There’s an app for that! Here are a variety of medical apps that you might want to try. You can download them in the iTunes store, and the basic service is free.
Medscape
More than 1.4 million healthcare professionals use this app from WebMD, which includes:
• medical news
• clinical reference information, such as drugs and diseases
• medical calculators (not available for iPad).
The app is available for Android, iPad, and iPhone/iPod touch devices.
Use this app to take a photo of a wound. The app segments the image into red, yellow, and black to help with ulcer classification. You can also use the app to track changes in the wound over time. The app is available for iPad and iPhone/iPod touch devices. Note: This is free for a limited time.
The ePSS (Electronic Preventive Services Selector) app allows you to search and browse the U.S. Preventive Services Task Force recommendations on the Web or a mobile device. The app is from the U.S. Department of Health & Human Services and is available for Android, iPad, and iPhone/iPod touch devices.
This app from the University of Michigan Health System allows users to complete and store photographs of the skin. Features include:
• guidance on performing a skin cancer self-exam and full-body photographic survey
• tracking of detected skin lesions and moles for changes over time
• notifications/reminders to perform self-exams on a routine basis
• storage of photos for baseline comparisons during routine follow-up self-
exams
• informational videos and literature on skin cancer prevention and healthy skin as well as a skin cancer risk calculator function.
The app is available for iPad and iPhone/iPod touch devices.
This data storage utility app is perfect for your patients with diabetes who want all their information in one place. Users can manually enter their glucose results, carbohydrate consumption, insulin dosages, and activities, and then view the data in a free glucosebuddy.com online account. Another option is the ability to set reminders for when it’s time to check blood glucose.
The app is available for Android, iPad, and iPhone/iPod touch devices.
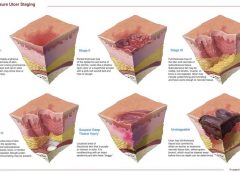
Use this app to learn more about pressure ulcer staging. It includes information about 3M pressure ulcer products.
The app is available for iPad and iPhone/iPod touch devices.
This evidence-based tool is helpful for assessing and classifying peristomal skin lesions. Click here for more information about the SACS Instrument.
The app is available for iPad and iPhone/iPod touch devices.
Do you experience chronic stress? Is your body stiff and inflexible? Does your mind seem dull and sluggish, your spirit exhausted?
Restorative yoga may help “open” your joints, ease your mind, and revive your spirit. It’s based on the concept that we’re overstimulated and don’t get enough rest. Constant stimulation activates the sympathetic nervous system, overtaxing the fight-or-flight response. The body responds by increasing cortisol and glucose production, which (along with additional unhealthy responses) raises the risk of metabolic syndrome.
Restorative yoga promotes active relaxation, helping to halt the overstimulation cycle. It promotes balance by alternately stimulating and relaxing the body, which is supported in yoga poses with such props as blankets, pillows, yoga mat, and eye covers. Research suggests restorative yoga may ease hot flashes in postmenopausal women and may promote a calm, positive mood in women with ovarian or breast cancer.
Five facets of restorative yoga
Restorative yoga takes a five-faceted approach to relieve the effects of stress. Over time, you’re likely to notice a new awareness of and appreciation for your body, mind, and spirit.
Simply put, networking is an information exchange, a forum for communicating your needs or agenda and, in return, listening and responding to others’ needs or agendas. Good networking requires emotional reciprocity, which means caring about the needs and agendas of the people you network with. Caring about others’ needs is what nurses do, so networking really shouldn’t be that difficult for a nurse.
1. Using props, restorative yoga supports the body in yoga poses, helping muscles and joints release tension and achieve muscular balance.
2. The restorative poses move the spine in all directions—flexion, extension, rotation, and lateral flexion. This enhances spinal flex-ibility, lubricates vertebrae, and strengthens the deep muscles that stabilize the spine.
3. Inverted poses, in which the feet and legs are elevated, counter the effects of gravity and promote lymph and fluid drainage to the heart.
4. The poses compress and release internal organs, cleansing them while aiding removal of cellular waste and renewing oxygen and nutrients.
5. Finally, the poses balance the body’s male (prana) and female (apana) energies.
Learning the poses
To learn the poses, consider taking a restorative yoga class. (See Finding an instructor.) Beforehand, make sure to tell the instructor about any special health concerns you have, so the instructor can modify the poses for you. Expect to bring your own blankets, pillows, eye covers, and yoga mat. The class will last from 60 to 90 minutes.
Restorative yoga typically doesn’t involve active (hatha) yoga poses, although it may include stretching poses to warm muscles and joints before the restorative poses begin. The instructor will help you use your props to make the poses right for you, and will direct you into a pose using them. Expect to stay in the pose for 5 to 10 minutes. The instructor will guide you by helping you focus on your breath and turn your attention inward. If your mind wanders and your body stays active, accept this reaction and don’t judge yourself. Over time, you’ll learn to use your breath to release tension and to focus and calm your mind.
After you hold the pose for the required duration, the instructor will help you into the next one. Generally, the class is near-silent, with minimal talking; the lights are low and music may play.
When the class ends, you may feel more relaxed and in touch with yourself. If you feel restless and jittery instead, accept your reaction. Don’t judge yourself. Try again. Give yourself the opportunity to experience something different.
Restorative yoga is just one method to renew and reconnect with your inner being. Only you can know if it’s right for you. n
Selected references
Cohen B, Kanaya A, Macer J, Shen H, Chang A, Grady D. Feasibility and acceptability of restorative yoga for treatment of hot flushes: a pilot trial. Maturitas. 2007;56(2):198-204.
Danhauer SC, Tooze JA, Farmer DF, Campbell CR, McQuellon RP, Barrett R, Miller BE. Restorative yoga for women with ovarian or breast cancer: findings from a pilot study. J Soc Integr Oncol. 2008;6(2):47-58.
Lisa Marie Bernardo is the managing member of The PIlates Centre, LLC, in Hampton Township, Pennsylvania, and adjunct faculty at Carlow University School of Nursing in Pittsburgh, Pennsylvania.
To find a certified yoga instructor in your area, check the Yoga Alliance website at www.yogaalliance.com. Restorative Yoga Teachers (www.restorativeyogateachers.com) focuses exclusively on restorative yoga. This site is operated by Judith Hansen Lasater, PhD, the leader in restorative yoga practice.
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
• Nonsterile dressings protect open wounds from contamination and absorb drainage.
• Clean aseptic technique should be used to change nonsterile dressings.
• In the event of multiple wounds, each wound is considered a separate treatment. (more…)
NPUAP releases new position statement on exposed cartilage as Stage IV ulcer
The National Pressure Ulcer Advisory Panel (NPUAP) has released a new position statement, “Pressure ulcers with exposed cartilage are Stage IV pressure ulcers,” which states that pressure ulcers with exposed cartilage should be classified as Stage IV.
NPUAP notes that although the presence of “visible or palpable cartilage at the base of a pressure ulcer” wasn’t included in Stage IV terminology, cartilage “serves the same anatomical function as bone,” so it fits into the current Stage IV definition, “Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often including undermining and tunneling.”
Medicare expenditures for diabetic foot care varies significantly by region
Medicare spending on patients with diabetes who have foot ulcers and lower extremity amputations varies significantly by region, according to a study in Journal of Diabetes and Its Complications, but more spending doesn’t significantly reduce 1-year mortality.
“Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations” examined data from 682,887 patients with foot ulcers and 151,752 patients with lower extremity amputations.
Macrovascular complications in patients with foot ulcers were associated with higher spending, and these complications in patients with amputations were more common in regions with higher mortality rates.
Rates of hospital admission were associated with higher spending and increased mortality rates for patients with foot ulcers and amputations.
“Geographic variation in Medicare spending and mortality rates for diabetic patients with foot ulcers and amputations is associated with regional differences in the utilization of inpatient services and the prevalence of macrovascular complications,” the study concludes.
Patients who develop pressure ulcers in hospital more likely to die
Medicare patients who develop pressure ulcers in the hospital are more likely to die during the hospital stay, have longer lengths of stay, and to be readmitted within 30 days after discharge, according to a study of 51,842 patients in the Journal of the American Geriatrics Society.
“Hospital-acquired pressure ulcers: results from the National Medicare Patient Safety Monitoring System Study” found that 4.5% of patients developed at least one new pressure ulcer during their hospitalization. Length of stay averaged 4.8 days for patients who didn’t develop a pressure ulcer, compared to 11.2 days for those with a new pressure ulcer.
Patients with diabetic foot ulcers may have higher risk of death
Patients with diabetes who have foot ulcers have a higher risk of cardiovascular disease and mortality, according to a meta-analysis in Diabetologia.
“The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis” notes that the more frequent occurrence of cardiovascular disease only partly explains the increased mortality rate. Other explanations may include the more advanced stage of diabetes associated with those who had foot ulcers.
A Drugs.com article about the study reported that “analysis of data from more than 17,000 diabetes patients in eight studies found that the more than 3,000 patients with a history of foot ulcers had an extra 58 deaths per 1,000 people each year than those without foot ulcers.”
The study authors emphasize the importance of screening patients with diabetes for foot ulcers so intervention can begin early, as well as lowering cardiovascular risk factors.
Access patient information on foot care from the American Diabetes Association.
Nurse’s innovation for ostomy patients could improve quality of life
An oncology nurse in Australia has developed StomaLife, an alternative to ostomy bags.
StomaLife is a ceramic appliance that eliminates the need for an ostomy bag. According to the StomaLife website, the appliance uses a magnetic implant technology that provides a “pushing force” from within the body outward in order to keep the site intact, while a second part is placed on the stoma site. A cotton gauze pad is used between the skin and the appliance to keep the site separated and to provide air circulation to the surrounding skin.
“The benefits of StomaLife to ostomy patients are continence all day, reduced skin irritation and infection, odour and sound control, leak prevention, waste material flow control and on-demand gas release,” says Saied Sabeti.
StomaLife still needs to be tested and is not yet being produced.
New laser-activated bio-adhesive polymer aims to replace sutures
The Journal of Visualized Experiments, a peer-reviewed video journal, has published “A chitosan based, laser activated thin film surgical adhesive, ‘SurgiLux’: preparation and demonstration.”
SurgiLux is a laser-activated, bio-adhesive polymer that is chitosan-based. Chitosan is a polymer derived from chitin, which is found in fungal cell walls or in exoskeletons of crustaceans and insects. This molecular component allows SurgiLux to form low-energy bonds between the polymer and the desired tissue when it absorbs light.
The technology may be able to replace traditional sutures in the clinical setting. SurgiLux polymer can achieve a uniform seal when activated by a laser and has antimicrobial properties, which help prevent a wound from becoming infected. It also maintains a barrier between the tissue and its surroundings.
SurgiLux has been tested both in vitro and in vivo on a variety of tissues, including nerve, intestine, dura mater, and cornea.
Palliative care raises patient satisfaction and reduces costs
Kaiser Permanente’s home-based palliative care program increased patient satisfaction and decreased emergency department visits, inpatient admissions, and costs, according to an innovation profile in the Agency for Healthcare Research and Quality’s Innovations Exchange.
“In-home palliative care allows more patients to die at home, leading to higher satisfaction and lower acute care utilization and costs” notes that the program uses an interdisciplinary team of providers to manage symptoms and pain, provide emotional and spiritual support, and educate patients and family members on an ongoing basis about changes in the patient’s condition.
Other components of the program include a 24-hour nurse call center, biweekly team meetings, and bereavement services to the family after the patient dies.
More research needed to determine efficacy of maggot debridement therapy
“The efficacy of maggot debridement therapy (MDT)—a review of comparative clinical trials” concludes that “poor quality of the data used for evaluating the efficacy of MDT highlights the need for more and better designed investigations.”
The authors of the article in International Wound Journal reviewed three randomized clinical trials and five nonrandomized clinical trials evaluating the efficacy of sterile Lucilia sericata applied on ulcers.
The studies found that MDT was “significantly more effective than hydrogel or a mixture of conventional therapy modalities, including hydrocolloid, hydrogel and saline moistened gauze,” but the designs of the study were “suboptimal.”
Use tool to select correct antimicrobial dressing
“Ensuring that the correct antimicrobial dressing is selected,” in Wounds International, emphasizes that dressing selection should be based on assessment of the microbial burden in the wound, the wound type, and the location and condition of the wound.
The article includes a checklist that may be helpful for deciding on the level of bacterial burden in a wound. The checklist is used to determine four levels of risk—colonized: at risk; localized infection; spreading infection; and systemic infection. Each level has a corresponding definition.
A table of antimicrobial dressings reviews the antimicrobial agent and dressing form, and the article ends with a case study.
Editor’s note: Part 1 of this series, published in the September-October issue, discussed lymphedema pathology and diagnosis. This article, Part 2, covers treatment.
Traditional treatment approaches
Traditionally, lymphedema treatment has been approached without a clear understanding of the underlying structure and function of lymphatic tissues. Ineffective traditional treatments include elevation, elastic garments, pneumatic pumps, surgery, diuretics, and benzopyrones (such as warfarin). Because many traditional treatments are still overused and some may be appropriate for limited use, it’s important for clinicians to understand these approaches.
Elevation
As a sole therapy for lymphedema, elevation of the affected part provides only short-lived results. Ever-increasing macromolecular wastes retain water against the effects of gravity. Increased interstitial colloid osmotic pressure must be addressed by interventions targeted at improving lymphatic function—not just a position change. Otherwise, lymphedema will progress. Furthermore, elevation alone is impractical, promotes deconditioning, and alters lifestyle for prolonged periods.
Elastic garments
Elastic garments prove inadequate because they attempt to treat lymphedema with compression alone. Medically correct garments are engineered with thoughtful attention to high-quality textiles and offer gradient support, which promotes proximal flow. However, without precise tissue stimulation leading to improved lymphangioactivity (lymph-vessel pulsation), macromolecular wastes can’t be removed.
Interstitial pressure increases caused by compression garments impede further fluid accumulation. When these garments are removed, the spontaneous girth increase causes an imprecise fit, and the garment rapidly leads to a countertherapeutic effect. Furthermore, compression garments don’t combat the osmotic forces generated by ever-increasing interstitial wastes. Except in patients diagnosed with stage 0 or stage 1 lymphedema, disease progression involving metaplasia ensues. Although elastic compression garments are a cornerstone of long-term management, they shouldn’t be used as a stand-alone treatment.
Pneumatic compression pump
Formerly, the pneumatic compression pump (PCP) was considered the standard of care for lymphedema. However, when inflated, the pump doesn’t increase the frequency of lymph-vessel contraction or enhance lymph capillary absorption. What’s more, accelerated fibrosis development and rapid tissue refilling occur when a PCP is removed. Also, PCP use disregards the ipsilateral territory of the excised regional nodes, effectively dumping fluid from the leg into the trunk. A PCP is appropriate only when nothing else is available, as it may worsen the patient’s condition.
Surgery
Surgical approaches to treating lymphedema involve either excisional (debulking) or microsurgical techniques. The most extensive surgical technique, the radical Charles procedure, completely debulks all involved tissue down to the muscle fascia. Split-thickness grafts are then harvested from excised skin and donor sites, and applied to the fascia to achieve so-called limb reduction.
Most debulking procedures have been applied to lower-extremity lymphedema and offer poor cosmetic results. Less radical surgeries favor long incisions, preserving the skin but excising subcutaneous edematous portions to reduce girth. Although less cosmetically alarming, these procedures effectively amputate the subcutaneous space where lymph vessels reside. Other surgical approaches are beyond the scope of this article.
Generally, surgery isn’t a good approach for any patient, as it’s linked to significant morbidity, such as skin necrosis, infection, and sensory changes. In the future, less invasive procedures may be available that yield significant improvement without these adverse effects.
Diuretics
Although diuretics are prescribed appropriately to address water-rich edemas of venous origin, they disregard the fact that lymphedema is a protein-rich edema. Long-term, high-dose diuretic therapy leads to treatment-resistant limbs, similar to those that have received intensive pneumatic compression.
Benzopyrones
Benzopyrones such as warfarin decrease swelling by combating protein accumulation in fluid. Such drugs have undergone clinical trials abroad. Their mechanism is to promote macrophage migration into interstitial fluid, as well as subsequent proteolysis. Due to significant risk of liver damage or failure, benzopyrones haven’t been approved for treating lymphedema.
Complete decongestive therapy: The current treatment approach
Currently, the gold standard for lymphedema treatment is complete decongestive therapy (CDT). Michael Foeldi and Etelka Foeldi, who originated this method, discovered a unique symbiotic relationship among five distinct modalities that addresses the challenges of lymphedema treatment. In 1989, CDT was brought to the United States by Robert Lerner and has become the mainstay of lymphedema treatment here.
CDT is a two-phase approach involving an intensive clinical effort followed by a semi-intensive home-care program geared toward autonomous management, stabilization, and continual improvement. It involves manual lymph drainage (MLD), compression bandaging, exercise, skin and nail hygiene, and self-care education. (See Phases of complete decongestive therapy by clicking the PDF icon above.)
Manual lymph drainage
A type of soft-tissue mobilization, MLD provides skin traction, stimulating superficial lymph vessels and nodes. Lymph capillaries contain large inter-endothelial inlets called swinging tips, akin to overlapping shingles. Each overlapping cell is tethered to the interstitial matrix by anchoring filaments, so that fluid increases cause immediate distention and lymph inflow. Manual skin traction using MLD promotes greater lymph fluid uptake by stretching these filamentous structures, opening the swinging tips.
MLD also provides extrinsic stimulation of the lymphangion (the segment of a lymph vessel between a distal and proximal valve), drawing fluid into the system at the capillary level and promoting flow at the vessel level toward regional lymph nodes. Usually, these segments contract and relax in a rhythmic fashion six times per minute. MLD triples this output to 18 or 20 times per minute, greatly enhancing systemic transport.
MLD requires intensive daily treatment sessions to strengthen collateral flow as a pathway to circumventing surgical or developmental lymphatic disruption. Treatment strategies further recruit more deeply situated lymphatics such as the thoracic duct, as well as lumbar trunks that empty at the juncture of the internal jugular and subclavian veins to improve global uptake. MLD thus stimulates deeper vessel angioactivity to help drain the superficial vessels that drain toward them.
Compression bandaging
Compression bandaging provides tissue support after MLD to prevent reflux, slow new fluid formation, and mechanically soften fibrotic areas. Bandaging techniques provide a high working pressure to harness the muscle and joint pumps as a propellant for lymph while resisting retrograde flow created by gravity and centrifugal forces during movement. Pure cotton materials coupled with specialized padding create a soft, castlike environment, which confines swollen tissues without constriction. By relying on high working pressure and low resting pressures to decrease limb swelling, this strategy achieves greater control over intensity (level of compression/pressure exerted), with little to no soft-tissue injury or discomfort.
The patient wears this bulky inelastic complex after each MLD treatment until the next day’s session to ensure limb-volume reduction in a stable, linear fashion. Once a plateau is reached, tissue stabilization and self-care education are the goals of additional sessions.
Exercise
Exercise always must be done with adequate support to counteract fluid formation. During the intensive CDT phase, limbs are bandaged to provide complete around-the-clock containment. Gentle exercises encourage blood flow into the muscle; during muscle contraction, this creates a favorable internal pressure that effectively squeezes the subcutaneous space between the bandage wall and muscle. Because every bandage strives to provide a gradient of support, fluid tends to drain proximally to the bandage—in most cases, to the trunk.
Skin and nail hygiene
Without intact, well-hydrated skin, cellulitic infections occur in many lymphedema patients whose immune response has been diminished by regional lymphadenectomy or inherited deficiencies. To prevent infection caused by avoidable external events, patients receive clear guidelines to reinforce appropriate behavior. As most cellulitis results from resident skin pathogens (streptococci and staphylococci), maintaining a low skin pH helps control colonization. Ways to avoid recurrent infections include maintaining an acid mantle on the skin using low-pH-formulated lotions and avoiding injury from daily tasks that may scratch, puncture, burn, or abrade the skin. Patients should receive lists of self-care precautions at the time of treatment.
Self-care education
Because lymphedema is a chronic condition, patients must receive self-care education for daily management to avoid lymphedema destabilization, which can lead to tissue saturation and subsequent skin changes. Therapists must provide patients with appropriate self-care tools and knowledge to maintain adequate treatment results. Teaching topics include how to apply and remove compression garments and bandages and how to exercise safely, preserve skin integrity, monitor for infection, and respond appropriately to infection and significant changes in limb mobility.
An underrecognized and mistreated problem
Lymphedema remains an underrecognized and mistreated condition, even though CDT yields safe, reliable results. Early detection, accurate staging, proper diagnosis, and appropriate treatment can slow the inevitable progression of lymphedema. Wound care specialists should adapt wound therapy to address not just the wound but the edematous environment responsible for delayed wound resolution.
Selected references
Al-Niaimi F, Cox N. Cellulitis and lymphedema: a vicious cycle. J Lymphoedema. 2009;4:38-42.
Browse N, Burnand KG, Mortimer PS. Diseases of the Lymphatics. London: Hodder Arnold; 2003.
Casley-Smith JR, Casley-Smith JR. Modern Treatment for Lymphoedema. 5th ed. The Lymphoedema Association of Australia; 1997.
Cooper R, White R. Cutaneous infections in lymphoedema. J Lymphoedema. 2009:4:44-8.
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. Consensus Document of the International Society of Lymphology. Lymphology. 2009 Jun;42(2):51-60.
Leduc A, Bastin R, Bourgeois P. Lymphatic reabsorption of proteins and pressotherapies. Progress in Lymphology XI. 1988:591-2.
National Lymphedema Network Medical Advisory Committee. Position Statement: Lymphedema Risk Reduction Practices. Revised May 2012. http://www.lymphnet.org/pdfDocs/nlnriskreduction.pdf. Accessed September 5, 2012.
Pappas CJ, O’Donnell TF Jr. Long-term results of compression treatment for lymphedema. J Vasc Surg. 1992 Oct;16(4):555-62.
Whittlinger H. Textbook of Dr. Vodder’s Manual Lymphatic Drainage. Vol 1. 7th ed. New York, NY: Thieme; 2003.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
In health care, we frequently use the terms formulary and protocol interchangeably even though they have different meanings. A formulary is an official list of available dressings, products, and medications. A protocol is a roadmap or guideline on how to use the formulary.
Formularies became popular several years ago when reimbursement changed to bundling and wound-product costs were included in the routine cost of care rather than separately billable. In an effort to control costs, hospitals, home health agencies, and long-term care facilities began exclusive partner agreements with supply and buying groups. (“You use our products exclusively and we’ll give you a huge discount on cost.”)
A good formulary not only can help save money. It can also assist in streamlining care delivery, reducing waste, and directing treatment decisions. But on the flip side, using formularies can have disastrous results. I realized this last week while speaking on the phone with a wound clinician who’d called to ask for wound treatment ideas for a hospice patient. As she described the situation, it became apparent that the patient’s symptoms definitely pointed to high levels of bacteria in the wound. As I began sharing recommendations for treatment ideas, she kept responding: “Nope. Can’t use that, not on our formulary.” “Nope, not on formulary.” The only options available on her hospice formulary were hydrocolloid, hydrogel, or foam dressings, none of which had antibacterial properties.
Providing an appropriate standard of care shouldn’t be dictated by a formulary, and choosing substandard care just because the patient is in hospice isn’t acceptable or appropriate. Evidence-based guidelines, wound characteristics, underlying complications, and patient care goals should dictate management and treatment.
To ensure your formulary is adequate, determine if it includes a variety of product categories, and negotiate the ability to go off formulary if needed. Although cost control is essential, clinicians need access to products and therapies that yield positive outcomes. One size doesn’t fit all in wound care.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Before discharge, a new ostomy patient and caregiver have a lot to learn, including how to empty the pouch, establish a schedule for pouch changes, measure the stoma to ensure protection from effluent, and use accessory supplies appropriately.
The most basic principle of healing a wound is to determine the cause—and then remove it. This is easier said than done, as many wounds have similar characteristics and we don’t always know all the facts leading up to the wound.
The process has been unnecessarily complicated by the recent pressure (no pun intended) to avoid at all costs calling a pressure ulcer a pressure ulcer. I use the term “unnecessarily” because it doesn’t matter what it’s called—a pressure ulcer, decubitus, “de-cube,” or bedsore—because in the end, the general idea is it’s bad news.
So what’s behind the desire to avoid calling it a pressure ulcer? First, a pressure ulcer has traditionally been equated to poor nursing care. As Florence Nightingale, the “Mother of Nursing,” wrote:
“If he has a bedsore, it’s generally not the fault of the disease, but of the nursing.”
No one likes to feel that he or she gave poor care, and as more hospital complications data are available to the public, reports of complications such as pressure ulcers affect people’s perceptions—right or wrong—about the care a hospital delivers.
The second reason gets at the “at all costs” part of the desire. The recent attention given to Medicare’s “present on admission” rule and “never” events has
elevated pressure ulcers high up the chain of “no-no’s” and put the hospital at risk for nonreimbursement. And many private insurers have followed Medicare’s lead in denying coverage for pressure ulcers that occur in the hospital. Unfortunately, all the focus on reimbursement is beginning to challenge even the best wound care experts, who simply want to get the patient’s wound healed.
Pressure from upper management has resulted in experts trying to bargain and rationalize their way out of calling it what it is (a pressure ulcer), instead calling it a bruise, not a deep-tissue injury. Or saying, “This is a shearing ulcer, not a pressure ulcer.” Or, my favorite: “It’s not an ischial pressure ulcer but a diabetic ulcer because the patient is a diabetic.” Wound care experts are being forced to question and doubt themselves because money, quality assurance, and reputation are on the line when an in-house wound is labeled a pressure ulcer.
Like crime scene investigation, determining wound etiology requires us to gather all the facts. Once the facts are in, systematically comparing and contrasting the clinical findings aids differential identification to pin down the type of wound present. It’s important that we assess and investigate all the following when searching for the cause:
• patient’s medical history
• recent activities (such as surgery, extensive X-rays, or long emergency-
department waits)
• comorbidities
• specific wound characteristics, such as location, distribution, shape, wound bed, and surrounding skin.
Naming the wound is an important first step in intervening. If the wound is caused by pressure, call it a pressure ulcer and jump into action. Remove the cause, heal the wound, and prevent further breakdown. Don’t let yourself be influenced by those who aren’t experts in wound care.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
Sherry stands nervously in the doorway, watching several dozen people chat each other up. The sound of her heartbeat threatens to drown out the conversational din. For the people on the other side of the door, this is a networking event. But for Sherry, it seems like a swap meet of business cards.
If Sherry sounds like you, know that you’re not alone. For many people, networking means an awkward evening spent cradling a wine glass in one hand, thrusting a business card at someone with the other hand, and exchanging small talk.
“Hello. My name is…”
Networking is one of the most overused, misunderstood, and underestimated terms in the business world (and yes, that includes health care). Actually, networking is just a newish term for an activity that has been around for millennia. Savvy people have always seen the wisdom of seeking out others who can help them get ahead.
Simply put, networking is an information exchange, a forum for communicating your needs or agenda and, in return, listening and responding to others’ needs or agendas. Good networking requires emotional reciprocity, which means caring about the needs and agendas of the people you network with. Caring about others’ needs is what nurses do, so networking really shouldn’t be that difficult for a nurse.
Think of networking as a great opportunity to make yourself known, gather critical information, and meet people who can help you now and in the future. Through networking, you can make contacts that further your agenda—whether it’s to find
a mentor, get information on a program you’re interested in, change jobs, or advance from your current position.
Networking isn’t just who you know, but who knows you. If you listen to other networkers and give them the resources they seek (as by introducing them to key people or sharing valuable information), they’ll become grateful—and indebted—networking colleagues.
Set a networking goal
At a networking event, the idea isn’t to meet the greatest number of people possible in one evening. It’s to meet the “right” people—those who can help you realize your goal.
When approaching a networking situation, ask yourself, “What do I want this experience to lead to?” You’ll be much more effective if you have a laser-focused goal. The most successful networker isn’t the one who walks away with the most business cards. It’s the one who leaves with the contacts and information he or she had been seeking.
A tale of two networkers
To demonstrate this point, let’s take the case of two wound care specialists, Myrna and Doris—colleagues who’ve carpooled together to a meeting of their professional organization.
Myrna arrives with an agenda and a plan for the evening: She wants to develop a wound care speakers bureau to boost the community profile of staff at her facility. She seeks out several speakers, who give her valuable tips on how to market her expertise. She also shares her vision of a speakers bureau with attendees from other facilities—and is surprised by the support and tips they offer. She leaves the meeting with valuable information that can further her vision. On the way home, she jots down a reminder to send one of the people she met an article he might find helpful. She also makes notes about what she learned tonight, so she can follow up that week. Clearly, Myrna’s networking has been effective.
Doris, on the other hand, goes to the meeting unfocused. She meanders about the room speaking with a lot of attendees, and exchanges a few business cards. But the “Where-do-you-work?” conversations that ensue provide little insight. Although she enjoys the meeting somewhat, she has accomplished little. That’s understandable, as she set out with no goals. She might have been better off spending the night watching television.
Networking etiquette
To succeed at networking, learn networking etiquette. Rule #1: Turn off your cell phone—or at least put the ringer on vibrate. If you absolutely must take a phone call, discreetly leave the room.
More etiquette advice:
• Wear your name tag on your left lapel so you don’t block your name when shaking hands. If you fill out the name tag yourself, print clearly so your name and title are visible from about 5 feet away. That way, others won’t need to squint at your chest to read your name.
• Keep your handshake firm and friendly. Don’t hang on, and don’t pump! Remember to make eye contact, and smile.
• Keep breath mints handy. Networking usually takes place around drinks and food, and the first thing that greets a new contact shouldn’t be the garlic and onion dip.
• Keep your business cards handy (a business card holder is best), but don’t throw them at everyone you meet. Hand your business card to a contact so it’s right side up and facing that person. When someone hands you a business card, take a moment to look at it; then say thank you and carefully put it away. It’s disrespectful to deface a business card, so don’t write on the back of it.
What happens next?
Okay—you’ve set an agenda, attended the networking event without violating etiquette, and made some good contacts. Now what? This is where many people drop the ball. They fail to follow through on the contacts they make and the information they gain. They simply shove the contacts’ business cards into a Rolodex, where they will sit forgotten.
Instead of letting business cards collect dust, develop a system that helps you follow through with your contacts—whether it’s an electronic tool, a simple calendar notation, or a color-coded filing system. Jot down contact information on each
person you met, along with a summary
of your conversations, when you need to follow up, and so forth. Make the system work for you.
Next, follow through with appropriate communication. Send handwritten thank-you notes to the contacts who gave you valuable information or resources—for instance, those who introduced you to a key player or offered to make a phone call on your behalf. If possible, your note should mention how that information worked out for you. (See Seven steps to effective networking by clicking the PDf icon above.)
In the coming weeks, months, or years, keep these relationships alive and thriving by sending tips or information to each contact. If you see a newspaper article or Internet story about a topic a particular contact was interested in, send it to him or her. This shows you’re thinking about that person, and conveys your generosity and willingness to continue a reciprocal relationship.
Make it happen
Networking opportunities can happen anywhere. Don’t wait for them—create them. Pinpoint your goal, identify the key people who can help make it happen—and then network! It’s as simple as picking up the phone, sending an e-mail, or meeting over lunch. With a little effort, networking can be an enjoyable and valuable career resource.
Joan C. Borgatti, MEd, RN, is the owner of Borgatti Communications in Wellesley Hills, Mass., which provides writing, editing, and coaching services. You may e-mail her at [email protected].
Here are a variety of resources related to quality that wound care clinicians may find valuable.
Home Health Quality Improvement National Campaign
If you are interested in home care, you’ll want to visit The Home Health Quality Improvement (HHQI) National Campaign’s website. HHQI is a grassroots project of the Centers for Medicare & Medicaid Services designed “to unite home health stakeholders and multiple health care settings under the shared vision of reducing avoidable hospitalizations and improving medication management.”
The many available free resources on the campaign’s website include:
• webinars; for example, “Hospital Readmissions and the Role of Home Care”
• best practice innovation packages, including ones on medication management and fall prevention.
You must register to obtain some of the resources.
Reducing Avoidable Readmissions Effectively (RARE) is a campaign in Minnesota that is working with hospitals and care providers to prevent hospital readmissions within 30 days of discharge.
Even if you aren’t in Minnesota, you can access resources such as a webinars. Past webinars include “Involving Patients and Families in Reducing Avoidable Readmissions” and “Home Care and Reducing Hospital Readmissions.”
You can also download “Recommended Actions for Improved Transitions,” which covers five key areas: patient and family engagement and activation, medication management, comprehensive transition planning, care transition support, and transition communication.
Effective communication is essential for any quality initiative to be successful. TeamSTEPPS is a teamwork system that improves communication through train-ing and tools. The Agency for Healthcare Research and Quality and the Defense Department have teamed up to provide
resources for implementing Team STEPPS. Tools include:
• Core TeamSTEPPS Training Curriculum Materials
• TeamSTEPPS Rapid Response Systems (RRS) Training Module
• TeamSTEPPS Teamwork Perception Questionnaire
• Pocket Guide that summarizes TeamSTEPPS principles in a portable, easy-
to-use format.
The educational materials contain information that clinicians can integrate into their practice. Video vignettes illustrate how failures in teamwork and communication can place patients in jeopardy and how successful teams can work to improve patient outcomes.
You can order free TeamSTEPPS materials, which are available online.
The Institute for Healthcare Improvement is an independent, not-for-profit organization that focuses on testing new models of care, disseminating best practices, and building the will to change to improve health care.
Among the many resources on the website:
• tools such as “Self-Management Toolkit for People with Chronic Conditions and Their Families”
• useful publications
• white papers such as “Using Care
Bundles to Improve Health Care
Quality”
• case studies of successful strategies
• audio and video broadcasts
• links to other helpful websites.
By Nancy Morgan, MBA, BSN, RN, WOC, WCC, CWCMS, DWC
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
• Semipermeable polyurethane foam dressing
• Nonadherent and nonlinting
• Hydrophobic or waterproof outer layer
• Provides moist wound environment
• Permeable to water vapor but blocks entry of bacteria and contaminants
• Available in various thicknesses with or without adhesive borders
• Available in pads, sheets, and cavity dressings (more…)