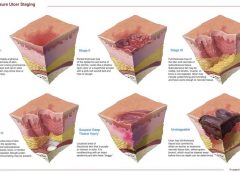
Pressure ulcers have been a health concern for a long time—since at least 5,000 years ago, when evidence of a pressure ulcer was found on an ancient Egyptian mummy. But not until 1975 did the staging classification system we’re familiar with begin. This system was designed to make things easier by creating a universal way to describe and communicate the various levels of tissue destruction. (more…)
Like many hospitals, Houston Methodist San Jacinto Hospital uses national benchmarks such as the National Database of Nursing Quality Indicators (NDNQI®) to measure quality outcomes. Based on benchmark reports that showed an increased trend of pressure ulcers in critically ill patients in our hospital, the clinical nurses in our Critical Care Shared Governance Unit-Based Council (CCSGUBC) identified an improvement opportunity. (more…)
I’m one of the nurses responsible for the pressure ulcer prevention education program at the 150-bed skilled nursing facility where I work. We try to keep education sessions simple, fun, and interactive. One day, our administrator asked us to develop a crossword puzzle and “minute to win it” education game that would be appropriate for all staff—registered nurses, licensed practical nurses, certified nursing assistants, and staff from administration, the business office, scheduling, maintenance, dietary, and housekeeping. (more…)
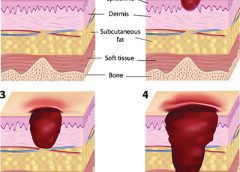
A declining pressure ulcer decreases the quality of life for patients and places providers at risk for regulatory citations and litigation. But it’s important for clinicians to determine whether the first appearance of skin injury is truly a stage I or II pressure ulcer or if it’s a deep tissue injury (DTI), a unique staging category for a pressure ulcer. Otherwise, a clinician might think a pressure ulcer is getting worse instead of the change being the normal progression of a pressure ulcer that is presenting as a DTI. (more…)
As a senior quality improvement specialist with IPRO, the Quality Improvement Organization for New York State over the past 11 years, I’ve been tasked with helping skilled nursing facilities (SNFs) embrace the process of continuous quality improvement. A necessary component of this effort has been to collect, understand, and analyze timely and accurate data. This article discusses a free tool I developed to help SNFs track their data related to pressure ulcers and focus their quality improvement efforts for the greatest impact. (more…)
As a wound care nurse, do you feel the weight of the world on your shoulders when trying to implement a pressure ulcer prevention program? Many staff members think it’s up to the wound care nurse alone to implement the program. However, a successful program requires involvement from all staff and is a 24/7 endeavor. Here’s how to do it. (more…)
A medical device–related pressure ulcer (MDRPU) is defined as a localized injury to the skin or underlying tissue resulting from sustained pressure caused by a medical device, such as a brace; splint; cast; respiratory mask or tubing; tracheostomy tube, collar, or strap; feeding tube; or a negative-pressure wound therapy device. The golden rule of pressure ulcer treatment is to identify the cause of pressure and remove it. Unfortunately, many of the medical devices are needed to sustain the patient’s life, so they can’t be removed. (more…)
By Joanne Aspiras Jovero, BSEd, BSN, RN; Hussam Al-Nusair, MSc Critical Care, ANP, RN; and Marilou Manarang, BSN, RN
A common problem in long-term care facilities, pressure ulcers are linked to prolonged hospitalization, pain, social isolation, sepsis, and death. This article explains how a Middle East rehabilitation facility battles pressure ulcers with the latest evidence-based practices, continual staff education, and policy and procedure updates. Sultan Bin Abdulaziz Humanitarian City (SBAHC) in Riyadh, Saudi Arabia, uses an interdisciplinary approach to address pressure-ulcer prevention and management. This article describes the programs, strategies, and preventive measures that have reduced pressure-ulcer incidence. (more…)
The first 24 hours after a patient’s admission are critical in preventing pressure ulcer development or preventing an existing ulcer from worsening. A skin inspection, risk assessment, and temporary care plan should all be implemented during this time frame. Essentially, it’s the burden of the care setting to prove to insurers, regulators, and attorneys the pressure ulcer was present on admission and interventions were put into place to avoid worsening of the condition. Of course, patients also benefit from having their condition identified and treated promptly. (more…)
The Affordable Care Act of 2010 requires nursing homes to have an acceptable Quality Assurance and Performance Improvement (QAPI) plan within a year after the start of the QAPI regulation. While the implementation of this regulation may be a year out, now is the time to start applying its principles. Reducing pressure ulcer rates is a great program to target for a QAPI plan.
A team approach
If you decide to use pressure ulcers as your QAPI project, don’t take on your entire program at once. Break the program down into system subsets (for example, admission process, prevention program, and weekly rounds). Determining the status of your program in each subset—completed, needs improvement, or not completed—can help you prioritize which areas to target. It’s important you have support from leadership for your efforts.
I’ll use the example of the admission phase (ensuring that within the first 24 hours, skin and risk concerns are identified and a temporary plan of care is implemented) to illustrate a QAPI project. To address this area, a team was created, including representation from staff members involved with the admission process. The team then used the problem-solving model Plan-Do-Study-Act (PDSA) to examine the process.
The first step in the PDSA cycle is to Plan. During this step, you:
• evaluate and analyze the current process to determine baseline data, which are used to measure progress
• identify system performance gaps
• determine the root cause of the performance gaps
• develop an action plan that identifies the goals, steps, responsible staff, and target dates.
In our example, the team determined that within the first 24 hours, skin inspections were being completed only 10% of the time. The root-cause analysis revealed that the admission nurses didn’t feel competent to document identified pressure ulcers or skin concerns, so they deferred it until the wound nurse was available. The team’s action plan included the following:
• Develop and educate all the facility nurses on how to complete and accurately document a skin inspection.
• Develop and implement a competency evaluation to assess the nurse’s ability to apply the knowledge at the bedside.
• Develop an ongoing plan to ensure all nurses receive this education during orientation and yearly thereafter.
The team also set the following goal:
By the end of the next quarter, 100% of admitted patients will have an accurate skin inspection completed within 24 hours of admission.
The second step of the PDSA cycle is Do. During this step, you implement and execute the plan, while documenting your observations and recording data.
In our example, the “Do” was to:
• develop and provide the skin inspection education and bedside competency evaluations
• develop an evaluation and tracking
system
• add the education to the orientation program
• add the education to the staff development calendar to be offered yearly.
The third step of the PDSA cycle is to Study: In this phase, you:
• reevaluate and analyze the system
• compare the results with the baseline data and predictions
• summarize what was learned and accomplished and what needs to be improved
• determine if another PDSA cycle is
necessary to continue to improve the system.
Once all staff had been properly educated and competency testing completed, an analysis of the rate and accuracy of the admission skin inspections done within 24 hours of admission was completed. It was found that 100% of the patients admitted had a complete skin inspection done within 24 hours. However, not all the nurses could accurately stage pressure ulcers, so it was determined that the system needed improvement to ensure accurate assessments.
The last step of the PDSA cycle is to Act. In this step, you:
• determine what changes need to be made
• modify the plan to continue to improve the system
• repeat the PDSA cycle as necessary.
In our example, the team determined the nurses needed more guidance and education on staging of pressure ulcers. Therefore, a new PDSA cycle was set to ensure the nurses are competent in this area.
Benefits for staff and patients
It may be difficult to start the QAPI project and at times the process may be stressful, but keep in mind that a successful pressure ulcer QAPI project can improve not only the quality of life and care of your patients but also morale and team building for your staff. n
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has beenspecializing in wound prevention and management since 1990.