Antibiotics and conservative surgery yield similar outcomes in patients with diabetic foot osteomyelitis
A study in Diabetes Care finds that antibiotics and surgery have similar outcomes related to rate of healing, time of healing, and short-term complications in patients who have neuropathic forefoot ulcers and osteomyelitis, but no ischemia or necrotizing soft-tissue infections.
No matter where you work or who your distributors are, ensuring the patient has sufficient ostomy supplies can be a challenge. Whether you’re the nurse, the physician, the patient, or the family, not having supplies for treatments can heighten frustration with an already challenging situation, such as a new ostomy. Here’s how to reduce the chance of experiencing frustrations related to ostomy supplies. (more…)
By Gail Hebert, RN, MS, CWCN, WCC, DWC, LNHA, OMS; and Rosalyn Jordan, BSN, RN, MSc, CWOCN, WCC, OMS
Imagine your physician has just told you that your rectal pain and bleeding are caused by invasive colon cancer and you need prompt surgery. She then informs you that surgery will reroute your feces to an opening on your abdominal wall. You will be taught how to manage your new stoma by using specially made ostomy pouches, but will be able to lead a normal life.
Like most people, you’d probably be in shock after hearing this. More than 700,000 people in the United States are living with ostomies. Every year, at least 100,000 ostomy surgeries are done, preceded by a conversation much like the one above. So how do patients recover from the shock of learning about their pending surgery—and then return to a full life? (more…)
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
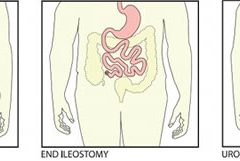
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Before discharge, a new ostomy patient and caregiver have a lot to learn, including how to empty the pouch, establish a schedule for pouch changes, measure the stoma to ensure protection from effluent, and use accessory supplies appropriately.
Every year, thousands of people of all ages have ostomy surgery in the United States. That means no matter where you work, you’re likely to care for patients with new ostomies and teach them to care for themselves. (See Why patients need ostomy surgery by clicking the PDF icon above.)
These patients present two challenges: staying up-to-date on ostomy equipment and procedures and having only 3 to 5 days after surgery to teach basic ostomy care to patients who are unlikely to be physically or emotionally ready to learn. This review and update of ostomy care should help you meet both challenges. Let’s start with the common types of stomas and ostomies.
Reviewing stoma types
The three common types of stomas are the end stoma, loop stoma, and double-barrel stoma. The patient’s surgeon decides on the most appropriate type based on the disease or injury, the amount of intestine available, and the patient’s health status.
To create an end stoma, the most common type, a surgeon creates a small opening in the abdominal wall, then resects the intestine and pulls it through the opening. Next, the surgeon turns the end of the intestine onto itself—somewhat like cuffing a sock—and sutures the stoma to the skin. Next to the stoma, the surgeon may create a mucous fistula, which secretes mucus from the nonfunctioning portion of the intestine.
A loop stoma is usually created for a temporary ostomy. The surgeon creates a small opening in the abdominal wall and pulls a loop of intestine through it. With an external rod or bridge placed under the loop to keep it from slipping back into the peritoneal cavity, the surgeon cuts the top of the loop to form the apex of the stoma. Next, the surgeon everts the intestine around the opening and sutures the stoma edges to the skin. After a few days, the rod is removed, and the stoma stays above skin level on its own. Double-barrel stomas aren’t common in adults, but they are used frequently in neonates. For this type, a surgeon cuts through the bowel to create two separate end stomas, one to evacuate stool and the other to evacuate mucus. The two stomas can be placed next to each other, so one pouching system can be used for both. If the stomas are further apart, the patient may need two pouches. If mucus secretions are slight, you may be able to apply a nonadherent dressing after gently cleaning the stoma and peristomal skin, instead of using a pouch.
An ideal stoma protrudes above the skin surface and has a flat peristomal skin surface that allows the ostomy barrier to adhere to it. (See Characteristics of an ideal stoma by clicking the PDF icon above.) A healthy stoma is red and moist and looks like gum tissue. In fact, the entire alimentary canal from mouth to anus has the same type of tissue. Keep in mind that while cleaning a stoma, you’ll commonly see a small amount of bleeding, just as your gums may bleed when you brush your teeth too vigorously. If you note excessive bleeding, report it immediately.
Reviewing types of ostomies
The three most common types of ostomies you’ll see are a colostomy, an ileostomy, and a urostomy.
A surgeon creates a colostomy by making an opening in the large intestine and connecting it to the stoma. The location of the surgical opening will affect the consistency of the stool exiting the body through the stoma: The lower the opening, the firmer the consistency. A colostomy produces flatus because of the high bacterial content in the large intestine. A colostomy can be temporary or permanent, depending on the diagnosis and the patient’s ability to heal.
To create an ileostomy, a surgeon makes an opening in the small intestine and forms a stoma. Patients with ileostomies are prone to dehydration because a large amount of enzymatic fluid is discharged through the ileostomy instead of being absorbed in the disconnected large intestine. Teach your patient to be alert for the signs and symptoms
of dehydration—thirst; decreased urination; darker, concentrated urine; warm, flushed skin; fever; and malaise. Also, warn the patient to keep enzymatic effluent off the skin because it can quickly cause skin breakdown. As with a colostomy, an ileostomy may be temporary or permanent.
To create a urostomy, a surgeon removes the diseased bladder and uses a portion of resected small intestine to create a conduit. The ureters, which were connected to the bladder, are sutured into the resected small intestine so urine can exit the body through the stoma. Urostomies are permanent.
Choosing the right pouching system
An ostomy pouching system has two parts: an adhesive barrier that attaches to the skin around the stoma and a pouch connected to the barrier that collects effluent. Determining the right ostomy pouching system for your patients will depend on their needs and preferences. Let’s look at some of the important choices.
A pouching system may come in one or two pieces. With one-piece systems, the barrier (also called the wafer, flange, or baseplate) and pouch come as a single unit. (See One- and two-piece ostomy pouching systems by clicking the PDF icon above.) One-piece systems are easier to apply and more flexible. Plus, they’re flatter and thus more discreet.
With two-piece systems, the barrier and pouch are separate components that must be attached. Depending on the product, the patient may need to press the pouch onto the barrier or use a locking ring mechanism or an adhesive coupling system. Two-piece systems allow the patient to remove the pouch without removing the barrier. Also, a patient can apply a smaller pouch, such as a stoma cap or close-ended pouch, before exercise or intimate relations.
Today, ostomy pouching systems offer many options that weren’t available just a few years ago—options such as built-in, varying levels of convexity and integrated closures. Skin-friendly barriers now eliminate the need for accessory products, such as skin prep, ostomy powder, and stoma paste. By knowing the new options, you can help simplify the pouch application process for your patient and increase patient satisfaction.
Selecting barriers
Barriers may be cut-to-fit or precut. Cut-to-fit barriers are used during the postoperative period while the stoma size is changing and for oval or irregularly shaped stomas. Precut sizes are convenient for round stomas after they stabilize.
The choice of a barrier also depends on abdominal contours and the effluent consistency. A standard-wear barrier is appropriate for thicker output. An extended-wear barrier is better for loose or watery output and for problematic ostomies.
Convex barriers can be used to push down the peristomal skin and help the stoma project into the pouch. These barriers help ensure that the effluent goes into the pouch and not between the skin and the barrier, causing leakage.
For ostomies that are difficult to manage and frequently leak, you may select an ostomy belt. This device helps secure a convex pouching system by increasing its pressure. The plastic hooks at the end of the belt attach to the belt loops of the pouching system. Depending on the manufacturer, the belt loops may be on the barrier or the pouch.
Selecting pouches
Pouches can be transparent or opaque. Transparent pouches allow you to see the stoma postoperatively and allow patients to watch as they place the pouch over the stoma. Opaque pouches, of course, have the advantage of concealing the effluent.
Some pouches have filters. Colostomy patients usually prefer filtered pouches because they eliminate the need to burp the pouch to remove gas. Ileostomy output is usually watery, so the charcoal filters may get wet and quit working.
The appropriate type of pouch closure also varies, depending on the type of output and the patient’s needs and preferences. A patient with a colostomy or ileostomy needs a drainable pouch. Newer clamps and integrated closures can make closing the pouch easier for the patient.
Close-ended pouches are available for patients who empty their pouch once or twice a day. Reimbursement guidelines for Medicare, which most insurance companies follow, allow 60 close-ended pouches a month. Thus, someone who empties once or twice a day will have enough pouches.
Patients with urostomies use pouches with spigots on the end to allow for urine drainage.
Urostomy pouches can be connected to a continuous urinary drainage bag at bedtime or to a leg bag during the day for those in a wheelchair.
Dealing with complications
Report the following postoperative complications to the surgeon and the ostomy clinician caring for the patient:
• allergic reaction
• candidiasis
• contact dermatitis
• folliculitis
• ischemic or necrotic stoma
• mechanical irritation
• mucocutaneous separation
• parastomal hernia
• prolapse.
Many complications result from surgical technique or the patient’s disease status, but complications also result from an incorrect fit or an ostomy that frequently leaks. To determine why and where leakage occurred, examine the back of the barrier. If leakage results from a flush or recessed stoma or an irregular surface around the stoma, the patient may need a convex barrier. Or the patient may need a convex barrier and an ostomy belt.
Remember that a firm abdomen requires a soft, flexible barrier that conforms to the abdominal contours. A soft belly, on the other hand, may need the rigidity of a convex barrier to help the stoma empty into the pouch.
For weepy, extremely denuded skin, apply ostomy powder, brush off the excess, and dab an alcohol-free skin sealant, such as No-Sting by 3M, on the area. Allow the area to air-dry before applying the barrier.
Discharge planning and patient teaching
Because the postoperative length of stay is short, start preparing for discharge and teaching the pouch-change procedure at your first hospital encounter with the patient. Teaching the patient at each encounter creates a continuum of care throughout hospitalization and recovery. If possible, include the caregiver. (See Teaching your patient to change an ostomy pouch by clicking the PDF icon above.) Before discharge, give the patient two or three ostomy pouches to take home, step-by-step printed instructions on applying pouches, a list of supplies the patient will need, and a list of ostomy product suppliers in the area.
Also, teach the patient about complications, activity, diet, and drug therapy and provide the names of local support groups. (See Finding support by clicking the PDF icon above.)
Complications at home
Tell the patient to call the physician if any of the following occurs: fever, increased pain or discomfort, diarrhea, dehydration, or signs and symptoms of infection at the surgical site. The patient should also call the physician if there’s no output from the stoma for more than 24 hours.
Patients with urostomies who develop the following signs and symptoms may have a urinary tract infection: fever, chills, abdominal or retroperitoneal pain, and bloody, cloudy, or foul-smelling urine. Clear urine with mucus shreds is normal.
Increasing activity
Explain that after surgery the patient should feel a little bit stronger every day. Teach the patient to alternate rest and activity periods and to increase the activity period a little each day while building endurance. Refer the patient to the physician for clearance to resume exercise and sexual relations.
Dietary considerations
After ostomy surgery, your patient will start on a clear liquid diet and progress to a normal, preoperative diet. The patient should reintroduce one food at a time to help determine if it’s well tolerated. High-fiber foods should be introduced slowly.
Tell your patient to expect his or her body to tolerate the food as it did before surgery: if onions caused gas before surgery, they will do so after surgery, too, but the stoma will expel the gas. Make the patient aware of other gas-forming foods, such as hard-boiled eggs, spicy foods, fish, dried beans, carbonated beverages, and beer.
Tell the patient to chew food well and to drink plenty of liquids, which will prevent blockage. Explain the importance of hydration to avoid constipation, dehydration, and urinary tract infection. To prevent dehydration, ileostomy patients who are not on fluid restriction should drink 64 ounces of fluid a day. Teach these patients to replace fluids by drinking a glass of water every time they empty their pouches.
Drug therapy
Tell the patient to adhere to the prescribed regimen and to call the physician before using any new drugs. Instruct patients with ileostomies not to take laxatives because they may become dehydrated. These patients should tell their pharmacist that they have an ileostomy, so the proper form of prescription drugs can be ordered. Extended-release tablets will not break down in time and may be found in the pouch.
Rewarding work
Keeping up with the changes in ostomy equipment and care and teaching new ostomy patients the skills they need can be challenging. But helping these patients regain the confidence and learn the skills they need to improve their quality of life makes the rewards much greater than the challenges.
Selected references
Colwell J. Principles in stoma management. In: Colwell JC, Goldberg MT, Carmel JE, eds. Fecal and Urinary Diversions Management Principles. St. Louis, MO: Mosby; 2004:240-262.
Discharge Planning for a Patient with a New Ostomy: Best Practice for Clinicians. Glenview, IL: Wound, Ostomy and Continence Nurses Society; 2004.
Hampton BG, Bryant RA. Ostomies and Continent Diversions: Nursing Management. St. Louis, MO: Mosby; 1992.
McCann E. Common ostomy problems. In: Milne C, Corbett L, Dubuc D. Wound, Ostomy, and Continence Nursing Secrets: Questions and Answers Reveal the Secrets to Successful WOC Care. Philadelphia, PA: Hanley & Belfus, Inc; 2004.
The Sarah Cole Hirsh Institute for Best Nursing Practices Based on Evidence. State of the evidence review hospital to home: Planning the transitions. 2000; Cleveland, OH.
Goranka Paula Bak is an Ostomy Sales Territory Manager for Coloplast Corporation.
Consider these solutions to three common mistakes. Stepping into a formal leadership role is exciting. Whether it’s your first supervisor or manager role or an interim position with the potential to become permanent, the new responsibilities can feel empowering and overwhelming. Many of your finely honed nursing skills will serve you well as a manager,...
Patient-centered care focused on self-sufficiency The Centers for Medicare and Medicaid Services (CMS) uses the term “home health” to describe a federal health insurance program that provides intermittent short-term care to help patients recover from illness and become as self-sufficient as possible at home. Professionals who participate in home health include nurses, physical therapists, occupational...
As nursing and academia have evolved, so too has the definition of faculty practice. It can include clinical practice, scholarship, clinical research, education, consultation, leadership and administration, preceptorship, policy advocacy, and quality improvement management. It also may refer to the clinical work undertaken by nursing faculty who maintain active roles in patient care, health services, […]
The United States continues to experience a shortage of frontline nurses, and a critical nurse faculty shortage impedes efforts to educate nurses to meet clinical workforce demands. In 2021, according to the American Association of Colleges of Nursing, U.S. nursing programs turned away 76,000 qualified prelicensure applicants due to a shortage of nursing faculty. Several...
Shared governance provides clinical nurses with a voice and opportunities to engage within an organization. It allows them to step into leadership roles to strengthen the inpatient, ambulatory, or direct patient care units in which they work.
USN nurses share their deployment experiences. Have you ever thought about a career as a U.S. Navy (USN) nurse? If so, you must consider that USN nurses hold two jobs—Naval officer and RN—and most are assigned to an operational platform for either their primary job responsibility or as a collateral role. USN nurses deploy with...
Nurses of color and those from other marginalized groups face several barriers to pursuing career advancement, including racial discrimination, few role models, and lack of support. However, exposure and mentorship can serve as a mechanism to address the mismatch between patient and nursing workforce demographics
I recently visited an 83-year-old patient in the hospital after EMTs rushed her to the ER with an infected leg wound. Her ordeal started inconspicuously when she bumped into the sharp edge of a table and developed a small cut. The patient’s wound didn’t close, but she ignored it until she woke up in pain one morning two weeks after first injuring her leg. Her daughter called 911 after noticing angry, red skin discoloration and pus – both signs of an infection. Our medical team treated her with IV antibiotics and cleared up the infection, but the wound did not fully close until at least a month later, well after she was discharged from the hospital.
How different the story is when children get a cut. They may scream initially, but within days, the scab falls off, revealing new skin. Why was healing so delayed in my 83-year-old patient compared to a healthy child?
The answer is age. Decades of life slow down healing for most tissues, and wounds in skin can offer a window into why this slowdown occurs.
Three stages of wound healing
I am physician who studies how aging predisposes patients to diseases like diabetes and whether behavioral changes such as intermittent fasting may slow down aging. In order to understand why the skin wound in my older patient healed so slowly, it is important to first understand how wounds heal under the ideal conditions of youth.
The first stage is inflammation, essentially the body’s attempt to clean the wound. During the inflammatory phase, immune cells called phagocytes move into the wound, kill any contaminating bacteria, and ingest and dispose of dead cells and debris.
Inflammation sets the stage for the regenerative phase, where several processes work in concert to regrow damaged skin. Replacement skin cells are born when cells at the edge of the wound divide, while fibroblast cells lay down a supportive scaffolding called the extracellular matrix. This holds the new cells together. Any damaged supporting structures of the skin, such as the blood vessels that supply critical oxygen and nutrients, also need to regrow. The second stage effectively closes the wound and restores a protective barrier against bacteria.
Once the wound is fully closed, the remodeling phase will rebuild the tissue in a stronger way. Jpbarrass via Wikimedia Commons
The regenerative phase is a relatively quick, but tenuous fix – new skin is fragile. The final remodeling phase plays out over a couple of years as the new skin is progressively strengthened by several parallel processes. The extracellular matrix, which was initially laid down in a haphazard fashion, is broken down and replaced in a more durable way. Any residual cells from prior phases that are no longer needed – such as immune cells or fibroblasts – become inactive or die. In addition to strengthening the new skin, these collective actions also account for the tendency of scars to visibly fade with time.
One major way aging can derail the orderly and efficient progression through the stages of healing is through the health problems that stem from diseases of old age.
Diabetes is one example of a disease that is strongly associated with older age. One of the many ways that diabetes negatively affects healing is by causing blood vessels to narrow. As a consequence of inadequate circulation, crucial nutrients and oxygen do not reach the wound in sufficient quantities to fuel the second regenerative phase.
Diabetes is just one of many age-related diseases that disrupts normal processes in the body such as wound healing.
When cells divide more slowly – or when they stop dividing altogether due to senescence – skin becomes thinner. The replacement of fat cells, which form a cushioning layer under the skin, also declines with age. The skin of older patients is therefore more prone to injury in the first place.
Once an older person’s skin is injured, the skin has a harder time healing properly as well. Aging and senescent immune cells cannot defend against bacteria, and the risk of serious skin infection rises. Then in the regenerative stage, slow rates of cell division translate into slow skin regrowth. My patient exhibited all of these negative effects of age – her thin, almost translucent skin ruptured from a minor bump, became infected and took nearly two months to fully regrow.
But senescent cells are more than just dysfunctional bystanders. For reasons that are not yet fully understood, senescent cells release toxic byproducts that damage surrounding tissue and drive inflammation – even when there’s no bacterial threat present. Some of these byproducts can even accelerate senescence in neighboring cells. This suggests that intrinsic aging of cells is in essence contagious and senescent cells actively fuel an uncontrolled cycle of inflammation and tissue damage that further impedes successful regeneration and healing.
A whole body problem
As the most outwardly visible tissue of the body, the skin provides a window into why people heal more slowly with age, but all tissues can be injured and are susceptible to the effects of aging. Injuries may be small, repetitive and build up over time – like the effect of smoking on the lungs. Or they may be discrete and dramatic – such as the death of heart cells with a heart attack. Different tissues may heal in different ways. Yet all tissues share a sensitivity to the repercussions of an aging immune system and a decline in the ability to regrow dead or damaged cells.
Understanding why healing slows down with age is important, but my patient asked a very practical question that physicians often face in one form or another: “Doctor, what can you do for me?”
Unfortunately, current treatment of wounds is fairly old-fashioned and often ineffective. Some of the options available include wound dressing changes, antibiotics when the wound is infected or treatment in a high oxygen chamber when circulation is bad due to diabetes.
There is hope, though, that medicine can do better and that progress in understanding the aging process will lead to new therapies. Neutralizing senescent cells in mice, for example, improves a variety of age-associated diseases. While it is way too early to say that researchers have discovered the fountain of youth, I am optimistic for a future when physicians will bend the aging curve and make skin and other organs heal faster and better.
The word “leprosy” conjures images of biblical plagues, but the disease is still with us today. Caused by infectious bacteria, some 200,000 new cases are reported each year, according to the World Health Organization. In the United States, leprosy has been entrenched for more than a century in parts of the South where people came into contact with armadillos, the principle proven linkage from animal to humans. However, the more recent outbreaks in the Southeast, especially Florida, have not been associated with animal exposure.
The Conversation talked with Robert A. Schwartz, professor and head of dermatology at Rutgers New Jersey Medical School, to explain what researchers know about the disease.
What is leprosy and why is it resurfacing in the US?
Leprosy is caused by two different but similar bacteria — Mycobacterium leprae and Mycobacterium lepromatosis — the latter having just been identified in 2008. Leprosy, also known as Hansen’s disease, is avoidable. Transmission among the most vulnerable in society, including migrant and impoverished populations, remains a pressing issue.
Leprosy is beginning to occur regularly within parts of the southeastern United States. Most recently, Florida has seen a heightened incidence of leprosy, accounting for many of the newly diagnosed cases in the U.S.
Traditional risk factors include zoonotic exposure and having recently lived in leprosy-endemic countries. Brazil, India and Indonesia have each noted more than 10,000 new cases since 2019, according to the World Health Organization data, and more than a dozen countries have reported between 1,000 to 10,000 new cases over the same time period.
From that time until the mid-20th century, limited treatments were available, so the bacteria could infiltrate the body and cause prominent physical deformities such as disfigured hands and feet. Advanced cases of leprosy cause facial features resembling that of a lion in humans.
Many mutilating and distressing skin disorders such as skin cancers and deep fungal infections were also confused with leprosy by the general public.
Fear of contagion has led to tremendous stigmatization and social exclusion. It was such a serious concern that the Kingdom of Jerusalem had a specialized hospital to care for those suffering from leprosy.
How infectious is leprosy?
Research shows that prolonged in-person contact via respiratory droplets is the primary mode of transmission, rather than through normal, everyday contact such as embracing, shaking hands or sitting near a person with leprosy. People with leprosy generally do not transmit the disease once they begin treatment.
Armadillos represent the only known zoonotic reservoir of leprosy-causing bacteria that threaten humans. These small mammals are common in Central and South America and in parts of Texas, Louisiana, Missouri and other states, where they are sometimes kept as pets or farmed as meat. Eating armadillo meat is not a clear cause of leprosy, but capturing and raising armadillos, along with preparing its meat, are risk factors.
The transmission mechanism between zoonotic reservoirs and susceptible individuals is unknown, but it is strongly suspected that direct contact with an infected armadillo poses a significant risk of developing leprosy. However, many cases reported in the U.S. have demonstrated an absence of either zoonotic exposure or person-to-person transmission outside of North America, suggesting that transmission may be happening where the infected person lives. But in many cases, the source remains an enigma.
Leprosy primarily affects the skin and peripheral nervous system, causing physical deformity and desensitizing one’s ability to feel pain on affected skin.
It may begin with loss of sensation on whitish patches of skin or reddened skin. As the bacteria spread in the skin, they can cause the skin to thicken with or without nodules. If this occurs on a person’s face, it may rarely produce a smooth, attractive-appearing facial contour known as lepra bonita, or “pretty leprosy.” The disease can progress to causing eyebrow loss, enlarged nerves in the neck, nasal deformities and nerve damage.
The onset of symptoms can sometimes take as long as 20 years because the infectious bacteria have a lengthy incubation period and proliferate slowly in the human body. So presumably many people are infected long before they know that they are.
Fortunately, worldwide efforts to screen for leprosy are being enhanced thanks to organizations like the Order of Saint Lazarus, which was originally founded in the 11th century to combat leprosy, and the Armauer Hansen Research Institute, which conducts immunologic, epidemiological and translational research in Ethiopia. The nongovernmental organization Bombay Leprosy Project in India does the same.
How treatable is it?
Leprosy is not only preventable but treatable. Defying stigma and advancing early diagnosis via proactive measures are critical to the mission of controlling and eradicating it worldwide.
Notably, the World Health Organization and other agencies provide multi-drug therapy at no cost to patients.
In addition, vaccine technology to combat leprosy is in the clinical trials stage and could become available in coming years. In studies involving nine-banded armadillos, this protein-based vaccine delayed or diminished leprous nerve damage and kept bacteria at bay. Researchers believe that the vaccine can be produced in a low-cost, highly efficient manner, with the long-term prospect of eradicating leprosy.
If health care professionals, biomedical researchers and lawmakers do not markedly enhance their efforts to eliminate leprosy worldwide, the disease will continue to spread and could become a far more serious problem in areas that have been largely free of leprosy for decades.
The World Health Organization launched a plan in 2021 for achieving zero leprosy.
Flesh-eating bacteria sounds like the premise of a bad horror movie, but it’s a growing – and potentially fatal – threat to people.
In September 2023, the Centers for Disease Control and Prevention issued a health advisory alerting doctors and public health officials of an increase in flesh-eating bacteria cases that can cause serious wound infections.
There are several types of bacteria that can infect open wounds and cause a rare condition called necrotizing fasciitis. These bacteria do not merely damage the surface of the skin – they release toxins that destroy the underlying tissue, including muscles, nerves and blood vessels. Once the bacteria reach the bloodstream, they gain ready access to additional tissues and organ systems. If left untreated, necrotizing fasciitis can be fatal, sometimes within 48 hours.
The bacterial species group A Streptococcus, or group A strep, is the most common culprit behind necrotizing fasciitis. But the CDC’s latest warning points to an additional suspect, a type of bacteria called Vibrio vulnificus. There are only 150 to 200 cases of Vibrio vulnificus in the U.S. each year, but the mortality rate is high, with 1 in 5 people succumbing to the infection.
How do you catch flesh-eating bacteria?
Vibrio vulnificus primarily lives in warm seawater but can also be found in brackish water – areas where the ocean mixes with freshwater. Most infections in the U.S. occur in the warmer months, between May and October. People who swim, fish or wade in these bodies of water can contract the bacteria through an open wound or sore.
Vibrio vulnificus can also get into seafood harvested from these waters, especially shellfish like oysters. Eating such foods raw or undercooked can lead to food poisoning, and handling them while having an open wound can provide an entry point for the bacteria to cause necrotizing fasciitis. In the U.S., Vibrio vulnificus is a leading cause of seafood-associated fatality.
Why are flesh-eating bacteria infections rising?
Vibrio vulnificus is found in warm coastal waters around the world. In the U.S., this includes southern Gulf Coast states. But rising ocean temperatures due to global warming are creating new habitats for this type of bacteria, which can now be found along the East Coast as far north as New York and Connecticut. A recent study noted that Vibrio vulnificus wound infections increased eightfold between 1988 and 2018 in the eastern U.S.
Climate change is also fueling stronger hurricanes and storm surges, which have been associated with spikes in flesh-eating bacteria infection cases.
Aside from increasing water temperatures, the number of people who are most vulnerable to severe infection, including those with diabetes and those taking medications that suppress immunity, is on the rise.
What are symptoms of necrotizing fasciitis? How is it treated?
Early symptoms of an infected wound include fever, redness, intense pain or swelling at the site of injury. If you have these symptoms, seek medical attention without delay. Necrotizing fasciitis can progress quickly, producing ulcers, blisters, skin discoloration and pus.
Treating flesh-eating bacteria is a race against time. Clinicians administer antibiotics directly into the bloodstream to kill the bacteria. In many cases, damaged tissue needs to be surgically removed to stop the rapid spread of the infection. This sometimes results in amputation of affected limbs.
Researchers are concerned that an increasing number of cases are becoming impossible to treat because Vibrio vulnificus has evolved resistance to certain antibiotics.
People who have a fresh cut, including a new piercing or tattoo, are advised to stay out of water that could be home to Vibrio vulnificus. Otherwise, the wound should be completely covered with a waterproof bandage.
People with an open wound should also avoid handling raw seafood or fish. Wounds that occur while fishing, preparing seafood or swimming should be washed immediately and thoroughly with soap and water.
Anyone can contract necrotizing fasciitis, but people with weakened immune systems are most susceptible to severe disease. This includes people taking immunosuppressive medications or those who have pre-existing conditions such as liver disease, cancer, HIV or diabetes.
It is important to bear in mind that necrotizing fasciitis presently remains very rare. But given its severity, it is beneficial to stay informed.
Debbie King barely gave it a second thought when she scraped her right shin climbing onto her friend’s pontoon for a day of boating in the Gulf of Mexico on Aug. 13.
Even though her friend immediately dressed the slight cut, her shin was red and sore when King awoke the next day. It must be a sunburn, she thought.
But three days later, the red and blistered area had grown. Her doctor took one look and sent King, 72, to the emergency room.
Doctors at HCA Florida Citrus Hospital in Inverness, Florida, rushed King into surgery after recognizing the infection as Vibrio vulnificus, a potentially fatal bacterium that kills healthy tissue around a wound. While King lay on the operating table, the surgeon told her husband she would likely die if they didn’t amputate.
Just four days after the scrape, King lost her leg then spent four days in intensive care.
“The flesh was gone; it was just bone,” she said of her leg.
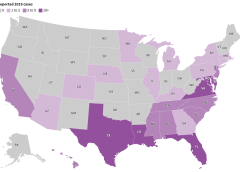
Cases of V. vulnificus are rare. Between 150 and 200 are reported to the Centers for Disease Control and Prevention every year, with about 20% resulting in death. Most are in states along the Gulf of Mexico, but, in 2019, 7% were on the Pacific Coast. Florida averages about 37 cases and 10 deaths a year.
But a rise in cases nationally and the spread of the disease to states farther north — into coastal communities in states such as Connecticut, New York, and North Carolina — have heightened concerns about the bacterium, which can result in amputations or extensive removal of tissue even in those who survive its infections. And warmer coastal waters caused by climate change, combined with a growing population of older adults, may result in infections doubling by 2060, a study in Scientific Reports warned earlier this year.
“Vibrio distributions are driven in large part by temperature,” said Tracy Mincer, an assistant professor at Florida Atlantic University. “The warmer waters are, the more favorable it is for them.”
The eastern United States has seen an eightfold increase in infections over a 30-year period through 2018 as the geographic range of infections shifted north by about 30 miles a year, according to the study, which was cited in a CDC health advisory last month.
The advisory was intended to make doctors more aware of the bacterium when treating infected wounds exposed to coastal waters. Infections can also arise from eating raw or undercooked seafood, particularly oysters, it warned. That can cause symptoms as common as diarrhea and as serious as bloodstream infections and severe blistered skin lesions.
New York and Connecticut this summer issued health warnings about the risk of infection as well. It’s not the first year either state has recorded cases.
“There’s very few cases but when they happen, they’re devastating,” said Paul A. Gulig, a professor in the Department of Molecular Genetics and Microbiology at the University of Florida College of Medicine.
‘An Accident of Nature’
Vibrio has more than 100 strains, including the bacterium that causes cholera, a disease that causes tens of thousands of deaths worldwide each year.
The V. vulnificus strain likes warm brackish waters close to shorelines where the salinity is not as high as in the open sea. Unlike some other Vibrio strains, it has no mechanism to spread between humans.
It’s found in oysters because the mollusks feed by filtering water, meaning the bacterium can become concentrated in oyster flesh. It can enter humans who swim in salty or brackish waters through the slightest cut in the skin. Infections are treated with antibiotics and, if needed, surgery.
“It’s almost an accident of nature,” Gulig said. “They have all these virulence factors that make them really destructive, but we’re not a part of this bug’s life cycle.”
Once inside the human body, the bacteria thrive.
Scientists don’t believe the bacteria eat flesh, despite how they’re often described. Rather, enzymes and toxins secreted by the bacterium as it multiplies break down the human tissue in the area below the skin, causing necrosis, or death of tissue cells.
The infection spreads like wildfire, Gulig said, making early detection critical.
“If you take a pen and mark where the edge of the redness is and then look at that two or four hours later, the redness would have moved,” Gulig said. “You can almost sit there and watch this spread.”
Researchers have conducted studies on the bacteria, but the small number of cases and deaths make it tough to secure funding, said Gulig. He said he switched his research focus to other areas because of the lack of money.
But growing interest in the bacteria has prompted talk about new research at his university’s Emerging Pathogens Institute.
Examining the bacteria’s genome sequence and comparing it with those of Vibrio strains that don’t attack human flesh could yield insights into potential drugs to interfere with that process, Gulig said.
Shock and Loss
Inside the operating room at HCA Florida Citrus, the only signs of King’s infection were on her shin. The surgeon opened that area and began cutting away a bright red mush of dead flesh.
Hoping to save as much of the leg as possible, the doctor first amputated below her knee.
But the bacteria had spread farther than doctors had hoped. A second amputation, this time 5 inches above the knee, had to be performed.
After surgery, King remained in critical care for four days with sepsis, a reaction to infection that can cause organs to fail.
Her son was there when she awakened. He was the one who told her she had lost her leg, but she was too woozy from medication to take it in.
It wasn’t until she was transferred to a rehab hospital in nearby Brooksville run by Encompass Health that the loss sank in.
A former radiation protection technician, King had always been self-reliant. The idea of needing a wheelchair, of being dependent on others — it felt like she had lost part of her identity.
One morning, she could just not stop crying. “It hit me like a ton of bricks,” she said.
Six different rehab staffers told her she needed to meet with the hospital’s consulting psychologist. She thought she didn’t need help, but she eventually gave in and met with Gerald Todoroff.
In four sessions with King, he said, he worked to redirect her perception of what happened. Amputation is not who you are but what you will learn to deal with, he told her. Your life can be as full as you wish.
“They were magic words that made me feel like a new person,” King said. “They went through me like music.”
Physical therapy moved her forward, too. She learned how to stand longer on her remaining leg, to use her wheelchair, and to maneuver in and out of a car.
Now, back in her Gulf Coast community of Homosassa, those skills have become routine. Her husband, Jim, a former oil company worker and carpenter, built an access ramp out of concrete and pressure-treated wood for their single-story home.
But she is determined to walk with the aid of a prosthetic leg. It’s the motivation for a one-hour regimen of physical therapy she does on her own every day in addition to twice-weekly sessions with a physical therapist.
Recovery still feels like a journey but one marked by progress. She has nicknamed her “stump” Peg. She’s now comfortable sharing before and after pictures of her leg.
And she’s made it her mission to talk about what happened so more people will learn about the danger.
“This is the most horrific thing that can happen to anybody,” she said. “But I’d sit back and think, ‘God put you here for a reason — you’ve got more things to do.’”
What to Know About ‘Flesh-Eating’ Bacterium Vibrio vulnificus
Infection Symptoms:
Diarrhea, often accompanied by stomach cramping, nausea, vomiting, and fever.
Wound infections cause redness, pain, swelling, warmth, discoloration, and discharge. They may spread to the rest of the body and cause fever.
Bloodstream infections cause fever, chills, dangerously low blood pressure, and blistering skin lesions.
To Protect Against Vibrio Infections:
Stay out of saltwater or brackish water if you have a wound or a recent surgery, piercing, or tattoo.
Cover wounds with a waterproof bandage if they could come into contact with seawater or raw or undercooked seafood and its juices.
Wash wounds and cuts thoroughly with soap and water after contact with saltwater, brackish water, raw seafood, or its juices.
Who Is Most at Risk:
Anyone can get a wound infection. People with liver disease, cancer, or diabetes, and those over 40 or with weakened immune systems, are more likely to get an infection and have severe complications.
This article was produced in partnership with the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.