The challenge of preventing pressure ulcers is won through our frontline staff—the patient’s caregivers. Caregivers deliver most of the pressure ulcer preventive interventions, such as turning and repositioning, floating the heels, and managing incontinence. That’s why it’s imperative to communicate the patient’s plan of care directly to the caregivers. (more…)
Here is a list of valuable ostomy resources, some suggested by our colleagues who follow Wound Care Advisor on Twitter.
United Ostomy Association of America
The United Ostomy Association of America provides comprehensive resources for patients, including information about the types of ostomies and issues related to nutrition, sexuality, and travel. Much of the information is also available in Spanish and can be downloaded for free from the website. (more…)
By Catherine R. Ratliff, PhD, APRN-BC, CWOCN, CFCN
It’s estimated that about 70% of the 1 million ostomates in the United States and Canada will experience or have experienced stomal or peristomal complications. Peristomal complications are more common, although stomal complications (for example, retraction, stenosis, and mucocutaneous separation) can often contribute to peristomal problems by making it difficult to obtain a secure pouch seal. This article will help you differentiate types of peristomal complications, including how to prevent and manage them. (more…)
This issue’s resources include patient tools and new guidelines.
Improving patient safety
Research suggests that adverse events affect patients with limited English proficiency (LEP) more frequently, are commonly caused by communication problems, and are more likely to result in serious harm compared to adverse events affecting English-speaking patients. Your hospital can take steps to reduce risks of adverse events for patients with LEP with “Improving patient safety systems for patients with limited english proficiency: a guide for hospitals,” from The Disparities Solutions Center, Mongan Institute for Health Policy at Massachusetts General Hospital, Boston, and Abt Associates, Cambridge, Massachusetts. (more…)
Take a few minutes to check out this potpourri of resources.
International Ostomy Association
The International Ostomy Association is an association of regional ostomy associations that is committed to improving the lives of ostomates. Resources on the association’s website include:
a variety of discussion groups
information for patients
list of helpful links.
The site also provides contact information for the regional associations. (more…)
No matter where you work or who your distributors are, ensuring the patient has sufficient ostomy supplies can be a challenge. Whether you’re the nurse, the physician, the patient, or the family, not having supplies for treatments can heighten frustration with an already challenging situation, such as a new ostomy. Here’s how to reduce the chance of experiencing frustrations related to ostomy supplies. (more…)
By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS
Imagine your physician has just told you that your rectal pain and bleeding are caused by invasive colon cancer and you need prompt surgery. She then informs you that surgery will reroute your feces to an opening on your abdominal wall. You will be taught how to manage your new stoma by using specially made ostomy pouches, but will be able to lead a normal life.
Like most people, you’d probably be in shock after hearing this. More than 700,000 people in the United States are living with ostomies. Every year, at least 100,000 ostomy surgeries are done, preceded by a conversation much like the one above. So how do patients recover from the shock of learning about their pending surgery—and then return to a full life? (more…)
By Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC, OMS; and Judith LaDonna Burns, LPN, WCC, DFC
About 1 million people in the United States have either temporary or permanent stomas. A stoma is created surgically to divert fecal material or urine in patients with GI or urinary tract diseases or disorders.
A stoma has no sensory nerve endings and is insensitive to pain. Yet several complications can affect it, making accurate assessment crucial. These complications may occur during the immediate postoperative period, within 30 days after surgery, or later. Lifelong assessment by a healthcare provider with knowledge of ostomy surgeries and complications is important. (more…)
By Rosalyn Jordan, RN, BSN, MSc, CWOCN, WCC, and Marci Christian, BBE
Any patient with a fecal or urinary ostomy may experience complications on the skin surface around the stoma. These complications may occur lifelong, although they’re more common during the first 5 years after the initial ostomy surgery. Causative factors include infection, trauma, certain diseases, and chemical irritation; most of these problems stem from the pouching system or pouch leakage.
Peristomal skin complications can cause a wide range of signs and symptoms, from skin discoloration to polyp-like growths, from erythema to full-thickness wounds. They can lead to discomfort, pain, poor self-image, social isolation, and impaired quality of life, not to mention additional care costs.
Incidence and types of these complications are hard to compare or contrast across multiple patients. Until recently, no standardized assessment or documentation tools were available to characterize or define complications. For this reason, reported rates ranged widely, from 10% to 70%. And because no designated common language or categories related to peristomal skin complications existed, documentation was inconsistent.
In the late 2000s, a group of nurses experienced in caring for ostomy patients worked with the World Council of Enterostomal Therapists to develop a resource called the Ostomy Skin Tool, which clinicians can use to categorize and describe peristomal skin complications in a consistent, objective manner. The tool also provides a common language for documentation.
The Ostomy Skin Tool has three major assessment domains—discoloration (D), erosion/ulceration (E), and tissue overgrowth (T), known collectively as DET. The DET combined rating ranges from normal, rated 0, to the worst condition possible, rated 15. Mild DET complications are documented as less than 4, moderate as less than 7, and severe as 8 or higher. (See Using the Ostomy Skin Tool by clicking the PDF icon above.)
The tool describes four categories of peristomal complications:
• chemical irritation
• mechanical trauma
• disease-related complications
• infection-related complications.
Chemical irritation
Chemical irritation can stem from irritants (as in contact dermatitis) or allergic reactions (allergic dermatitis). The most likely cause of chemical dermatitis is effluent leakage (feces or urine) from the colostomy, ileostomy, or urostomy, in which effluent comes in contact with peristomal skin. Other potential causes include contact with soap, certain adhesives, and adhesive removers.
The major treatment of chemical irritation is identification and removal of the offending agent, followed by patient and caregiver education on the new pouching procedure the patient must use. Follow-up assessment also is recommended. In a 2010 study that followed 89 patients for 1 year after ostomy surgery, about 50% of subjects experienced peristomal skin complications, most of them from pouch leakage. Another investigator estimated that 85% of ostomy patients experience pouch leakage at some time during their lives. Pouch leakage usually occurs when stool is extremely liquid (for instance, ileostomy effluent). Other causes of pouch leakage include wearing a pouch more than half full of effluent and abdominal contours that aren’t level. Besides changes in the pouching system, treatment may entail adding products to the pouching system or removing certain agents.
Some patients experience allergic dermatitis in reaction to products used in the pouching system (such as skin barriers, belts, pouch closures, or adhesives). However, allergic dermatitis is rare. One 2010 study suggested allergic reactions to these products occur in only about 0.6% of patients with peristomal skin irritation. Most major ostomy product manufacturers provide a patch test on request to help identify allergic conditions. Once the offending product is discontinued, allergic dermatitis should resolve rapidly.
Mechanical trauma
Mechanical trauma usually results from either the pouching system itself or its removal. It also may result from harsh or multiple skin-barrier removals, pressure from convex rings or pouches, and abrasive cleansing techniques. Some researchers believe the stronger the adhesive barrier and the more often a pouch is changed, the greater the risk of epidermal damage.
Mechanical trauma may present as a partial-thickness ulcer caused by pressure, shear, friction, tearing, or skin stripping. Patients with fragile skin are susceptible to mechanical trauma, so less aggressive pouching systems may be preferred for them. Of course, if the pouching system is changed, the patient or caregiver needs to learn about the new system.
Disease-related complications
Disease-related peristomal complications may be linked to preexisting skin conditions, such as psoriasis, eczema (atopic dermatitis), or seborrheic dermatitis. Hyperplasia also may occur. This overgrowth of cells, which may appear as gray or reddish brown pseudoverrucous lesions, usually is linked to urinary ostomies, although it can occur with fecal ostomies as well. Vinegar soaks are the recommended treatment, in addition to a change in the pouching system and corresponding patient education.
Occasionally, other disease-related complications occur, including primary adenocarcinoma of the peristomal skin and peristomal pyoderma gangrenosum, a painful and problematic condition that presents as peristomal ulcers. Ulcer borders are well-defined with a bluish purple coloration at the edges. Infection must be ruled out, as this condition usually is linked to an autoimmune condition. Treatment includes pain management and, in most cases, a topical corticosteroid. Crohn’s disease also may manifest as a peristomal skin ulcer.
Infection-related complications
Infection-related complications may be bacterial or fungal. Two common peristomal skin infections are folliculitis and Candida fungal infections. An infection of the hair follicle that causes pustules, folliculitis usually stems from traumatic hair pulling in the peristomal area during pouch removal. It may warrant a prescribed antibiotic, along with patient teaching regarding proper hair removal using an electric razor.
Candida infections may arise because peristomal skin provides a warm, dark, moist environment that promotes fungal growth. These infections appear as erythema with pustules or papules and satellite lesions. Treatment usually involves antifungal powder and use of the crusting technique to secure the pouching system. (See Using the crusting technique by clicking the PDF icon above.)
Management
Many complications are well advanced by the time patients seek assistance, perhaps because they don’t understand the significance of their symptoms and think they can manage the problem themselves. In some cases, they don’t know where to turn for assistance. Commonly, the complication progresses to the point where the patient goes to the emergency department or (particularly during the immediate postoperative period) needs to be readmitted for treatment. The best way to manage peristomal skin complications is to prevent them in the first place. (See Preventing peristomal skin complications by clicking the PDF icon above.)
Patient education
Over the past 20 years, hospital stays for ostomy surgery patients have decreased from about 2 weeks to less than 5 days. Reduced stays decrease the time available for caregivers to teach patients and family members how to empty and change the pouch. They need alternative education covering (among other topics) how to recognize peristomal skin complications and when to seek help. Not only do these complications require vigilant self-observation, but many patients don’t understand their implications or how rapidly they can worsen. In some cases, the first symptoms are itching and redness under the skin barrier. Fortunately, some patients may know or remember that itching, burning, stinging, reddened, or weeping peristomal skin requires professional attention. They can avoid serious complications by seeking assistance early, such as right after noticing pouch leakage.
Early treatment can reduce the cost of treatment. In a 2012 study, researchers estimated care costs related to peristomal skin complications for a 7-week treatment period, using the Ostomy Skin Tool as a reference. Severe complications (those with a DET score above 8) cost six times more to treat than mild cases (those with a DET score below 4) and 4.5 times more than moderate cases.
Along with early intervention by a trained ostomy care specialist, self-assessment by ostomy patients promotes a better quality of life, reduces pain, and may decrease care costs. Clinicians’ use of the Ostomy Skin Tool to assess and document peristomal skin complications promotes more reliable, objective, comparable assessment data for reporting.
Selected references
Al-Niaimi F, Lyon CC. Primary adenocarcinoma in peristomal skin: a case study. Ostomy Wound Manage. 2010;56(1):45-7.
Burch J. Management of stoma complications. Nurs Times. 2011;107(45):17-8, 20.
Jemec GB, Martins L, Claessens I, et al. Assessing peristomal skin changes in ostomy patients: validation of the Ostomy Skin Tool. Br J Dermatol. 2011; 164;330-5.
Jones T, Springfield T, Brudwick M, Ladd A. Fecal ostomies: practical management for the home health clinician. Home Healthc Nurse. 2011;29(5):306-17.
Martins L, Samai O, Fernandez A, et al. Maintaining healthy skin around an ostomy: peristomal skin disorders and self-assessment. Gastrointest Nurs. 2011;
9(2):9-13.
Martins L, Tavernelli K, Serrano JLC. Introducing a peristomal skin assessment tool: The Ostomy Skin Tool. World Council Enterostomal Therapists J. 2008;28(2):3-13.
Meisner S, Lehur P, Moran B, et al. Peristomal skin complications are common, expensive, and difficult to manage: a population based cost modeling study. PLoS One. 2012;7(5):e37813.
Omura Y, Yamabe M, Anazawa S. Peristomal skin disorders in patients with intestinal and urinary ostomies: influence of adhesive forces of various hydrocolloid wafer skin barriers. J Wound Ostomy Continence Nurs. 2010;37(3):289-98.
Ratliff CR. Early peristomal skin complications reported by WOC nurses. J Wound Ostomy Continence Nurs. 2010;37(5):505-10.
Shabbir J, Britton DC. Stomal complications: a literature overview. Colorectal Dis. 2010;12(10):958- 64.
Wound, Ostomy, Continence Clinical Practice Ostomy Subcommittee. Peristomal skin complications: Best practice for clinicians. Mt. Laurel, NJ; 2007.
The authors work for RecoverCare, LLC, in Louisville, Kentucky. Rosalyn Jordan is director of clinical education and Marci Christian is a clinical associate product specialist.
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
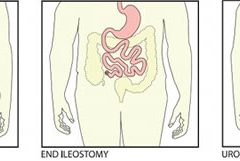
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
In most cases, amputation (removal of an extremity, digit, or other body part) is a surgical intervention performed to remove tissue affected by a disease and, in some cases, to provide pain relief. Fecal and urinary diversion surgeries also are considered amputations. Amputations and fecal or urinary diversions (ostomies) require extensive rehabilitation and adaptation to a new way of life, with physiologic and psychological impacts. Although diversions and ostomies usually are less visible to others than other types of amputations, they call for similar patient education, rehabilitatio n, and lifelong counseling.
The primary goal of therapy for ostomates and amputees is to resume their presurgical lifestyle to the greatest extent possible and to adapt to their new circumstances. Preoperative assessment and training interventions have proven valuable. Having a clear understanding of the surgical intervention helps reduce postoperative anxiety and depression, which can pose roadblocks to patients’ adaptation or response to their new situation. Successful interventions should be done by healthcare professionals who are trained in caring for ostomates and amputees.
Ostomates and amputees experience similar psychosocial challenges, body-
image problems, and sexuality concerns. This article focuses on these three issues. For a summary of other issues these patients may experience, see Other problems amputees and ostomates may face by clicking the PDF icon above.
Psychosocial challenges
Ostomates and amputees may experience depression, anxiety, fear, and many other concerns related to the surgical procedure—concerns that center on whether they’ll be able to resume their presurgical lifestyle. Many worry about social isolation and loss of income. Some fear both the primary disease process and the lifestyle changes induced by surgery. Anxiety may impede their social interactions and lead to significant psychological problems. Appropriate and effective counseling and therapy must be planned and provided. (But be aware that untrained or inexperienced healthcare professionals may not be able to provide the guidance the patient needs to feel comfortable; some may be unable even to offer information about available support systems.)
These patients also may find themselves socially isolated, in part due to loss of employment or the socioeconomic consequences of a decreased income. Some experience fear and worry when anticipating lifestyle changes caused by loss in or change of function, adaptation to the prosthesis, and treatment costs.
Maintaining social contact after surgery is extremely important to recovery and adaptation to the amputation or ostomy. The United Ostomy Associations of America and the Amputee Coalition encourage patients to maintain social involvement. Both groups suggest patients discuss their feelings, thoughts, and fears with a trusted family member, friend, or partner. Both organizations sponsor and encourage support-group involvement. In some cases, emotional support from other amputees or ostomates with a similar experience may be appropriate; some patients may be more comfortable sharing thoughts and asking questions in a group of people with similar experiences. Resuming presurgical social events and activities can enhance patients’ adaptation to a new way of life.
Ostomates and amputees have to cope not only with changes in physical appearance but with how their body functions and how they feel and perceive their body. They’re keenly aware of their changed appearance and are concerned about others’ perceptions of them. They may feel anxious and depressed related to body image; the degree of anxiety and depression may relate directly to their presurgical body image and activities. Many become anxious and fearful as they adapt to the prosthesis. (See Stages of grief by clicking the PDF icon above.)
Compared to amputees, ostomates may have more concerns about body image with sexual partners, because the stoma is, in a sense, a hidden amputation. In most cases, the stoma and pouch can be obscured visually from others. The amputee, on the other hand, has fewer options for hiding the missing body part.
To help patients cope with body-image problems, care providers must offer education, therapy, and counseling to help the patient accept and successfully adapt to the body-image change. The first step in this process may simply be to have the patient look at the stoma or stump, progressing to participation in prosthesis care.
Sexuality concerns
Many ostomates and amputees have difficulty resuming sexual activity after surgery. Although the stoma usually remains hidden from others, it’s observable to the ostomate and sex partner. Most patients require an adjustment period before they feel comfortable with a sex partner. They may fear that:
• the partner will reject them or no longer find them attractive
• they will experience loss of function and sensation
• they will experience pain or injury of the stoma.
They also may feel embarrassed, causing them to avoid sex. However, counselors can help couples discuss these concerns and resume a satisfactory sexual relationship. Ostomates and amputees and their partners may need counseling to resume a satisfactory sexual relationship. If they continue to have adjustment difficulties, referral to a trained sex counselor or psychologist may be indicated. Several studies show that appropriate counseling can help prevent complications and allow amputees and ostomates to continue to express their affection physically. (See Talking to patients about sexual problems by clicking the PDF icon above.)
Resuming sexual activity may be easier if the ostomate or amputee had a sex partner before surgery. However, males who experience postsurgical erectile dysfunction are less likely than other males to resume sexual activity. Counseling encourages postsurgical patients to focus more on the pleasurable feelings they and their partners feel, rather than on sexual performance. Body-image problems and inadequate sexual adjustment go hand in hand. (See Helping ostomates resume sex by clicking the PDF icon above.)
Team approach to patient education and counseling
In many parts of the country, a designated healthcare team manages amputees’ care and rehabilitation. But until recently, nurses were the only professionals certified to participate in ostomates’ care and rehabilitation. In fact, ostomates may represent a significant underserved population. A 2012 study found many ostomy patients didn’t receive consistent training and counseling from ostomy certified nurses. Only 13% of respondents reported they had regular visits with an ostomy certified nurse; 32% said they’d never received care from an ostomy nurse. Just over half (56%) indicated they saw an ostomy nurse when they thought it was necessary. The study also reported that 57% hadn’t seen an ostomy certified nurse in more than 1 year.
A team with specialized training to address ostomates’ physical and psychosocial needs might be able to provide the specialized care these patients need. The primary medical caregiver or general practitioner would serve as team leader and make appropriate referrals. The team should include a surgeon, ostomy- and amputee-trained nurses, a prosthetist or other healthcare provider trained in selection and fitting of prosthetic equipment and devices that affect function, a physical therapist, an occupational therapist, a social worker, a vocational counselor, a psychologist, caregiver or family members, support groups, and (last but not least) the patient.
The team approach might reduce hospital stays and promote patients’ return to their home environment. It also might encourage independence and enhance the success of long-term adaptation.
Focus on the future
Healthcare providers should encourage ostomates and amputees to focus on the future, not the past. Feeling comfortable with the prosthesis—the amputee’s artificial limb or the ostomate’s pouching system—is essential to adapting to a “new normal” way of life. Maintaining social relationships is important to adaptation as well. Mastering basic skills and adapting to changes in body function help improve the patient’s quality of life. Follow-up visits, phone contact, and access to a team of well-trained healthcare providers for patient education, rehabilitation, and long-term management are crucial to these patients’ successful adaptation and quality of life.
Selected references
Bhuvaneswar CG, Epstein LA, Stern TA. Reactions to amputation: recognition and treatment. Prim Care Companion J Clin Psychiatry. 2007;9(4):303-8.
Davidson T, Laberge M. Amputation. Gale Encyclopedia of Surgery: A Guide for Patients and Caregivers. 2004. www.encyclopedia.com/doc/1G2-3406200023.html. Accessed December 20, 2012.
Erwin-Toth P, Thompson SJ, Davis JS. Factors impacting the quality of life of people with an ostomy in North America: results from the Dialogue Study. J Wound Ostomy Continence Nurs. 2012;39(4):417-22.
Maguire P, Parkes CM. Surgery and loss of body parts. BMJ. 1998;316(7137):1086-8.
Pittman J, Kozell K, Gray M. Should WOC nurses measure health-related quality of life in patients undergoing intestinal ostomy surgery? J Wound Ostomy Continence Nurs. 2009;36(3):254- 65.
Pittman J. Characteristics of the patient with an ostomy. J Wound Ostomy Continence Nurs. 2011;38(3):271-9.
Racy JC. Psychological adaptation to amputation. In Bowker JH, Michael JW, ed. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2nd ed. Rosemont, IL: American Academy of Orthopedic Surgeons; 1998.
Tunn PU, Pomraenke D, Goerling U, Hohenberger P. Functional outcome after endoprosthetic limb-salvage therapy of primary bone tumours—a comparative analysis using the MSTS score, the TESS and the RNL index. Int Orthop. 2008;32(5):619-25.
Turnbull G. Intimacy After Ostomy Surgery Guide. United Ostomy Associations of America, Inc. Revised 2009. www.ostomy.org. Accessed December 20, 2012.
Turnbull G. Sexuality after ostomy surgery. Ostomy Wound Manage. 2006;52(3):14,16.
Before discharge, a new ostomy patient and caregiver have a lot to learn, including how to empty the pouch, establish a schedule for pouch changes, measure the stoma to ensure protection from effluent, and use accessory supplies appropriately.