Starting your own consulting business is an exciting and rewarding experience: You’re the boss; you’re in charge. The question is, do you have what it takes? Along with the excitement of being the boss comes the responsibility of decisions and commitment. Your decisions will affect whether the business is a failure or a success.
To succeed in consulting, you must be an expert at recognizing problems and shaping solutions to those problems, and you must possess excellent time-management and networking skills. If you think you have what it takes to be a consultant, read on. This article gives an overview of the process.
Nature of the business
Businesses hire consultants for their expertise to help them identify problems, supplement staff, institute change, provide an objective viewpoint, or teach.
Examples of specific services you can offer include single patient reviews, serving as a member of the wound care team, making wound rounds on all patients, providing education, patient teaching, protocol development, and troubleshooting. These services are provided in many settings—long-term care, home care, long-term acute care, rehabilitation hospitals, acute-care hospitals, insurance companies, and primary-care provider groups. (more…)
Study finds ultrasound therapy improves venous ulcer healing
In a study of 10 venous ulcers not responding to treatment, the use of noncontact ultrasound significantly reduced the wound area over 4 weeks of treatment.
It has been unclear exactly how ultrasound achieves its positive results. The
authors of “A prospective pilot study of ultrasound therapy effectiveness in refractory venous leg ulcers,” an article published online on February 1 by the International Wound Journal, found that patients treated with ultrasound and compression therapy had reduced inflammatory cytokines and bacterial counts, but the reduction wasn’t statistically significant.
The study found another important benefit for patients-reduced pain.
Serum albumin is not a goodindicator of nutritional status
Traditionally the standard of practice for wound care patients has been to review albumin blood levels as a measure of nutritional status and the effect of nutritional interventions. But as noted in The Role of Nutrition in Pressure Ulcer Prevention and Treatment: National Pressure Ulcer Advisory Panel White Paper, recent studies show that hepatic proteins (albumin, transthyretin, and transferrin) correlate with the severity of an underlying disease, not nutritional status. Moreover, many factors can alter albumin levels even when protein intake is adequate, including infection, acute stress, surgery, cortisone excess, and hydration status.
For these reasons, the National Pressure Ulcer Advisory Panel (NPUAP) and the Academy of Nutrition and Dietetics (previously known as The American Dietetic Association) recommend against using serum proteins as a nutritional assessment tool. Evaluation of lab values is just one part of the nutritional assessment process and should be considered along with other factors such as ensuring that the patient receives what is prescribed; daily food/fluid intake; changes in weight status, diagnosis, and medications; and clinical improvement in the wound.
The mean number of serious comorbid conditions was 1.8.
The most common comorbid conditions were obesity/overweight (71.3%), cardiovascular or peripheral vascular disease (51.3%), and diabetes (46.8%).
Nearly two-thirds (65.8%) of wounds healed, with an average healing time
of 15 weeks.
In half of the wounds that healed, patients received only moist wound care and no advanced therapeutics.
The mean cost for wound healing was $3,927.
The authors of the article, published in March’s Wounds, analyzed 5,240 patients with 7,099 wounds in 59 hospital-based outpatient wound centers in 18 states over 5 years.
LOI index comparable to ABI for assessing PAD in patients with type 2 diabetes
The pilot study “Lanarkshire Oximetry Index as a diagnostic tool for peripheral arterial disease in type 2 diabetes,” published in Angiology, compared the gold standard ankle brachial index (ABI) to the Lanarkshire Oximetry Index (LOI) in 161 patients with type 2 diabetes. Researchers assessed the patients for peripheral artery disease (PAD, defined as ABI < 0.9) using both ABI and LOI.
Using a LOI cut-off value of 0.9., the sensitivity and specificity for PAD were 93.3% and 89.1%, respectively. The study concluded that LOI is a “potentially useful alternative diagnostic test for PAD” in patients with type 2 diabetes.
LOI is a noninvasive procedure similar to ABI; both indices indicate whether it’s safe to apply compression to the limb of a patient who has lower leg ulceration or venous hypertension. With LOI, a pulse oximeter is used in place of a hand-held Doppler to determine the index.
Start planning for World Diabetes Day
It’s not too early to begin planning for World Diabetes Day, November 14. Started by the World Health Organization (WHO) and the International Diabetes Federation (IDF), the day is designed to raise global awareness of diabetes.
Access materials, including posters, a campaign book, and the Word Diabetes Day Logo, from IDF’s website, which also has activity ideas.
WHO estimates that more than 346 million people worldwide have diabetes, and the number is expected to double by 2030. World Diabetes Day is celebrated on November 14 to mark the birthday of Frederick Banting who, along with Charles Best, was instrumental in the discovery of insulin in 1922.
Guidelines for PAD in patients with diabetes and foot ulceration published
February’s issue of Diabetes/Metabolism Research and Reviews includes “Specific guidelines for the diagnosis and treatment of peripheral arterial disease in a patient with diabetes and ulceration of the foot 2011,” which is based on two companion International Working Group on the Diabetic foot papers. The guidelines state that if a patient’s PAD is impairing wound healing, revascularization through bypass or endovascular technique must be considered except in a few cases such as severely frail patients. Limb salvage rates after revascularization procedures are about 80-85%, and there is ulcer healing in > 60% at 12 months.
Other points of particular interest to wound care professionals:
Patients with PAD and a foot infection are at high risk for major limb amputation, so should be treated as a “medical emergency”, preferably within 24 hours.
Half of patients with diabetes, a foot ulcer, and PAD die within 5 years because of higher cardiovascular morbidity and mortality. Cardiovascular risk management should include “support for cessation of smoking, treatment of hypertension, and prescription of a statin as well as low-dose aspirin or clopidrogel.
By: Darlene Hanson, MS, RN, Pat Thompson, MS, RN, Diane Langemo, PhD, RN, FAAN, Susan Hunter, MS, RN, and Julie Anderson, PhD, RN, CCRC
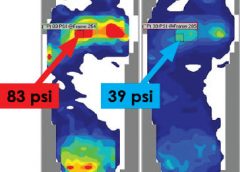
Faced with the nursing diagnosis of Impaired skin integrity, we’ve all written care plans that state our goal as “redistributing or reducing pressure.” But how do we do that? Which measures do we take? And how do we know that our interventions have relieved pressure? Do we rely solely on a skin assessment? A patient’s self-assessment of comfort? What if the patient can’t feel pressure relief because of neurologic impairment?
The answers to these questions may be that nurses should use pressure mapping, a tool used by occupational and physical therapists to determine seat-interface pressures and by other healthcare professionals to perform foot assessments. (more…)
By Nancy Chatham, MSN, RN, ANP-BC, CWOCN, CWS, and Carrie Carls, BSN, RN, CWOCN, CHRN
Moisture-related skin breakdown has been called many things-perineal dermatitis, irritant dermatitis, contact dermatitis, heat rash, and anything else caregivers could think of to describe the damage occurring when moisture from urine or stool is left on the skin. At a 2005 consensus conference, attendees chose the term incontinence-associated dermatitis (IAD).
IAD can be painful, hard to properly identify, complicated to treat, and costly. It’s part of a larger group of moisture-associated skin damage that also includes intertrigo and periwound maceration. IAD prevalence and incidence vary widely with the care setting and study design. Appropriate diagnosis, prompt treatment, and management of the irritant source are crucial to long-term treatment.
Causes
IAD stems from the effects of urine, stool, and containment devices on the skin. The skin’s pH contributes to its barrier functions and defenses against bacteria and fungus; ideal pH is 5.0 to 5.9. Urine pH ranges from 4.5 to 8.0; the higher range is alkaline and contributes to skin damage.
Skin moisture isn’t necessarily damaging. But when moisture that contains irritating substances, such as alkaline urine, contacts the skin for a prolonged period, damage can occur. Urine on the skin alters the normal skin flora and increases permeability of the stratum corneum, weakening the skin and making it more susceptible to friction and erosion. Fecal incontinence leads to active fecal enzymes on the skin, which contribute to skin damage. Fecal bacteria can penetrate the skin, increasing the risk of secondary infection. Wet skin has a lower temperature than dry skin; wet skin under a pressure load has less blood flow than dry skin.
Containment devices, otherwise known as adult diapers or briefs, are multilayer disposable garments containing a superabsorbent polymer. The polymer is designed to wick and trap moisture in the containment device. This ultimately affects the skin by trapping heat and moisture, which may cause redness and inflammation that can progress to skin erosion. This trapping can lead to increased pressure against the skin, especially if the device has absorbed liquid and remains in contact with the skin.
Categorizing IAD
IAD is categorized as mild, moderate, or severe. (See Picturing IAD by clicking the PDF icon above.)
Screening for IAD
Screen the patient’s skin for persistent redness, inflammation, rash, pain, and itching at least daily. To differentiate IAD from pressure ulcers, keep in mind that:
IAD can occur wherever urine or stool contacts the skin. In contrast, pressure ulcers arise over bony prominences in the absence of moisture.
With IAD, affected skin is red or bright red. With a pressure ulcer, skin may take on a bluish purple, red, yellow, or black discoloration.
The skin-damage pattern in IAD usually is diffuse. With a pressure ulcer, edges are well defined.
The depth of IAD-related skin damage usually is partial-thickness without necrotic tissue. With a pressure ulcer, skin damage depth may vary.
Preventing IAD
The three essentials of IAD prevention are to cleanse, moisturize, and protect.
Cleanse the skin with a mild soap that’s balanced to skin pH and contains surfactants that lift stool and urine from the skin. Clean the skin routinely and at the time of soiling. Use warm (not hot) water, and avoid excess force and friction to avoid further skin damage.
Moisturize the skin daily and as needed. Moisturizers may be applied alone or
incorporated into a cleanser. Typically, they contain an emollient such as lanolin to replace lost lipids in the stratum corneum.
To protect the skin, apply a moisture-barrier cream or spray if the patent has significant urinary or fecal incontinence (or both). The barrier may be zinc-based, petrolatum-based, dimethicone-based, an acrylic polymer, or another type. Consider using an algorithm developed by wound and skin care specialists that’s customized for skin care products your facility uses. (See Skin care algorithm by clicking the PDF icon above.)
If the treatment protocol fails, the patient should be referred to an appropriate skin care specialist promptly.
To help prevent urine or stool from contacting the patient’s skin, consider using a male external catheter, a female urinary pouch, a fecal pouch, or a bowel management system. Avoid containment devices. If the patient has a containment pad, make sure it’s highly absorbent and not layered, to decrease pressure under the patient.
Managing IAD
A comprehensive multidisciplinary approach to IAD is essential to the success of any skin care protocol. Identify skin care champions within your facility and educate them on IAD. Incorporating administrators, physicians, nursing staff, therapists, and care assistants makes implementation of protocols and algorithms within an institution seamless.
Administrators support the skin care program in the facility, including authorizing a budget so product purchases can be made. The certified wound clinician is the team expert regarding skin care, incontinence, prevention, and product recommendation. The physician oversees protocol development and evaluates and prescribes additional treatment when a patients fails to respond to treatment algorithms. Nursing staff identify patients at risk, incorporate the algorithm into the patient’s plan of care, and direct care
assistants. Therapists address function, strength, and endurance issues to improve the patient’s self-care abilities in activities of daily living to manage or prevent episodes of incontinence.
In severe inflammation, topical dressings, such as alginates and foam dressings, may be used along with topical corticosteroids. In complex IAD, antifungals or antibiotics may be required if a secondary fungal or bacterial infection is suspected.
Additional diagnostic tests may be done to identify and treat secondary infections. These tests may include skin scraping, potassium hydroxide test or Gram’s stain for fungal components, or a swab culture and sensitivity for bacterial infections. If your patient has a suspected secondary fungal or bacterial infection, use appropriate treatments for the full course of recommended therapy. In severe secondary fungal infection, an oral agent may be added to topical therapy. If cost is a concern, consider using a pharmacy knowledgeable about compounding for topical combination therapies.
Referrals and education
For assessment and treatment of under-lying incontinence, refer the patient to a continence specialist if appropriate. Teach the patient strategies for managing incontinence through dietary measures, toileting programs, pelvic-floor muscle training, clothing modification, and mobility aids.
Selected references
Beguin A, Malaquin-Pavan E, Guihaire C, et al., Improving diaper design to address incontinence associated dermatitis. BMC Geriatrics. 2010;10:86. http://www.biomedcentral.com/1471-2318/10/86. Accessed March 15, 2012.
Black JM, Gray M, Bliss DZ, et al. MASD part 2: incontinence-associated dermatitis and intertriginous dermatitis. J Wound Ostomy Continence Nurs. 2011; 38(4):359-370.
Bliss DZ, Zehrer C, Savik K, et al. An economic evaluation of four skin damage prevention regimens in nursing home residents with incontinence: economics of skin damage prevention. J Wound Ostomy Continence Nurs. 2007;34(2):143-152.
Denat Y, Khorshid L. The effect of 2 different care products on incontinence-associated dermatitis in patients with fecal incontinence. J Wound Ostomy Continence Nurs. 2011;38(2):171-176.
Doughty DB. Urinary and Fecal Incontinence: Current Management Concepts. 3rd ed. St. Louis, MO: Mosby Elsevier; 2006.
Gray, M. Optimal management of incontinence-associated dermatitis in the elderly. Am J Clin Dermatol. 2010;11(3):201-210.
Gray M, Beeckman D, Bliss DZ, et al. Incontinence-associated dermatitis: a comprehensive review and update. J Wound Ostomy Continence Nurs. 2012;39(1):61-74
Gray M, Bliss DZ, Doughty DB, et al. Incontinence-associated dermatitis: a consensus. J Wound Ostomy Continence Nurs. 2007;34(1):45-54.
Gray M, Bohacek L, Weir D, et al. Moisture vs pressure: making sense out of perineal wounds. J Wound Ostomy Continence Nurs. 2007;34(2):134-42.
Junkin J, Lerner-Selekof JL. Prevalence of incontinence and associated skin injury in the acute care inpatient. J Wound Ostomy Continence Nurs. 2007;34(3):260-269.
Landefeld CS, Bowers BJ, Feld AD, et al. National Institutes of Health state-of-the-science conference statement: prevention of fecal and urinary incontinence in adults. Ann Intern Med. 2008;148(6):449-458.
Langemo D, Hanson D, Hunter S, et al. Incontinence and incontinence-associated dermatitis. Adv Skin Wound Care. 2011;24(3):126-142.
Nancy Chatham is an advanced practice nurse at Passavant Physician Associates in Jacksonville, Illinois. Carrie Carls is the nursing director of advanced wound healing and hyperbaric medicine at Passavant Area Hospital in Jacksonville, Illinois.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Co-Founder
Wound Care Education Institute
Lake Geneva, IL
Editorial Advisory Board
Nenette L. Brown, RN, PHN, MSN/FNP, WCC
Wound Care Program Coordinator
Sheriff’s Medical Services Division
San Diego, CA
Debra Clair, PhD, APN, RN, WOCN, WCC, DWC
Wound Care Provider
Alliance Community Hospital
Alliance, OH
Kulbir Dhillon, NP, WCC
Wound Care Specialist
Skilled Wound Care
Sacramento, CA
Fred Berg
Vice President, Marketing/Business Development
National Alliance of Wound Care and Ostomy
St. Joseph, MI
Cindy Broadus, RN, BSHA, LNHA, CLNC,
CLNI, CHCRM, WCC, DWC, OMS
Executive Director
National Alliance of Wound Care and Ostomy
St. Joseph, MI
Gail Hebert, MSN, RN, CWCN, WCC, DWC, OMS
Clincal instructor
Wound Care Education Institute
Plainfield, IL
Joy Hooper, BSN, RN, CWOCN, OMS, WCC
Owner and manager of MedicalCraft, LLC
Tifton, GA
Catherine Jackson RN, MSN, WCC
Clinical Nurse Manager
Inpatient and Outpatient Wound Care
MacNeal Hospital
Berwyn, IL
Jeffrey Jensen DPM, FACFAS
Dean & Professor of Podiatric Medicine and Surgery
Barry University School of Podiatric Medicine
Miami Shores, FL
Rosalyn S. Jordan, RN, BSN, MSc, CWOCN, WCC
Director of Clinical Education
RecoverCare, L.L.C.
Louisville, KY
Jeff Kingery
Vice President of Professional Development
RestorixHealth
Tarrytown, NY
Jeri Lundgren, RN, BSN, PHN, CWS, CWCN
Vice President of Clinical Consulting
Joerns
Charlotte, NC
Nancy Morgan, RN BSN, MBA, WOC, WCC, DWC, OMS
Co-Founder, Wound Care Education Institute
Plainfield, IL
Steve Norton, CDT, CLT-LANA
Co-founder, Lymphedema & Wound Care Education, LLC
President, Lymphedema Products, LLC
Matawan, NJ
Lu Ann Reed, RN, MSN, CRRN, RNC, LNHA, WCC
Adjunct Clinical Instructor
University of Cincinnati
Cincinnati, OH
Bill Richlen, PT, WCC, CWS, DWC
Owner
Infinitus, LLC
Chippewa Falls, WI
Cheryl Robillard,PT WCC, CLT
Clinical Specialist
Aegis Therapies
Milwaukee, WI
Stanley A Rynkiewicz III, RN, MSN, WCC, DWC, CCS
Administrator
Deer Meadows Home Health and Support Services LLC
BHP Services
Philadelphia, PA
Donald A. Wollheim, MD, WCC, DWC, FAPWCA
Owner and Clinician, IMPLEXUS Wound Care Service, LLC
Watertown, WI
Instructor for Wound Care Education Institute
Plainfield, IL