls by 50%, with an 250% increase in blood vessel growth, and a 300% increase in cell migration in response to the injury. (more…)
Read MoreWound Care Advisor, is dedicated to delivering succinct insights and information that multidisciplinary wound team members can immediately apply in their practice and use to advance their professional growth. If you’re considering writing for us, please use these guidelines to help choose an appropriate topic and learn how to prepare and submit your manuscript. Following these guidelines will increase the chance that we’ll accept your manuscript for publication
 About the journal
About the journalWound Care Advisor serves as a practical resource for multidisciplinary skin and would care specialists. The journal provides news, clinical information, and insights from authoritative experts to enhance skin and wound care management. Wound Care Advisor is written by skin and wound care experts and presented in a reader-friendly electronic format. Clinical content is peer reviewed. It also serves as a resource for professional development and career management.
The journal is sent to Certificants of the National Alliance of Wound Care and Ostomy and other healthcare professionals, who are also dedicated to improving skin and wound care.
Each issue of Wound Care Advisor offers compelling feature articles on clinical and professional topics, plus regular departments. We publish articles that present clinical tips and techniques, discuss new or innovative treatments, provide information on technology related to wound care, review medical conditions that affect wound healing such as diabetes and cardiovascular disease, address important professional and career issues, and other topics of interest to wound care specialists.
We accept submissions for these departments:
Best Practices, which includes case studies, clinical tips from wound care specialists, and other resources for clinical practice
Business Consult, which is designed to help wound care specialist manage their careers and stay current in relevant healthcare issues that affect skin and wound care.
We also welcome case studies. Please use the WCA Case Study Template as a guide
Please send a brief email query to [email protected]. In the email, state 1) the topic of your proposed article, 2) briefly describe what the article will include, 3) provide a short summary of your background, and 4) explain why you’re qualified to write on this topic. We will respond whether or not we are interested in the article you have proposed.
Our journal is written in simple, concise language. The tone is informal, and articles are short to medium in length (about 600 words for departments and 1200 words for feature articles). When writing the manuscript, follow these guidelines:
For reference style, use the American Medical Association Manual of Style: A Guide for Authors and Editors (10th ed). If you don’t have access to this book, include at least the following information for each reference you cite:
For a book: author(s), book title, edition (if appropriate), place of publication, publisher, and publication date
For a print journal article: author(s); article title; journal name; year, volume; inclusive page numbers
For online references: URL (web address) and the date you accessed the website.
We encourage you to submit tables, photographs, and illustrations for your article (although we can’t guarantee we’ll publish them).
The article must be your own original work. Do not submit material taken verbatim from a published source.
Submit your manuscript electronically as an MS Word file. Follow these guidelines:
Thank you for considering publishing in Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy, the official. If you have any questions, please email: Cynthia Saver, RN, MS, at [email protected] or [email protected].
Copyright © 2017, HealthCom Media. All rights reserved.
Read More