In the current healthcare environment, wound care practitioners need to capitalize on all available reimbursement avenues for care delivery and wound care supplies and dressings. And when it comes to reimbursement, there’s one constant: The rules change constantly. Whether these changes always benefit the patient is questionable. Nowhere is this more evident than in acute-care settings. Clinicians constantly are challenged to make sure their patient-care decisions comply with current Medicare reimbursement guidelines. (And if you’re not sure about today’s guidelines, be prepared for the guidelines to change tomorrow.) (more…)
Wound care has come a long way in just a few decades. With our expanded knowledge of wound healing and recent advances in treatment, we’re now able to assess wounds more accurately, recognize wound-related problems sooner, provide better interventions, and reduce morbidity.
To bring you up to date on current evidence-based wound management, this article focuses on assessing patients with chronic wounds, optimizing wound healing with effective wound-bed preparation, and selecting an appropriate dressing.
Wound chronicity and cause
Developing an appropriate plan of care hinges on conducting a thorough, accurate evaluation of both the patient and the wound. The first step is to determine whether the wound is acute or chronic.
• A chronic wound is one that fails to heal within a reasonable time—usually
3 months.
• An acute wound heals more quickly, causing minimal functional loss in the part of the body with the wound.
Identifying the cause of the wound also is essential. If the wound etiology is unknown, explore the patient’s medical history (including medication history) for clues to possible causes. Also review the patient’s history for conditions that could impede wound healing. (See What factors hamper healing? by clicking the PDF icon above)
Other important aspects of assessment include evaluating the patient’s nutritional status, quantifying the level of pain (if present), and gauging the patient’s self-care abilities.
General physical appearance
Conduct a general head-to-toe physical examination, focusing on the patient’s height, weight, and skin characteristics.
Height, weight, and weight trend
On admission, the patient’s height and weight should be measured to ensure appropriate nutritional and pharmacologic management. After a weight gain or loss, various factors may complicate wound healing. For instance, involuntary weight loss and protein-energy malnutrition may occur in both acute-care and long-term-care patients.
Especially note trends in your patient’s weight. For a long-term-care patient, a 5% weight loss over 30 days or a 10% loss over 180 days is considered involuntary. Arrange for a nutritional consult for any patient with an involuntary weight loss, as adequate nutrition is essential for general well-being and wound healing. (See A wound on the mend by clicking the PDF icon above.)
Skin color
Evaluate the patient’s skin color in light of ethnic background. If you note erythema—especially on a pressure point over a bony prominence—examine this area carefully for nonblanching erythema. Keep in mind that darkly pigmented skin doesn’t show such erythema and subsequent blanching, yet the patient may still be in jeopardy. So in dark-skinned patients, check for differences in skin color, temperature, or firmness compared to adjacent tissue; these differences may signify skin compromise.
Skin texture and turgor
Generally, healthy skin feels smooth and firm and has an even surface and good turgor (elasticity). To test turgor, gently grasp and pull up a fold of skin on a site such as the anterior chest below the clavicle. Does the skin return to place almost immediately after you release it, or does it stand up (“tent”)? Tenting indicates dehydration. But keep in mind that skin loses elasticity with age, so elderly patients normally have decreased turgor.
Skin temperature
With normal circulatory status, the skin is warm and its temperature is similar bilaterally. Areas of increased warmth or coolness suggest infection or compromised circulation. Be sure to check the temperature of skin surrounding the wound.
Wound assessment
Proper wound assessment can significantly influence patient outcome. Measure the wound carefully and document the condition of the wound bed. Remember that accurate descriptions are essential for guiding ongoing wound care. Repeat wound measurement and wound-bed assessment at least weekly, after the wound bed has been cleaned and debrided.
Keep in mind that assessing a chronic wound can be challenging. Wounds commonly have irregular shapes that can change quickly. Also, the multiple clinicians caring for the same patient may each describe the wound a bit differently.
Wound location
Note the precise anatomic location of the wound, as this can influence the wound care plan. A venous ulcer on the lower leg, for instance, requires different care than an arterial ulcer in the same site or a pressure ulcer on the ischium.
Circumference and depth
Use a paper or plastic measuring device to measure wound circumference and depth in centimeters (cm) or millimeters (mm). To promote accurate assessment of healing, be sure to use the same reference points each time you measure the wound.
You can use several methods to measure circumference. The most commonly used method of measurement is done in the head to toe direction. Measure the wound at its greatest length in that direction & measure the width at a 90 degree angle, at the widest point of the wound. Then multiply these two measurements (greatest length x greatest width) to obtain the total wound area. Although such linear measurements are imprecise, they yield gross information relative to wound healing when repeated over time.
Classify wound depth as partial thickness or full thickness.
• Partial-thickness wounds are limited to the skin layers and don’t penetrate the dermis. They usually heal by reepithelialization, in which epidermal cells regenerate and cover the wound. Abrasions, lacerations, and blisters are examples of partial-thickness wounds.
• Full-thickness wounds involve tissue loss below the dermis.
(Note: Pressure ulcers usually are classified by a four-stage system and diabetic foot ulcers by a grading system. Both systems are beyond this article’s scope.)
Measure and record wound depth based on the deepest area of tissue loss. To measure depth, gently place an appropriate device (such as a foam-tipped applicator) vertically in the deepest part of the wound, and mark the applicator at the patient’s skin level. Then measure from the end of the applicator to the mark to obtain depth.
Surrounding skin and tissue
Inspect for and document any erythema, edema, or ecchymosis within 4 cm of the wound edges, and reevaluate for these signs frequently. Because compromised skin near the wound is at risk for breakdown, preventive measures may be necessary.
Appearance of wound-bed tissue
Document viable tissue in the wound bed as granulation, epithelial, muscle, or subcutaneous tissue. Granulation tissue is connective tissue containing multiple small blood vessels, which aid rapid healing of the wound bed; appearing red or pink, it commonly looks shiny and granular. Epithelial tissue consists of regenerated epidermal cells across the wound bed; it may be shiny and silvery.
Check for nonviable tissue (also called necrotic, slough, or fibrin slough tissue), which may impede wound healing. It may vary in color from black or tan to yellow, and may adhere firmly or loosely to the wound bed. (See Picturing a necrotic wound by clicking the PDF icon above.)
Be sure to document the range of colors visible throughout the wound. Identify the color that covers the largest percentage of the wound bed. This color—and its significance—guide dressing selection.
Wound exudate
Document the amount, color, and odor of exudate (drainage) in the wound. Exudate with high protease levels and low growth factor levels may impede healing.
If the wound is covered by an occlusive dressing, assess exudate after the wound has been cleaned. Describe the amount of exudate as none, minimal, moderate, or heavy.
Describe exudate color as serous, serosanguineous, sanguineous, or purulent. Serous exudate is clear and watery, with no debris or blood present. Serosanguineous exudate is clear, watery, and tinged pink or pale red, denoting presence of blood. Sanguineous exudate is bloody, indicating active bleeding. Purulent exudate may range from yellow to green to brown or tan.
Describe wound odor as absent, faint, moderate, or strong. Note whether the odor is present only during dressing removal, if it disappears after the dressing is discarded, or if it permeates the room.
Wound edges
Wound edges indicate the epithelialization trend and suggest the possible cause and chronicity of the wound. The edges should attach to the wound bed. Edges that are rolled (a condition called epibole) indicate a chronic wound, in which epithelial cells are unable to adhere to a moist, healthy wound bed and can’t migrate across and resurface the wound.
Undermining and tracts
Gently probe around the wound edges and in the wound bed to check for undermining and tracts. Undermining, which may occur around the edges, presents as a space between the intact skin and wound bed (resembling a roof over part of the wound). It commonly results from shear forces in conjunction with sustained pressure. A tract, or tunnel, is a channel extending from one part of the wound through subcutaneous tissue or muscle to another part.
Measure the depth of a tract or undermining by inserting an appropriate device into the wound as far as it will go without forcing it. Then mark the skin on the outside where you can see or feel the applicator tip. Document your findings based on a clock face, with 12 o’clock representing the patient’s head and 6 o’clock denoting the feet. For instance, you might note “2.0-cm undermining from 7:00 to 9:00 position.”
Pain level
Ask the patient to quantify the level of pain caused by the wound, using the pain scale designated by your facility. Find out which pain-management techniques have relieved your patient’s pain in the past; as appropriate, incorporate these into a pain-management plan. Reevaluate the patient’s pain level regularly.
Wound-bed preparation
An evolving science, wound-bed preparation is crucial for minimizing or removing barriers to healing. The goal is to minimize factors that impair healing and maximize the effects of wound care. The key elements of wound-bed preparation are controlling bioburden and maintaining moisture balance. (For online resources on wound-bed preparation and other wound-care topics, see Where to get more information by clicking the PDF icon above.)
Controlling bioburden
Necrotic tissue and exudate harbor bacteria. A wound’s bioburden—the number of contaminating microbes—contributes to poor healing. All chronic wounds are considered contaminated or colonized, but not necessarily infected. In a colonized wound, healing is impeded as bacteria compete for nutrients; also, bacteria have harmful byproducts. To control bioburden, the wound must be cleaned and necrotic tissue must be debrided.
Cleaning the wound. Clean the wound before assessing it and applying a dressing. Use a noncytotoxic agent (typically, potable water, normal saline irrigating solution, or an appropriate wound-cleaning agent). Antiseptic solutions generally aren’t recommended for wound irrigation or dressings because they’re toxic to fibroblasts and other wound-repairing cells. If you must use such a solution, make sure it’s well diluted.
To ensure gentle cleaning or irrigation, pour solution over the wound bed or gently flush the wound with solution (using a 60-mL catheter-tip syringe) until the drainage clears. Know that pressurized irrigation techniques and whirlpool therapy aren’t recommended for wound cleaning because they disturb cell proliferation in the wound bed.
Debriding the wound. Debridement removes slough and necrotic tissue. Nonselective debridement techniques remove any type of tissue within the wound bed, whereas selective methods remove only necrotic tissue. (See Wound debridement techniques by clicking the PDF icon below.)
Maintaining moisture balance
To maintain moisture balance in the wound bed, you must manage exudate and keep the wound bed moist. The proper dressing (which may stay in place for days or longer) supports moist wound healing and exudate management. To minimize fluid pooling, a drain may be inserted into the wound. Negative-pressure wound therapy also may aid removal of excess exudate.
Choosing an appropriate dressing
The wound dressing plays a major role in maintaining moisture balance. Dressing selection is challenging because of the large number and variety of dressings available. Each product has specific actions, benefits, and drawbacks, so determining which dressing best suits the patient’s needs is a multifaceted process.
Dressing choice depends on such factors as wound type and appearance, exudate, presence or absence of pain, and required dressing change frequency. (See Dressings Options by clicking the PDF icon above.)
In a traditional dressing, gauze is applied in layers. The initial (contact) layer in the wound bed absorbs drainage and wicks it to the next layer; most often, this layer consists of woven cotton gauze or synthetic gauze. Remove the gauze gently, because it may be stuck to the wound or incision (especially if the gauze is cotton). For easier removal, moisten the dressing with normal saline solution to loosen it.
With a traditional dressing, the cover layer or secondary dressing is an abdominal pad with a “no-strike-through” layer next to the outside of the dressing. Be aware that wet-to-dry dressings are highly discouraged for their nonselective debriding effect and inability to provide a moist wound bed.
Reassess the patient’s wound at least weekly (after preparing the wound bed and dressing the wound) to determine healing progress. Keep in mind that wound-care management is a collaborative effort. Once you’ve assessed the patient, discuss your findings and subsequent wound management with other members of the team.
Wound care wisdom
Getting wiser about wound care will help your patients achieve good outcomes. Poor wound healing can be frustrating to patients, family members, and healthcare providers alike. Chronic wounds may necessitate lifestyle changes and lead to severe physical consequences ranging from infection to loss of function and even death. By performing careful assessment, tailoring patients’ wound care to wound etiology, and using evidence-based protocols to manage wounds, you can promote speedier wound healing, help lower morbidity, and improve quality of life.
Selected references
Bryant RA, Nix DP. Acute and Chronic Wounds: Current Management Concepts. 4th ed. St. Louis, MO: Mosby; 2011.
Gardener SE, Frantz R, Hillis SL, Park H, Scherubel M. Diagnostic validity of semiquantitative swab cultures. Wounds. 2007;(19)2:31-38.
Krasner DL, Rodeheaver GT, Sibbald RG. Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. 4th ed. Wayne, PA: HMP Communications; 2007.
Langemo DK, Brown G. Skin fails too: acute, chronic, and end-stage skin failure. Adv Skin Wound Care. 2006;19(4):206-211.
Langemo DK, Anderson J, Hanson D, Hunter S, Thompson P. Measuring wound length, width, and area: which technique? Adv Skin Wound Care. 2008;21:42-45.
Milne C, Armand OC, Lassie M. A comparison of collagenase to hydrogel dressings in wound debridement. Wounds. 2010:22(11):270-274.
National Pressure Ulcer Advisory Panel and European Pressure Ulcer Advisory Panel. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Washington, DC: National Pressure Ulcer Advisory Panel; 2009.
Ovington LG. Hanging wet-to-dry dressings out to dry. Adv Skin Wound Care. 2002;15(2):79-86.
Sibbald RG, Coutts P, Woo KY. Reduction of bacterial burden and pain in chronic wounds using a new polyhexamethylene biguanide antimicrobial foam dressing—clinical trial results. Adv Skin Wound Care. 2011;24(2):78-84.
Solway DR, Consalter M, Levinson DJ. Microbial cellulose wound dressing in the treatment of skin tears in the frail elderly. Wounds. 2010:22(1):17-19.
Wound Ostomy and Continence Nurses Society. Guideline for Prevention and Management of Pressure Ulcers. Mt. Laurel, NJ: Author; 2010
Patricia A. Slachta is a Clinical Nurse Specialist at The Queens Medical Center in Honolulu, Hawaii and an adjunct nursing instructor at the Technical College of the Lowcountry in Beaufort, South Carolina.
Hansen’s disease, also called leprosy, is treatable today – and that’s partly thanks to a curious tree and the work of a pioneering young scientist in the 1920s. Centuries prior to her discovery, sufferers had no remedy for leprosy’s debilitating symptoms or its social stigma.
This young scientist, Alice Ball, laid fundamental groundwork for the first effective leprosy treatment globally. But her legacy still prompts conversations about the marginalization of women and people of color in science today.
Alice Augusta Ball, born in Seattle, Washington, in 1892, became the first woman and first African American to earn a master’s degree in science from the College of Hawaii in 1915, after completing her studies in pharmaceutical chemistry the year prior.
After she finished her master’s degree, the college hired her as a research chemist and instructor, and she became the first African American with that title in the chemistry department.
Doctors now understand that leprosy, also called Hansen’s disease, is minimally contagious. But in 1865, the fear and stigma associated with leprosy led authorities in Hawaii to implement a mandatory segregation policy, which ultimately isolated those with the disease on a remote peninsula on the island of Molokai. In 1910, over 600 leprosy sufferers were living in Molokai.
Doctors had attempted to use nearly every remedy imaginable to treat leprosy, even experimenting with dangerous substances such as arsenicand strychnine. But the lone consistently effective treatment was chaulmoogra oil.
Chaulmoogra oil is derived from the seeds of the chaulmoogra tree. Health practitioners in India and Burma had been using this oil for centuries as a treatment for various skin diseases. But there were limitations with the treatment, and it had only marginal effects on leprosy.
The oil is very thick and sticky, which makes it hard to rub into the skin. The drug is also notoriously bitter, and patients who ingested it would often start vomiting. Some physicians experimented with injections of the oil, but this produced painful pustules.
Dr. Isabel Kerr, a European missionary, administering to a patient a chaulmoogra oil treatment in 1915, prior to the invention of the Ball Method. George McGlashan Kerr, CC BY
The Ball Method
If researchers could harness chaulmoogra’s curative potential without the nasty side effects, the tree’s seeds could revolutionize leprosy treatment. So, Hollmann turned to Ball. In a 1922 article, Hollmann documents how the 23-year-old Ball discovered how to chemically adapt chaulmoogra into an injection that had none of the side effects.
The Ball Method, as Hollmann called her discovery, transformed chaulmoogra oil into the most effective treatment for leprosy until the introduction of sulfones in the late 1940s.
In 1920, the Ball Method successfully treated 78 patients in Honolulu. A year later, it treated 94 more, with the Public Health Service noting that the morale of all the patients drastically improved. For the first time, there was hope for a cure.
Ball’s death meant she didn’t have the opportunity to publish her research. Arthur Dean, chair of the College of Hawaii’s chemistry department, took over the project.
Dean mass-produced the treatment and published a series of articles on chaulmoogra oil. He renamed Ball’s method the “Dean Method,” and he never credited Ball for her work.
Ball’s other colleagues did attempt to protect Ball’s legacy. A 1920 article in the Journal of the American Medical Association praises the Ball Method, while Hollmann clearly credits Ball in his own 1922 article.
Ball is described at length in a 1922 article in volume 15, issue 5, of Current History, an academic publication on international affairs. That feature is excerpted in a June 1941 issue of Carter G. Woodson’s “Negro History Bulletin,” referring to Ball’s achievement and untimely death.
Joseph Dutton, a well-regarded religious volunteer at the leprosy settlements on Molokai, further referenced Ball’s work in a 1932 memoir broadly published for a popular audience.
Historians such as Paul Wermager later prompted a modern reckoning with Ball’s poor treatment by Dean and others, ensuring that Ball received proper credit for her work. Following Wermager’s and others’ work, the University of Hawaii honored Ball in 2000 with a bronze plaque, affixed to the last remaining chaulmoogra tree on campus.
In 2019, the London School of Hygiene and Tropical Medicine added Ball’s name to the outside of its building. Ball’s story was even featured in a 2020 short film, “The Ball Method.”
The Ball Method represents both a scientific achievement and a history of marginalization. A young woman of color pioneered a medical treatment for a highly stigmatizing disease that disproportionately affected an already disenfranchised Indigenous population.
In 2022, then-Gov. David Ige declared Feb. 28 Alice Augusta Ball Day in Hawaii. It was only fitting that the ceremony took place on the Mānoa campus in the shade of the chaulmoogra tree.
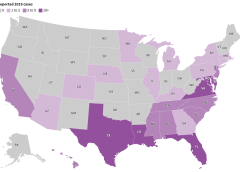
The word “leprosy” conjures images of biblical plagues, but the disease is still with us today. Caused by infectious bacteria, some 200,000 new cases are reported each year, according to the World Health Organization. In the United States, leprosy has been entrenched for more than a century in parts of the South where people came into contact with armadillos, the principle proven linkage from animal to humans. However, the more recent outbreaks in the Southeast, especially Florida, have not been associated with animal exposure.
The Conversation talked with Robert A. Schwartz, professor and head of dermatology at Rutgers New Jersey Medical School, to explain what researchers know about the disease.
What is leprosy and why is it resurfacing in the US?
Leprosy is caused by two different but similar bacteria — Mycobacterium leprae and Mycobacterium lepromatosis — the latter having just been identified in 2008. Leprosy, also known as Hansen’s disease, is avoidable. Transmission among the most vulnerable in society, including migrant and impoverished populations, remains a pressing issue.
Leprosy is beginning to occur regularly within parts of the southeastern United States. Most recently, Florida has seen a heightened incidence of leprosy, accounting for many of the newly diagnosed cases in the U.S.
Traditional risk factors include zoonotic exposure and having recently lived in leprosy-endemic countries. Brazil, India and Indonesia have each noted more than 10,000 new cases since 2019, according to the World Health Organization data, and more than a dozen countries have reported between 1,000 to 10,000 new cases over the same time period.
From that time until the mid-20th century, limited treatments were available, so the bacteria could infiltrate the body and cause prominent physical deformities such as disfigured hands and feet. Advanced cases of leprosy cause facial features resembling that of a lion in humans.
Many mutilating and distressing skin disorders such as skin cancers and deep fungal infections were also confused with leprosy by the general public.
Fear of contagion has led to tremendous stigmatization and social exclusion. It was such a serious concern that the Kingdom of Jerusalem had a specialized hospital to care for those suffering from leprosy.
How infectious is leprosy?
Research shows that prolonged in-person contact via respiratory droplets is the primary mode of transmission, rather than through normal, everyday contact such as embracing, shaking hands or sitting near a person with leprosy. People with leprosy generally do not transmit the disease once they begin treatment.
Armadillos represent the only known zoonotic reservoir of leprosy-causing bacteria that threaten humans. These small mammals are common in Central and South America and in parts of Texas, Louisiana, Missouri and other states, where they are sometimes kept as pets or farmed as meat. Eating armadillo meat is not a clear cause of leprosy, but capturing and raising armadillos, along with preparing its meat, are risk factors.
The transmission mechanism between zoonotic reservoirs and susceptible individuals is unknown, but it is strongly suspected that direct contact with an infected armadillo poses a significant risk of developing leprosy. However, many cases reported in the U.S. have demonstrated an absence of either zoonotic exposure or person-to-person transmission outside of North America, suggesting that transmission may be happening where the infected person lives. But in many cases, the source remains an enigma.
Leprosy primarily affects the skin and peripheral nervous system, causing physical deformity and desensitizing one’s ability to feel pain on affected skin.
It may begin with loss of sensation on whitish patches of skin or reddened skin. As the bacteria spread in the skin, they can cause the skin to thicken with or without nodules. If this occurs on a person’s face, it may rarely produce a smooth, attractive-appearing facial contour known as lepra bonita, or “pretty leprosy.” The disease can progress to causing eyebrow loss, enlarged nerves in the neck, nasal deformities and nerve damage.
The onset of symptoms can sometimes take as long as 20 years because the infectious bacteria have a lengthy incubation period and proliferate slowly in the human body. So presumably many people are infected long before they know that they are.
Fortunately, worldwide efforts to screen for leprosy are being enhanced thanks to organizations like the Order of Saint Lazarus, which was originally founded in the 11th century to combat leprosy, and the Armauer Hansen Research Institute, which conducts immunologic, epidemiological and translational research in Ethiopia. The nongovernmental organization Bombay Leprosy Project in India does the same.
How treatable is it?
Leprosy is not only preventable but treatable. Defying stigma and advancing early diagnosis via proactive measures are critical to the mission of controlling and eradicating it worldwide.
Notably, the World Health Organization and other agencies provide multi-drug therapy at no cost to patients.
In addition, vaccine technology to combat leprosy is in the clinical trials stage and could become available in coming years. In studies involving nine-banded armadillos, this protein-based vaccine delayed or diminished leprous nerve damage and kept bacteria at bay. Researchers believe that the vaccine can be produced in a low-cost, highly efficient manner, with the long-term prospect of eradicating leprosy.
If health care professionals, biomedical researchers and lawmakers do not markedly enhance their efforts to eliminate leprosy worldwide, the disease will continue to spread and could become a far more serious problem in areas that have been largely free of leprosy for decades.
The World Health Organization launched a plan in 2021 for achieving zero leprosy.
Flesh-eating bacteria sounds like the premise of a bad horror movie, but it’s a growing – and potentially fatal – threat to people.
In September 2023, the Centers for Disease Control and Prevention issued a health advisory alerting doctors and public health officials of an increase in flesh-eating bacteria cases that can cause serious wound infections.
There are several types of bacteria that can infect open wounds and cause a rare condition called necrotizing fasciitis. These bacteria do not merely damage the surface of the skin – they release toxins that destroy the underlying tissue, including muscles, nerves and blood vessels. Once the bacteria reach the bloodstream, they gain ready access to additional tissues and organ systems. If left untreated, necrotizing fasciitis can be fatal, sometimes within 48 hours.
The bacterial species group A Streptococcus, or group A strep, is the most common culprit behind necrotizing fasciitis. But the CDC’s latest warning points to an additional suspect, a type of bacteria called Vibrio vulnificus. There are only 150 to 200 cases of Vibrio vulnificus in the U.S. each year, but the mortality rate is high, with 1 in 5 people succumbing to the infection.
How do you catch flesh-eating bacteria?
Vibrio vulnificus primarily lives in warm seawater but can also be found in brackish water – areas where the ocean mixes with freshwater. Most infections in the U.S. occur in the warmer months, between May and October. People who swim, fish or wade in these bodies of water can contract the bacteria through an open wound or sore.
Vibrio vulnificus can also get into seafood harvested from these waters, especially shellfish like oysters. Eating such foods raw or undercooked can lead to food poisoning, and handling them while having an open wound can provide an entry point for the bacteria to cause necrotizing fasciitis. In the U.S., Vibrio vulnificus is a leading cause of seafood-associated fatality.
Why are flesh-eating bacteria infections rising?
Vibrio vulnificus is found in warm coastal waters around the world. In the U.S., this includes southern Gulf Coast states. But rising ocean temperatures due to global warming are creating new habitats for this type of bacteria, which can now be found along the East Coast as far north as New York and Connecticut. A recent study noted that Vibrio vulnificus wound infections increased eightfold between 1988 and 2018 in the eastern U.S.
Climate change is also fueling stronger hurricanes and storm surges, which have been associated with spikes in flesh-eating bacteria infection cases.
Aside from increasing water temperatures, the number of people who are most vulnerable to severe infection, including those with diabetes and those taking medications that suppress immunity, is on the rise.
What are symptoms of necrotizing fasciitis? How is it treated?
Early symptoms of an infected wound include fever, redness, intense pain or swelling at the site of injury. If you have these symptoms, seek medical attention without delay. Necrotizing fasciitis can progress quickly, producing ulcers, blisters, skin discoloration and pus.
Treating flesh-eating bacteria is a race against time. Clinicians administer antibiotics directly into the bloodstream to kill the bacteria. In many cases, damaged tissue needs to be surgically removed to stop the rapid spread of the infection. This sometimes results in amputation of affected limbs.
Researchers are concerned that an increasing number of cases are becoming impossible to treat because Vibrio vulnificus has evolved resistance to certain antibiotics.
People who have a fresh cut, including a new piercing or tattoo, are advised to stay out of water that could be home to Vibrio vulnificus. Otherwise, the wound should be completely covered with a waterproof bandage.
People with an open wound should also avoid handling raw seafood or fish. Wounds that occur while fishing, preparing seafood or swimming should be washed immediately and thoroughly with soap and water.
Anyone can contract necrotizing fasciitis, but people with weakened immune systems are most susceptible to severe disease. This includes people taking immunosuppressive medications or those who have pre-existing conditions such as liver disease, cancer, HIV or diabetes.
It is important to bear in mind that necrotizing fasciitis presently remains very rare. But given its severity, it is beneficial to stay informed.
Debbie King barely gave it a second thought when she scraped her right shin climbing onto her friend’s pontoon for a day of boating in the Gulf of Mexico on Aug. 13.
Even though her friend immediately dressed the slight cut, her shin was red and sore when King awoke the next day. It must be a sunburn, she thought.
But three days later, the red and blistered area had grown. Her doctor took one look and sent King, 72, to the emergency room.
Doctors at HCA Florida Citrus Hospital in Inverness, Florida, rushed King into surgery after recognizing the infection as Vibrio vulnificus, a potentially fatal bacterium that kills healthy tissue around a wound. While King lay on the operating table, the surgeon told her husband she would likely die if they didn’t amputate.
Just four days after the scrape, King lost her leg then spent four days in intensive care.
“The flesh was gone; it was just bone,” she said of her leg.
Cases of V. vulnificus are rare. Between 150 and 200 are reported to the Centers for Disease Control and Prevention every year, with about 20% resulting in death. Most are in states along the Gulf of Mexico, but, in 2019, 7% were on the Pacific Coast. Florida averages about 37 cases and 10 deaths a year.
But a rise in cases nationally and the spread of the disease to states farther north — into coastal communities in states such as Connecticut, New York, and North Carolina — have heightened concerns about the bacterium, which can result in amputations or extensive removal of tissue even in those who survive its infections. And warmer coastal waters caused by climate change, combined with a growing population of older adults, may result in infections doubling by 2060, a study in Scientific Reports warned earlier this year.
“Vibrio distributions are driven in large part by temperature,” said Tracy Mincer, an assistant professor at Florida Atlantic University. “The warmer waters are, the more favorable it is for them.”
The eastern United States has seen an eightfold increase in infections over a 30-year period through 2018 as the geographic range of infections shifted north by about 30 miles a year, according to the study, which was cited in a CDC health advisory last month.
The advisory was intended to make doctors more aware of the bacterium when treating infected wounds exposed to coastal waters. Infections can also arise from eating raw or undercooked seafood, particularly oysters, it warned. That can cause symptoms as common as diarrhea and as serious as bloodstream infections and severe blistered skin lesions.
New York and Connecticut this summer issued health warnings about the risk of infection as well. It’s not the first year either state has recorded cases.
“There’s very few cases but when they happen, they’re devastating,” said Paul A. Gulig, a professor in the Department of Molecular Genetics and Microbiology at the University of Florida College of Medicine.
‘An Accident of Nature’
Vibrio has more than 100 strains, including the bacterium that causes cholera, a disease that causes tens of thousands of deaths worldwide each year.
The V. vulnificus strain likes warm brackish waters close to shorelines where the salinity is not as high as in the open sea. Unlike some other Vibrio strains, it has no mechanism to spread between humans.
It’s found in oysters because the mollusks feed by filtering water, meaning the bacterium can become concentrated in oyster flesh. It can enter humans who swim in salty or brackish waters through the slightest cut in the skin. Infections are treated with antibiotics and, if needed, surgery.
“It’s almost an accident of nature,” Gulig said. “They have all these virulence factors that make them really destructive, but we’re not a part of this bug’s life cycle.”
Once inside the human body, the bacteria thrive.
Scientists don’t believe the bacteria eat flesh, despite how they’re often described. Rather, enzymes and toxins secreted by the bacterium as it multiplies break down the human tissue in the area below the skin, causing necrosis, or death of tissue cells.
The infection spreads like wildfire, Gulig said, making early detection critical.
“If you take a pen and mark where the edge of the redness is and then look at that two or four hours later, the redness would have moved,” Gulig said. “You can almost sit there and watch this spread.”
Researchers have conducted studies on the bacteria, but the small number of cases and deaths make it tough to secure funding, said Gulig. He said he switched his research focus to other areas because of the lack of money.
But growing interest in the bacteria has prompted talk about new research at his university’s Emerging Pathogens Institute.
Examining the bacteria’s genome sequence and comparing it with those of Vibrio strains that don’t attack human flesh could yield insights into potential drugs to interfere with that process, Gulig said.
Shock and Loss
Inside the operating room at HCA Florida Citrus, the only signs of King’s infection were on her shin. The surgeon opened that area and began cutting away a bright red mush of dead flesh.
Hoping to save as much of the leg as possible, the doctor first amputated below her knee.
But the bacteria had spread farther than doctors had hoped. A second amputation, this time 5 inches above the knee, had to be performed.
After surgery, King remained in critical care for four days with sepsis, a reaction to infection that can cause organs to fail.
Her son was there when she awakened. He was the one who told her she had lost her leg, but she was too woozy from medication to take it in.
It wasn’t until she was transferred to a rehab hospital in nearby Brooksville run by Encompass Health that the loss sank in.
A former radiation protection technician, King had always been self-reliant. The idea of needing a wheelchair, of being dependent on others — it felt like she had lost part of her identity.
One morning, she could just not stop crying. “It hit me like a ton of bricks,” she said.
Six different rehab staffers told her she needed to meet with the hospital’s consulting psychologist. She thought she didn’t need help, but she eventually gave in and met with Gerald Todoroff.
In four sessions with King, he said, he worked to redirect her perception of what happened. Amputation is not who you are but what you will learn to deal with, he told her. Your life can be as full as you wish.
“They were magic words that made me feel like a new person,” King said. “They went through me like music.”
Physical therapy moved her forward, too. She learned how to stand longer on her remaining leg, to use her wheelchair, and to maneuver in and out of a car.
Now, back in her Gulf Coast community of Homosassa, those skills have become routine. Her husband, Jim, a former oil company worker and carpenter, built an access ramp out of concrete and pressure-treated wood for their single-story home.
But she is determined to walk with the aid of a prosthetic leg. It’s the motivation for a one-hour regimen of physical therapy she does on her own every day in addition to twice-weekly sessions with a physical therapist.
Recovery still feels like a journey but one marked by progress. She has nicknamed her “stump” Peg. She’s now comfortable sharing before and after pictures of her leg.
And she’s made it her mission to talk about what happened so more people will learn about the danger.
“This is the most horrific thing that can happen to anybody,” she said. “But I’d sit back and think, ‘God put you here for a reason — you’ve got more things to do.’”
What to Know About ‘Flesh-Eating’ Bacterium Vibrio vulnificus
Infection Symptoms:
Diarrhea, often accompanied by stomach cramping, nausea, vomiting, and fever.
Wound infections cause redness, pain, swelling, warmth, discoloration, and discharge. They may spread to the rest of the body and cause fever.
Bloodstream infections cause fever, chills, dangerously low blood pressure, and blistering skin lesions.
To Protect Against Vibrio Infections:
Stay out of saltwater or brackish water if you have a wound or a recent surgery, piercing, or tattoo.
Cover wounds with a waterproof bandage if they could come into contact with seawater or raw or undercooked seafood and its juices.
Wash wounds and cuts thoroughly with soap and water after contact with saltwater, brackish water, raw seafood, or its juices.
Who Is Most at Risk:
Anyone can get a wound infection. People with liver disease, cancer, or diabetes, and those over 40 or with weakened immune systems, are more likely to get an infection and have severe complications.
This article was produced in partnership with the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
The Indications and Contraindications for Collagen
What a Wound Wants and Needs; and Why
Considerations of Collagen in Treating & Healing Wounds
Our Speaker: Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).
As a visionary and entrepreneur in the field of mobile medicine, she has operated mobile wound care practices nationwide for many years. She enjoys educating on the art and science of wound healing and how practical solutions apply to healthcare professionals today. Martha enjoys being a positive change in healthcare impacting clients suffering from wounds and skin issues of all etiologies.
Submit below to view the Webinar and download Slidedeck
*By accessing this webinar you are opting in to receiving information from Healthcom Media and Affiliates. Or the details, including your email address/mobile number, may be used to keep you informed about future products and services.
Why All the (pH)uss About Microenvironments?
The Importance of Acidic pH on Wound Healing Why All the (pH)uss About Microenvironments? By Martha Kelso, RN, HBOT, CEO, WCP The Wound Microenvironment Every wound or ulcer has factors that influence the wound bed environment and how it reacts. Many of these factors occur at a microscopic level and therefore can be referred to as the wound microenvironment. Inside this microenvironment, factors are at play that influence whether a wound heals or becomes chronically stalled.
The Importance of Acidic pH on Wound Healing Why All the (pH)uss About Microenvironments? By Martha Kelso, RN, HBOT, CEO, WCP The Wound Microenvironment Every wound or ulcer has factors that influence the wound bed environment and how it reacts. Many of these factors occur at a microscopic level and therefore can be referred to as the wound microenvironment. Inside this microenvironment, factors are at play that influence whether a wound heals or becomes chronically stalled.
American Nurse Today, Woundcare Advisor and Angelini present: Innovations in Wound Care: Case Studies Basic Wound Cleansing and use of Collagen in Diabetic Foot Ulcer
This 30-minute presentation featurea learning opportunities that will provide in-depth instruction and demonstration in wound care treatments. After this webinar, the learner will be able to:
Identify the role of proper wound cleansing
Discuss how to select and use non-toxic wound cleansers
Describe advantages of collagen for managing a chronic wound
Martha Kelso, RN, HBOT, CEO, WCP Wound Care Plus, LLC, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP). As a visionary and entrepreneur in the field of mobile medicine, she has operated mobile wound care practices nationwide for many years. She enjoys educating on the art and science of wound healing and how practical solutions apply to healthcare professionals today. Martha enjoys being a positive change in healthcare impacting clients suffering from wounds and skin issues of all etiologies. Martha started her career as a Certified Nurse Aide at the age of 15 in Kansas before moving to Kansas City, MO to attend nursing school. Long Term Care nursing was her first love and her biggest challenge.






 Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).
Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).
 Martha Kelso, RN, HBOT, CEO, WCP Wound Care Plus, LLC, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP). As a visionary and entrepreneur in the field of mobile medicine, she has operated mobile wound care practices nationwide for many years. She enjoys educating on the art and science of wound healing and how practical solutions apply to healthcare professionals today. Martha enjoys being a positive change in healthcare impacting clients suffering from wounds and skin issues of all etiologies. Martha started her career as a Certified Nurse Aide at the age of 15 in Kansas before moving to Kansas City, MO to attend nursing school. Long Term Care nursing was her first love and her biggest challenge.
Martha Kelso, RN, HBOT, CEO, WCP Wound Care Plus, LLC, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP). As a visionary and entrepreneur in the field of mobile medicine, she has operated mobile wound care practices nationwide for many years. She enjoys educating on the art and science of wound healing and how practical solutions apply to healthcare professionals today. Martha enjoys being a positive change in healthcare impacting clients suffering from wounds and skin issues of all etiologies. Martha started her career as a Certified Nurse Aide at the age of 15 in Kansas before moving to Kansas City, MO to attend nursing school. Long Term Care nursing was her first love and her biggest challenge.