BY: NANCY MORGAN, RN, BSN, MBA, WOCN, WCC, CWCMS, DWC
An essential part of weekly wound assessment is measuring the wound. It’s vitally important to use a consistent technique every time you measure. The most common type of measurement is linear measurement, also known as the “clock” method. In this technique, you measure the longest length, greatest width, and greatest depth of the wound, using the body as the face of an imaginary clock. Document the longest length using the face of the clock over the wound bed, and then measure the greatest width. On the feet, the heels are always at 12 o’clock and the toes are always 6 o’clock. Document all measurements in centimeters, as L x W x D. Remember—sometimes length is smaller than width. (more…)
Search Results for: Spi
Think a Patient Has Rights? They Left.

by Dr. Michael Miller
There are few absolutes in my universe. I know that my youngest daughter will gleefully and with full malice (but humorously presented) find something to torment me about every time I see her; referrals from family practice docs arrive well marinated in multiple antibiotics with nary a diagnosis in sight (save for the ubiquitous “infection”); and that regardless of what I recommend, offer, beg, plead, or cajole, that the patient has the complete and total power to make their decisions regarding their care and who provides it. Unless they are deemed by multiple authorities to be incapable of making a decision, until the appropriate paperwork or an emergency situation exists mandating immediate lifesaving action, the ball bounces squarely in their court…or so I thought. (more…)
Read MoreJim Nabors Would Just Cry

by Dr. Michael Miller
For those of you not as familiar with the Hoosier State as you should be, I used to think it was essentially paradise. Jim Nabors of Gomer Pyle fame is our ubiquitous, tuneful icon with his always well-received “Back Home in Indiana” as a mantra to that source of pride. Our former Governor “My Man” Mitch Daniels was a genius who, using a combination of intelligence, common sense and the persuasive powers of a midwest Svengali, created an economic model that our neighbors can only lust after. Our medicolegal climate is among the best in the US and well it should be. However, while there are some extraordinary caregivers and facilities here, a recent US News and World Report curiously showed that almost none of our hospitals made their “Best of” lists in any category. That is not to say there is bad care but to not have a single facility in an entire state even achieve an honorable mention gives one pause to reflect. The State newspapers were notoriously quiet on this concerning fact despite their trumpeting of who does what well, when and where. (more…)
Read MoreIf All You Have is a Hammer, What Happens When You Run Out of Nails?

by Dr. Michael Miller
Over the years of making house calls for wound care, I found that there was a real need for home based mental health and behavioral care, palliative care, podiatry and lots of other things. We cater to those who are home bound based on the classic definition involving the word “Taxing”. One of the more prevalent problems affecting all patients involves the nebulous but ubiquitous, nerve jangling, aptly named, “5th Vital Sign”, namely pain. As a part of my medical group, we have created a program that provides pain management not just to the home bound but all those whose lives and lifestyles are affected adversely by it. The program is a monument to government bureaucracy involving multiple layers of paperwork, mental health evaluations, testing of bodily fluids for both illegal and legal substances and then, the actual evaluation of the patient commences. After all hurdles are vetted and then jumped, then and only then does a prescription for the appropriate nostrum leave the pad. In wound care, we treat based on the etiology, the location, the related factors, the amounts of drainage, the surrounding tissues and so on, ad nauseum. Not surprisingly, in pain management, the scenario is much different. In wound care the mantra of the dabbler is see the hole, fill the hole. In pain management, the goal is to minimize pain to maximize functionality but the overriding questions are how this is accomplished. (more…)
Read MoreCondemning Patients to a Leap of Faith

by Dr. Michael Miller
I have several letters after my name. The two that say “DO” indicate that I have the training of a physician and the requisite education and responsibilities that uphold those letters. They should mean to patients that my ultimate goal is to offer (and provide when the fates allow) the entire spectrum of medical care referable to what I am good at and what they came to seek solace for. Nothing less and if I keep my ego in check, certainly nothing more. Patients run the gamut of their perception of the medical field. But like the old sales nemesis called “Bait and Switch”, what is offered on the sign all too often does not truly match what is seen on the shelves. Arrogant people are that way because they are good at what they do and not afraid to tell others. As a child, we are told to let others brag about us but failing to let people know what we can and can’t do is integral to our patients’ survival and our success. The problem is that the glitz and glamour of being a healer all too often clouds our success. Some time ago, I blogged about the pseudo-utilitarianism of all those so-called “Wound Certification” Exams. At first blush, these seem to be the key to health, wealth, omniscience and outcomes equaled only by those wound care management companies. (more…)
Read MoreDon’t Kid Yourself, Amputation Is Unquestionably A Failure

by Dr. Michael Miller
I recently saw an ad for a pending lecture at a national conference that piqued my interest much like “deflate-gate”. The title of this lecture horrifically touted that Amputation need not be considered failure. As a full time wound care doc, I work to identify those conditions that place patients at risk of all consequences both limited and catastrophic. We use the catchy title of “Limb Preservation”. We start the process by engaging in the unusual behavior of making definitive diagnoses, then systematically address them in as comprehensive manner as possible. I am proud to tell you that while there are occasions in which a terminally damaged digit is lost, that we have rarely sacrificed the greater part of a foot and more, have had only 3 lower extremity amputations in the last 5 years on patients who’s care remained exclusively with us. Of course, when a patient for whom we have created and implemented a “Limb Pres” care plan is taken out of our system (usually via a hospitalization for a reason other then the lower extremity problem), the facility forces that be unfortunately but infrequently demonstrate their inadequacy and paranoia by gang-harangueing the patient and family. They are lambasted with lurid tales of the condition marching up the leg engulfing the foot, knee, torso, and brains much like a flesh-eating PacMan. The patient’s confidence now neutered has little chance against this persistent onslaught of inadequacy and so, much like the Queen song, “Another One Bites The Dust”. (more…)
Read MoreHelp Me, Help Me, Help Me…next Tuesday

by Dr. Michael Miller
Health care providers are by nature an altruistic bunch. I have the honor of interviewing potential entries to my beloved profession as part of the admissions process at the newest Osteopathic Medical School in Indiana, Marian University. The process is unique in that it does not simply ask the age old questions of “Why you want to be a physician ?”, (“Because I want to do primary care in a rural area”). No, our probing involves scenarios in which they have to look at a social situation, identify their thoughts, those of the opposing views and then cohesively demonstrate intelligence, confidence, logical thought processes and humanity…all in an 8 minute period repeated 7 times. Their responses juxtaposed against what I see in my day to day always gives me pause to think about how the practice of medicine has been so perverted by the promotion of self abdication of responsibility. The “let your government do it for you” mantras and newest politically correct definitions of disabled (encompassing everything from melancholia to dislike of red M and M’s) have resulted in a major paradigm shift in medicine. Whereas, the hospitals once touted their ability to heal all manner of maladies, they now recognize their cost ineffectiveness, more detrimental than beneficial care (just check the nutritional parameters of anyone pre and post hospitalization) and the downright danger of going to one, unless you are a burgeoning superbug. (more…)
Read MoreAlternate universes – Einstein’s insanity

I remain absolutely amazed that there are so many people doing the same thing and yet doing it so completely different. Depending on where a patient’s wound care and orders originate from, the care I try to translate from that starting point is always a combination of dressing regimens worthy of computer code in their simplicity. The only thing usually missing is the diagnosis. It’s as though they come from an identical planet in an alternate universe.
The issue is that there is the complete dissociation of what is done for a given wound care problem in one practice setting versus another. Having stayed as far away from hospital-based wound care as possible, I continue to be amazed by hospital wound teams touting their expertise while using two to three times a day dressing changes and therapies that are the antithesis of any identifiable evidence. They actually expect entities receiving their cases (including home healthcare agencies, LTAC, skilled facilities, and others) to copy the identical care scenario regardless of their widely variable situations. In fact, the only constant is the patient and his or her condition. (more…)
Read MoreWound care treatment explained at Rotary

When treating people for wounds, the care team preforms both a comprehensive diagnosis and comprehensive treatment, Kathy Khandaker, director of wound care at Community Hospitals and Wellness Centers-Bryan, told the Bryan Rotary Club at its Friday meeting.
The wound care clinic opened at CHWC in 2006, added ostomy care in 2007, continence care in 2010 and added a full-time physician in 2015. The care team includes a wound care nurse, a hyperbaric oxygen therapy technician and a receptionist in addition to the physician. (more…)
Read MoreBreaking silos: Effective wound healing means treatment across the continuum

Around 6.5 million patients in the U.S. suffer from chronic wounds, such as pressure injuries or ulcers. Treatment costs $25 billion each year, representing a sizable and growing problem. Despite the wide impact of chronic wounds, it’s rare to see specialized, effective wound care delivered across the care continuum.
A chronic non-healing wound is a surrogate marker for illness. These patients require holistic management of their co-morbidities and continuity across care settings.
Despite this, a great deal of emphasis has been placed on treating wounds as singular events, managed topically with expensive dressings and support surfaces. This is only a small part of wound healing.
As a physician focused solely on wound care, I have learned that we must shift the focus from simply treating the wound to treating the wounded patient. The impact in the post-acute care setting in particular is worthy of evaluation and discussion, as up to 29% of patients in long-term care facilities will experience a pressure ulcer, posing serious legal, financial, and staffing implications.
For those providers working outside long-term care, there is little understanding of challenges facing LTC providers. Acute providers do not often ask, for example, how are my LTC partners reimbursed? How are they staffed? What are the requirements and regulatory pressures they face? Asking these questions would facilitate a more productive dialogue with a focus on collaborative prevention, rather than waiting until a chronic wound occurs in the LTC setting.
Creating an integrated wound care community
To address the needs of the present and growing population of patients with chronic wounds, Healogics developed an integrated wound care community model, to coordinate the wound healing process across all care settings. The program utilizes Healogics Specialty Physicians, a subspecialty group of physicians and providers with extensive training solely focused on wound care.
HSPs provide expert inpatient consultation and ensure safe transition of patients out of the hospital into the appropriate care setting. Because HSPs see the patient regardless of post-discharge venue, patients receive the same quality of care whether they are going home, to a skilled-nursing, assisted living, or LTC setting. Because chronic wounds are surrogate markers for illness, we have realized it’s essential to have an integrated, multi-setting, and multi-disciplinary process to treat the patient and their co-morbidities.
Data collected at a pilot IWCC site in the Midwestern U.S. from 2014 to 2016 revealed very positive trends for chronic wound patients. In the acute care setting, the average length of stay decreased from 9.41 days to 5.64 days, and total cost of care per patient was reduced from $10,670 to $7,248.
We’re excited by these promising results, which were revealed at the American College of Wound Healing and Tissue Repair Conference last December. We look forward to refining and expanding the model by helping our partners in acute and LTC settings standardize their practices, use evidence-based clinical guidelines, mobilize technologies and processes, and pay critical attention to patient safety and value-based outcomes.
When it comes to wound healing, no venue of care should operate alone—an integrated solution that creates continuity for the patient is critical. There are four things LTC facilities can do to break down the silos:
Read more at McKnight’s
Read MoreReduction of 50% in Diabetic Foot Ulcers With Stem Cells

MUNICH — Local injection of mesenchymal stem cells derived from autologous bone marrow shows promise in healing recalcitrant neuropathic diabetic foot ulcers, a novel study from Egypt shows.
Presenting the results at the European Association for the Study of Diabetes (EASD) 2016 Annual Meeting, Ahmed Albehairy, MD, from Mansoura University, Egypt, said: “In patients who received the mesenchymal stem cells, ulcer reduction was found to be significantly higher compared with patients on conventional treatment after both 6 weeks and 12 weeks of follow-up. This is despite the fact that initial ulcer size was larger in the stem-cell–treated group.” (more…)
Read MoreUsing fat to help wounds heal without scars
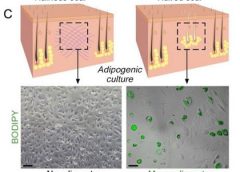
Philadelphia – Doctors have found a way to manipulate wounds to heal as regenerated skin rather than scar tissue. The method involves transforming the most common type of cells found in wounds into fat cells – something that was previously thought to be impossible in humans. Researchers began this work at the Perelman School of Medicine at the University of Pennsylvania, which led to a large-scale, multi-year study in connection with the Plikus Laboratory for Developmental and Regenerative Biology at the University of California, Irvine. They published their findings online in the journal Science on Thursday, January 5th, 2017.Fat cells called adipocytes are normally found in the skin, but they’re lost when wounds heal as scars. The most common cells found in healing wounds are myofibroblasts, which were thought to only form a scar. Scar tissue also does not have any hair follicles associated with it, which is another factor that gives it an abnormal appearance from the rest of the skin. Researchers used these characteristics as the basis for their work – changing the already present myofibroblasts into fat cells that do not cause scarring. (more…)
Read More