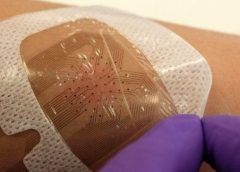
Smart bandages which can detect how well a wound is healing and send a progress report to the doctor will be trialled within the next year, scientists have said. The dressings are fitted with tiny sensors which can pick up blood clotting, or spot infections, and wirelessly send data back to a clinician. Swansea University, which is hoping to trial the bandages within 12 months, said the new technology could offer a personalised approach to medicine.
Currently patients with wounds are advised to return to the doctor in a certain amount of time. But each case may need a longer time to heal, or may have become infected before the visit. (more…)
ROLLA, Mo.–(BUSINESS WIRE)–ETS Wound Care LLC, an Engineered Tissue Solutions (ETS) subsidiary focused on commercializing next generation wound care solutions, announced MIRRAGEN™ Advanced Wound Matrix was cleared by the United States Food and Drug Administration (FDA) for treatment of acute and chronic wounds. MIRRAGEN™ is a fully resorbable borate glass matrix comprised of fibers and beads proven to be highly effective in wound care management.
MIRRAGEN™ represents a breakthrough discovery for chronic and acute wound management due to its unique borate-based fiber matrix. MIRRAGEN™ is packed into wounds to manage and control wound fluids, while the resorbable matrix provides an environment for optimal wound healing. To learn more about the technology, click here. (more…)
BY: NANCY MORGAN, RN, BSN, MBA, WOCN, WCC, CWCMS, DWC
What exactly is wound exudate? Also known as drainage, exudate is a liquid produced by the body in response to tissue damage. We want our patients’ wounds to be moist, but not overly moist. The type of drainage can tell us what’s going on in a wound.
Let’s look at the types of exudates commonly seen with wounds. (more…)
There are few absolutes in my universe. I know that my youngest daughter will gleefully and with full malice (but humorously presented) find something to torment me about every time I see her; referrals from family practice docs arrive well marinated in multiple antibiotics with nary a diagnosis in sight (save for the ubiquitous “infection”); and that regardless of what I recommend, offer, beg, plead, or cajole, that the patient has the complete and total power to make their decisions regarding their care and who provides it. Unless they are deemed by multiple authorities to be incapable of making a decision, until the appropriate paperwork or an emergency situation exists mandating immediate lifesaving action, the ball bounces squarely in their court…or so I thought. (more…)
For those of you not as familiar with the Hoosier State as you should be, I used to think it was essentially paradise. Jim Nabors of Gomer Pyle fame is our ubiquitous, tuneful icon with his always well-received “Back Home in Indiana” as a mantra to that source of pride. Our former Governor “My Man” Mitch Daniels was a genius who, using a combination of intelligence, common sense and the persuasive powers of a midwest Svengali, created an economic model that our neighbors can only lust after. Our medicolegal climate is among the best in the US and well it should be. However, while there are some extraordinary caregivers and facilities here, a recent US News and World Report curiously showed that almost none of our hospitals made their “Best of” lists in any category. That is not to say there is bad care but to not have a single facility in an entire state even achieve an honorable mention gives one pause to reflect. The State newspapers were notoriously quiet on this concerning fact despite their trumpeting of who does what well, when and where. (more…)
I have several letters after my name. The two that say “DO” indicate that I have the training of a physician and the requisite education and responsibilities that uphold those letters. They should mean to patients that my ultimate goal is to offer (and provide when the fates allow) the entire spectrum of medical care referable to what I am good at and what they came to seek solace for. Nothing less and if I keep my ego in check, certainly nothing more. Patients run the gamut of their perception of the medical field. But like the old sales nemesis called “Bait and Switch”, what is offered on the sign all too often does not truly match what is seen on the shelves. Arrogant people are that way because they are good at what they do and not afraid to tell others. As a child, we are told to let others brag about us but failing to let people know what we can and can’t do is integral to our patients’ survival and our success. The problem is that the glitz and glamour of being a healer all too often clouds our success. Some time ago, I blogged about the pseudo-utilitarianism of all those so-called “Wound Certification” Exams. At first blush, these seem to be the key to health, wealth, omniscience and outcomes equaled only by those wound care management companies. (more…)
I recently saw an ad for a pending lecture at a national conference that piqued my interest much like “deflate-gate”. The title of this lecture horrifically touted that Amputation need not be considered failure. As a full time wound care doc, I work to identify those conditions that place patients at risk of all consequences both limited and catastrophic. We use the catchy title of “Limb Preservation”. We start the process by engaging in the unusual behavior of making definitive diagnoses, then systematically address them in as comprehensive manner as possible. I am proud to tell you that while there are occasions in which a terminally damaged digit is lost, that we have rarely sacrificed the greater part of a foot and more, have had only 3 lower extremity amputations in the last 5 years on patients who’s care remained exclusively with us. Of course, when a patient for whom we have created and implemented a “Limb Pres” care plan is taken out of our system (usually via a hospitalization for a reason other then the lower extremity problem), the facility forces that be unfortunately but infrequently demonstrate their inadequacy and paranoia by gang-harangueing the patient and family. They are lambasted with lurid tales of the condition marching up the leg engulfing the foot, knee, torso, and brains much like a flesh-eating PacMan. The patient’s confidence now neutered has little chance against this persistent onslaught of inadequacy and so, much like the Queen song, “Another One Bites The Dust”. (more…)
I remain absolutely amazed that there are so many people doing the same thing and yet doing it so completely different. Depending on where a patient’s wound care and orders originate from, the care I try to translate from that starting point is always a combination of dressing regimens worthy of computer code in their simplicity. The only thing usually missing is the diagnosis. It’s as though they come from an identical planet in an alternate universe.
The issue is that there is the complete dissociation of what is done for a given wound care problem in one practice setting versus another. Having stayed as far away from hospital-based wound care as possible, I continue to be amazed by hospital wound teams touting their expertise while using two to three times a day dressing changes and therapies that are the antithesis of any identifiable evidence. They actually expect entities receiving their cases (including home healthcare agencies, LTAC, skilled facilities, and others) to copy the identical care scenario regardless of their widely variable situations. In fact, the only constant is the patient and his or her condition. (more…)
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make.
Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled procedures and herbal treatments to heal wounds, including xenografts (skin from another species). The practice of applying allografts (human cadaver skin) to wounds was first documented in 1503. In 1871, autologous skin grafting (skin harvested from the the person with the wound) was tried. Next came epithelial- cell seeding, which involves scraping off the superficial epithelium of healthy skin and transplanting the cells onto the wound. (more…)
Herpes zoster (HZ, also called shingles) is a painful condition that produces a maculopapular and vesicular rash. Usually, the rash appears along a single dermatome (band) around one side of the body or face.
In most cases, pain, tingling, burning, or itching occurs a few days before the rash. Next, blisters form, scabbing over in 7 to 10 days. In rare cases, the rash is widespread, resembling varicella zoster (VZ, or chickenpox) rash. Pain can range from mild to severe and may be dull, burning, or gnawing. It may last weeks, months, or even years after the blisters heal. Shingles on the face may impair vision or hearing. (more…)
Herpes zoster (HZ, also called shingles) is a painful condition that produces a maculopapular and vesicular rash. Usually, the rash appears along a single dermatome (band) around one side of the body or face. In most cases, pain, tingling, burning, or itching occurs a few days before the rash. Next, blisters form, scabbing over in 7 to 10 days. In… read more
The National Pressure Ulcer Advisory Panel (NPUAP) describes support surfaces as “specialized devices for pressure redistribution designed for management of tissue loads, microclimate, and/or other therapeutic functions.” These devices include specialized mattresses, mattress overlays, chair cushions, and pads used on transport stretchers, operating room (OR) tables, examination or procedure tables, and gurneys. Some support surfaces are part of an integrated…
Herpes zoster (HZ, also called shingles) is a painful condition that produces a maculopapular and vesicular rash. Usually, the rash appears along a single dermatome (band) around one side of the body or face. In most cases, pain, tingling, burning, or itching occurs a few days before the rash. Next, blisters form, scabbing over in 7 to 10 days. In…
As a wound care expert, you’re probably consulted for every eruption, scrape, and opening in a patient’s skin. Occasionally during a patient assessment, you may scratch your head and ask yourself, “What is this? I’ve never seen anything like it.” Most wound care experts want to help heal everyone, and most of us love a challenge. But when should we…
Chronic venous leg ulcers (CVLUs) affect nearly 2.2 million Americans annually, including an estimated 3.6% of people over the age of 65. Given that CVLU risk increases with age, the global incidence is predicted to escalate dramatically because of the growing population of older adults. Annual CVLU treatment-related costs to the U.S. healthcare system alone are upwards of $3.5 billion,…
General characteristics Document if the diversion is an intestinal or urinary ostomy, whether it’s temporary or permanent, and the location— abdominal quadrant, skin fold, umbilicus. (See Descriptor reference.)
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make. Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled…
It’s been a stressful day at work—nothing new. One confused patient pulled off her ostomy bag, you’re having difficulties applying negative-pressure wound therapy on another, and a third patient’s family is
angry with you. We all experience stressful days, but unfortunately, sometimes we take our stress out on each other. Too often, this ineffective way of identifying and managing stress leads nurses to engage in lateral violence. (more…)