By Bill Richlen, PT, WCC, DWC, and Denise Richlen, PT, WCC, DCCT
How many times have you heard someone say, “I didn’t know PTs did wound care”? Statements like this aren’t uncommon. The role of physical therapists (PTs), occupational therapists, and speech therapists in wound care is commonly misunderstood by and even a mystery to many clinicians. Sometimes the therapists themselves are confused about reimbursement or what their role on the wound care team can be. (more…)
As I write this, I am still feeling the energy from the 11th annual Wild on Wounds Conference. What a great group of wound care clinicians. With close to 1,000 attendees, the conference was fun, friendly, and jam-packed with sessions for all levels of clinicians, from beginners to advanced. Many of the attendees shared their frustrations in choosing one session over another with comments such as, “It was so difficult because of all of the great educational offerings.”
Once again, the National Alliance of Wound Care and Ostomy (NAWCO) had an answer table set up in the registration area. We enjoyed the many inquiries we received, and it was nice to put faces with names.
Each year, NAWCO gives four awards to deserving clinicians who put their hearts and souls into their work. We have so many talented and committed certified wound care clinicians that it seemed only fitting to recognize these talented people and give them the opportunity to shine. These individuals are nominated by their colleagues, coworkers, peers, and subordinates, and we had an abundance of nominations. While we would have loved to recognize all of the nominees, the committee could choose only four.
During the closing session, appropriately titled “Pay it Forward,” NAWCO recognized these four exceptionally talented, committed, hard-working clinicians for their achievements in their work with wound care patients. I wanted to share some of the impressive comments made about the award winners.
Outstanding Work in Diabetic Wounds:
Anna Ruelle, DPM, WCC
• “Voted ‘top doctor’ 11+ years in a row by peers”
• “Greatly reduced the incidence of below-the-knee amputations and loss of limb”
• “Never lets the sun set on a diabetic ulcer or wound when a patient calls.”
Outstanding Research in Wound Care:
Michael Katzman, RN, BSN, ONC, WCC
• “Known for his expertise in wound care and for being very approachable, professional, and a mentor to others”
• “Works collaboratively with other hospital skin champions to develop a protocol to prevent and treat skin tears through evidence-based research”
• “Offers regular in-services while collaborating with others to continuously improve outcomes.”
Outstanding WCC of the Year:
Chelsey Hawthorne, RN-BC, BSN, WCC
• “Serves as one of the certified nurses in a long-term care facility, and is a resource for the medical-surgical and other skilled units”
• “Works with the Magnet® Program supervisor to assist in getting more nurses certified through NAWCO”
• “Collaborates with the health system’s wound care clinic to ensure proper delivery of care to the residents.”
2014 Scholarship sponsored by Joerns® RecoverCare:
Craig Johnson, RN, BSN
• “Serves as staff nurse at a busy skilled nursing facility with a diverse and complex veteran population”
• “Demonstrates an overwhelming and sincere interest in wound care”
• “Designed and developed a mobile Wound Cart, which is used as a tool in the unit’s Wound Rounds Process.”
NAWCO is proud and honored to recognize the achievements of such a dedicated group of wound care clinicians. All of us at NAWCO congratulate the 2014 award winners.
Disclaimer: The views expressed in this article are those of the author and do not necessarily represent the views of, and should not be attributed to, Wound Care Advisor. All clinical recommendations are intended to assist with determining the appropriate wound therapy for the patient. Responsibility for final decisions and actions related to care of specific patients shall remain the obligation of the institution, its staff, and the patients’ attending physicians. Nothing in this information shall be deemed to constitute the providing of medical care or the diagnosis of any medical condition. Individuals should contact their healthcare providers for medical-related information.
Radiation therapy doesn’t increase the incidence of lymphedema in patients with node-negative breast cancer, according to research presented at the American Society for Radiation Oncology’s 56th Annual Meeting held this fall. (more…)
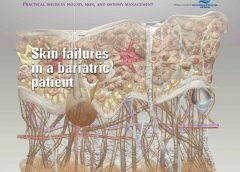
Despite the healthcare team’s best efforts, not all hospitalizations go smoothly. This article describes the case of an obese patient who underwent bariatric surgery. After a 62-day hospital stay, during which a multidisciplinary team collaborated to deliver the best care possible, he died. Although the outcome certainly wasn’t what we wanted, we’d like to share his story to raise awareness of the challenges of caring for bariatric patients.
By David L. Johnson, NHA, RAC-CT As a senior quality improvement specialist with IPRO, the Quality Improvement Organization for New York State over the past 11 years, I’ve been tasked with helping skilled nursing facilities (SNFs) embrace the process of continuous quality improvement. A necessary component of this effort has been to collect, understand, and analyze timely and accurate data.…
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN As a wound care nurse, do you feel the weight of the world on your shoulders when trying to implement a pressure ulcer prevention program? Many staff members think it’s up to the wound care nurse alone to implement the program. However, a successful program requires involvement from all staff and is…
By Hedy Badolato, RD, CSR, CNSC; Denise Dacey, RD, CDE; Kim Stevens, BSN, RN, CCRN; Jen Fox, BSN, RN, CCRN; Connie Johnson, MSN, RN, WCC, LLE, OMS, DAPWCA; Hatim Youssef, DO, FCCP; and Scott Sinner, MD, FACP Despite the healthcare team’s best efforts, not all hospitalizations go smoothly. This article describes the case of an obese patient who underwent bariatric…
Radiation and lymphedema Radiation therapy doesn’t increase the incidence of lymphedema in patients with node-negative breast cancer, according to research presented at the American Society for Radiation Oncology’s 56th Annual Meeting held this fall.
Here is a list of valuable ostomy resources, some suggested by our colleagues who follow Wound Care Advisor on Twitter. United Ostomy Association of America The United Ostomy Association of America provides comprehensive resources for patients, including information about the types of ostomies and issues related to nutrition, sexuality, and travel. Much of the information is also available in Spanish…
By Stanley A. Rynkiewicz III, MSN, RN, WCC, DWC, CCS Developing a successful wound care program requires a strong commitment and a willingness to learn. Our experience with creating such a program at Deer Meadows Home Health and Support Services, LLC (DMHHSS), a nonprofit home-care facility in Philadelphia, Pennsylvania, may help others build a similar wound care program and reap…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Measurement of wounds is an important component of wound assessment and provides baseline measurements, enables monitoring of healing rates, and helps distinguish among wounds that are static, deteriorating, or improving. All alterations in skin integrity,…
By Joy Hooper, BSN, RN, CWOCN, OMS Have you ever had an idea for improving patient care that you wanted to market? You may have lacked confidence or know-how, as I once did. But one patient, a crafty idea, and a trip to Walmart put me on the path to becoming a successful nurse entrepreneur.
By Ronald A. Sherman, MD; Sharon Mendez, RN, CWS; and Catherine McMillan, BA Note From the Editor: This is the second of two articles on maggot therapy. The first article appeared in our July/August 2014 issue, Read part 1 here. Whether your practice is an acute-care setting, a clinic, home care, or elsewhere, maggot debridement therapy (MDT) can prove to…
By Laura L. Barry, MBA, MMsc, and Maureen Sirois, MSN, RN, CEN, ANP Why is it that some things don’t bother us, while other things catapult us from an emotional 0 to 60 mph in a heartbeat? We all know what it feels like when someone says or does something that gets our juices flowing. We feel it in our…
By: Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Have you ever had a patient yell “Get out of my room!” or “Don’t touch me! I don’t want to be turned”? How about “No! Don’t put those compression stockings on my legs!” or “No, I’m not going to wear those ugly orthopedic shoes!” or “No way. I can’t stay in bed.…
A study in the Journal of Experimental Medicine describes how aspirin inhibits wound healing and paves the way for the development of new drugs to promote healing.
Pressure-ulcer prevention and management guidelines recommend support-surface therapy to help prevent and treat pressure ulcers. Support surfaces include pads, mattresses, and cushions that redistribute pressure. Full cushions and cushion pads are considered therapeutic support surfaces if used to redistribute a patient’s pressure in a chair or wheelchair.
The National Pressure Ulcer Advisory Panel (NPUAP) defines support surfaces as “specialized devices for pressure redistribution designed for the management of tissue loads, microclimate, and/or other therapeutic functions.” These surfaces address the mechanical forces associated with skin and tissue injury, such as pressure, shear, friction, and excess moisture and heat. (See Clearing up the confusion.)
Incidence density best measure of pressure-ulcer prevention program According to the National Pressure Ulcer Advisory Panel (NPUAP), incidence density is the best quality measure of pressure-ulcer prevention programs. Pressure-ulcer incidence density is calculated by dividing the number of inpatients who develop a new pressure ulcer by 1,000 patient days. Using the larger denominator of patient days allows fair comparisons between institutions…
This issue’s resources include patient tools and new guidelines. Improving patient safety Research suggests that adverse events affect patients with limited English proficiency (LEP) more frequently, are commonly caused by communication problems, and are more likely to result in serious harm compared to adverse events affecting English-speaking patients. Your hospital can take steps to reduce risks of adverse events for…
By Debra Rose Wilson, PhD, MSN, RN, IBCLC, AHN-BC, and Dana Marie Dillard, MS, HSMI Like many clinicians, you may experience stress frequently, both on and off the job. Chronic stress can alter your equilibrium (homeostasis), activating physiologic reactive pathways that cause your body to shift its priorities. Physiologic effects of stress may include: slowed digestion delay in reproductive and…
By Pamela Anderson, MS, RN, APN-BC, CCRN, and Terri Townsend, MA, RN, CCRN-CMC, CVRN-BC Jan Smith, age 59, is admitted to the coronary intensive care unit with an acute inferior myocardial infarction (MI). Recently diagnosed with hypertension and hyperlipidemia, she smokes a pack and a half of cigarettes daily. She reports she has always been healthy and can’t believe she…
By: Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS Years ago, when I first started out in the wound care specialty, the only way to learn about new products and what was going on in the field was to “go to conference” (wound care conference). All year long, planning and excitement continued to build for our big trip. Not going…
By Cheryl Ericson, MS, RN, CCDS, CDIP Providers are often surprised at how pages upon pages of documentation in a patient’s health record can result in few reportable diagnosis and/or procedure codes, which often fail to capture the complexity of the patient’s condition. However, providers need to be aware of the implications of coding. As healthcare data become increasingly digital…
By Catherine R. Ratliff, PhD, APRN-BC, CWOCN, CFCN It’s estimated that about 70% of the 1 million ostomates in the United States and Canada will experience or have experienced stomal or peristomal complications. Peristomal complications are more common, although stomal complications (for example, retraction, stenosis, and mucocutaneous separation) can often contribute to peristomal problems by making it difficult to obtain…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. The crusting procedure produces a dry surface and absorbs moisture from broken skin through an artificial scab that’s created by using skin barrier powder (stoma powder) and liquid polymer skin barrier. The crusting procedure is…
By Rosalyn S. Jordan, BSN, RN, MSc, CWOCN, WCC, and Sandra Phipps, BSN, RN, MBA, WCC Pressure-ulcer prevention and management guidelines recommend support-surface therapy to help prevent and treat pressure ulcers. Support surfaces include pads, mattresses, and cushions that redistribute pressure. Full cushions and cushion pads are considered therapeutic support surfaces if used to redistribute a patient’s pressure in a…
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Prevention of pressure ulcers and skin breakdown begins with a comprehensive risk assessment. Most providers use a skin risk assessment tool, such as the Braden or Norton scale. While these tools have been validated to predict pressure ulcer development, their use alone isn’t considered a comprehensive assessment, and frequently the individual risk…
By Pamela Anderson, MS, RN, APN-BC, CCRN, and Terri Townsend, MA, RN, CCRN-CMC, CVRN-BC
Jan Smith, age 59, is admitted to the coronary intensive care unit with an acute inferior myocardial infarction (MI). Recently diagnosed with hypertension and hyperlipidemia, she smokes a pack and a half of cigarettes daily. She reports she has always been healthy and can’t believe she has had a heart attack. (Note: Name is fictitious.)
On physical exam, the cardiologist finds decreased femoral pulses bilaterally and recommends immediate cardiac catheterization. Fortunately, primary percutaneous coronary intervention (PCI) is readily available at this hospital. PCI is the preferred reperfusion method when it can be provided by skilled cardiologists in a timely manner.(more…)
Incidence density best measure of pressure-ulcer prevention program
According to the National Pressure Ulcer Advisory Panel (NPUAP), incidence density is the best quality measure of pressure-ulcer prevention programs. Pressure-ulcer incidence density is calculated by dividing the number of inpatients who develop a new pressure ulcer by 1,000 patient days. Using the larger denominator of patient days allows fair comparisons between institutions of all sizes. (more…)
By Joanne Aspiras Jovero, BSEd, BSN, RN; Hussam Al-Nusair, MSc Critical Care, ANP, RN; and Marilou Manarang, BSN, RN
A common problem in long-term care facilities, pressure ulcers are linked to prolonged hospitalization, pain, social isolation, sepsis, and death. This article explains how a Middle East rehabilitation facility battles pressure ulcers with the latest evidence-based practices, continual staff education, and policy and procedure updates. Sultan Bin Abdulaziz Humanitarian City (SBAHC) in Riyadh, Saudi Arabia, uses an interdisciplinary approach to address pressure-ulcer prevention and management. This article describes the programs, strategies, and preventive measures that have reduced pressure-ulcer incidence. (more…)
We’ve all experienced how a bad night’s sleep can affect our mood and ability to function the next day. Now imagine you’re a patient who has a pressure ulcer, most likely secondary to a declining disease state, and you’re being awakened and manipulated every 2 hours or in some cases hourly. How is your body supposed to recover without adequate sleep? (more…)
Antibiotics and conservative surgery yield similar outcomes in patients with diabetic foot osteomyelitis
A study in Diabetes Care finds that antibiotics and surgery have similar outcomes related to rate of healing, time of healing, and short-term complications in patients who have neuropathic forefoot ulcers and osteomyelitis, but no ischemia or necrotizing soft-tissue infections.