At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
In most cases, amputation (removal of an extremity, digit, or other body part) is a surgical intervention performed to remove tissue affected by a disease and, in some cases, to provide pain relief. Fecal and urinary diversion surgeries also are considered amputations. Amputations and fecal or urinary diversions (ostomies) require extensive rehabilitation and adaptation to a new way of life, with physiologic and psychological impacts. Although diversions and ostomies usually are less visible to others than other types of amputations, they call for similar patient education, rehabilitatio n, and lifelong counseling.
The primary goal of therapy for ostomates and amputees is to resume their presurgical lifestyle to the greatest extent possible and to adapt to their new circumstances. Preoperative assessment and training interventions have proven valuable. Having a clear understanding of the surgical intervention helps reduce postoperative anxiety and depression, which can pose roadblocks to patients’ adaptation or response to their new situation. Successful interventions should be done by healthcare professionals who are trained in caring for ostomates and amputees.
Ostomates and amputees experience similar psychosocial challenges, body-
image problems, and sexuality concerns. This article focuses on these three issues. For a summary of other issues these patients may experience, see Other problems amputees and ostomates may face by clicking the PDF icon above.
Psychosocial challenges
Ostomates and amputees may experience depression, anxiety, fear, and many other concerns related to the surgical procedure—concerns that center on whether they’ll be able to resume their presurgical lifestyle. Many worry about social isolation and loss of income. Some fear both the primary disease process and the lifestyle changes induced by surgery. Anxiety may impede their social interactions and lead to significant psychological problems. Appropriate and effective counseling and therapy must be planned and provided. (But be aware that untrained or inexperienced healthcare professionals may not be able to provide the guidance the patient needs to feel comfortable; some may be unable even to offer information about available support systems.)
These patients also may find themselves socially isolated, in part due to loss of employment or the socioeconomic consequences of a decreased income. Some experience fear and worry when anticipating lifestyle changes caused by loss in or change of function, adaptation to the prosthesis, and treatment costs.
Maintaining social contact after surgery is extremely important to recovery and adaptation to the amputation or ostomy. The United Ostomy Associations of America and the Amputee Coalition encourage patients to maintain social involvement. Both groups suggest patients discuss their feelings, thoughts, and fears with a trusted family member, friend, or partner. Both organizations sponsor and encourage support-group involvement. In some cases, emotional support from other amputees or ostomates with a similar experience may be appropriate; some patients may be more comfortable sharing thoughts and asking questions in a group of people with similar experiences. Resuming presurgical social events and activities can enhance patients’ adaptation to a new way of life.
Ostomates and amputees have to cope not only with changes in physical appearance but with how their body functions and how they feel and perceive their body. They’re keenly aware of their changed appearance and are concerned about others’ perceptions of them. They may feel anxious and depressed related to body image; the degree of anxiety and depression may relate directly to their presurgical body image and activities. Many become anxious and fearful as they adapt to the prosthesis. (See Stages of grief by clicking the PDF icon above.)
Compared to amputees, ostomates may have more concerns about body image with sexual partners, because the stoma is, in a sense, a hidden amputation. In most cases, the stoma and pouch can be obscured visually from others. The amputee, on the other hand, has fewer options for hiding the missing body part.
To help patients cope with body-image problems, care providers must offer education, therapy, and counseling to help the patient accept and successfully adapt to the body-image change. The first step in this process may simply be to have the patient look at the stoma or stump, progressing to participation in prosthesis care.
Sexuality concerns
Many ostomates and amputees have difficulty resuming sexual activity after surgery. Although the stoma usually remains hidden from others, it’s observable to the ostomate and sex partner. Most patients require an adjustment period before they feel comfortable with a sex partner. They may fear that:
• the partner will reject them or no longer find them attractive
• they will experience loss of function and sensation
• they will experience pain or injury of the stoma.
They also may feel embarrassed, causing them to avoid sex. However, counselors can help couples discuss these concerns and resume a satisfactory sexual relationship. Ostomates and amputees and their partners may need counseling to resume a satisfactory sexual relationship. If they continue to have adjustment difficulties, referral to a trained sex counselor or psychologist may be indicated. Several studies show that appropriate counseling can help prevent complications and allow amputees and ostomates to continue to express their affection physically. (See Talking to patients about sexual problems by clicking the PDF icon above.)
Resuming sexual activity may be easier if the ostomate or amputee had a sex partner before surgery. However, males who experience postsurgical erectile dysfunction are less likely than other males to resume sexual activity. Counseling encourages postsurgical patients to focus more on the pleasurable feelings they and their partners feel, rather than on sexual performance. Body-image problems and inadequate sexual adjustment go hand in hand. (See Helping ostomates resume sex by clicking the PDF icon above.)
Team approach to patient education and counseling
In many parts of the country, a designated healthcare team manages amputees’ care and rehabilitation. But until recently, nurses were the only professionals certified to participate in ostomates’ care and rehabilitation. In fact, ostomates may represent a significant underserved population. A 2012 study found many ostomy patients didn’t receive consistent training and counseling from ostomy certified nurses. Only 13% of respondents reported they had regular visits with an ostomy certified nurse; 32% said they’d never received care from an ostomy nurse. Just over half (56%) indicated they saw an ostomy nurse when they thought it was necessary. The study also reported that 57% hadn’t seen an ostomy certified nurse in more than 1 year.
A team with specialized training to address ostomates’ physical and psychosocial needs might be able to provide the specialized care these patients need. The primary medical caregiver or general practitioner would serve as team leader and make appropriate referrals. The team should include a surgeon, ostomy- and amputee-trained nurses, a prosthetist or other healthcare provider trained in selection and fitting of prosthetic equipment and devices that affect function, a physical therapist, an occupational therapist, a social worker, a vocational counselor, a psychologist, caregiver or family members, support groups, and (last but not least) the patient.
The team approach might reduce hospital stays and promote patients’ return to their home environment. It also might encourage independence and enhance the success of long-term adaptation.
Focus on the future
Healthcare providers should encourage ostomates and amputees to focus on the future, not the past. Feeling comfortable with the prosthesis—the amputee’s artificial limb or the ostomate’s pouching system—is essential to adapting to a “new normal” way of life. Maintaining social relationships is important to adaptation as well. Mastering basic skills and adapting to changes in body function help improve the patient’s quality of life. Follow-up visits, phone contact, and access to a team of well-trained healthcare providers for patient education, rehabilitation, and long-term management are crucial to these patients’ successful adaptation and quality of life.
Selected references
Bhuvaneswar CG, Epstein LA, Stern TA. Reactions to amputation: recognition and treatment. Prim Care Companion J Clin Psychiatry. 2007;9(4):303-8.
Davidson T, Laberge M. Amputation. Gale Encyclopedia of Surgery: A Guide for Patients and Caregivers. 2004. www.encyclopedia.com/doc/1G2-3406200023.html. Accessed December 20, 2012.
Erwin-Toth P, Thompson SJ, Davis JS. Factors impacting the quality of life of people with an ostomy in North America: results from the Dialogue Study. J Wound Ostomy Continence Nurs. 2012;39(4):417-22.
Maguire P, Parkes CM. Surgery and loss of body parts. BMJ. 1998;316(7137):1086-8.
Pittman J, Kozell K, Gray M. Should WOC nurses measure health-related quality of life in patients undergoing intestinal ostomy surgery? J Wound Ostomy Continence Nurs. 2009;36(3):254- 65.
Pittman J. Characteristics of the patient with an ostomy. J Wound Ostomy Continence Nurs. 2011;38(3):271-9.
Racy JC. Psychological adaptation to amputation. In Bowker JH, Michael JW, ed. Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2nd ed. Rosemont, IL: American Academy of Orthopedic Surgeons; 1998.
Tunn PU, Pomraenke D, Goerling U, Hohenberger P. Functional outcome after endoprosthetic limb-salvage therapy of primary bone tumours—a comparative analysis using the MSTS score, the TESS and the RNL index. Int Orthop. 2008;32(5):619-25.
Turnbull G. Intimacy After Ostomy Surgery Guide. United Ostomy Associations of America, Inc. Revised 2009. www.ostomy.org. Accessed December 20, 2012.
Turnbull G. Sexuality after ostomy surgery. Ostomy Wound Manage. 2006;52(3):14,16.
A hot flush of embarrassment creates a bead of sweat on my forehead. “I’ve got to get this measurement,” I plead to myself. One glance at the clock tells me this bedside ankle-brachial index (ABI) procedure has already taken more than 30 minutes. My stomach sinks as I realize I’ll have to abandon the test as inconclusive. (more…)
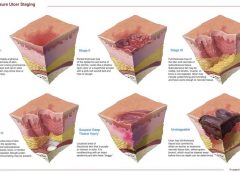
NPUAP releases new position statement on exposed cartilage as Stage IV ulcer
The National Pressure Ulcer Advisory Panel (NPUAP) has released a new position statement, “Pressure ulcers with exposed cartilage are Stage IV pressure ulcers,” which states that pressure ulcers with exposed cartilage should be classified as Stage IV.
NPUAP notes that although the presence of “visible or palpable cartilage at the base of a pressure ulcer” wasn’t included in Stage IV terminology, cartilage “serves the same anatomical function as bone,” so it fits into the current Stage IV definition, “Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often including undermining and tunneling.”
Medicare expenditures for diabetic foot care varies significantly by region
Medicare spending on patients with diabetes who have foot ulcers and lower extremity amputations varies significantly by region, according to a study in Journal of Diabetes and Its Complications, but more spending doesn’t significantly reduce 1-year mortality.
“Geographic variation in Medicare spending and mortality for diabetic patients with foot ulcers and amputations” examined data from 682,887 patients with foot ulcers and 151,752 patients with lower extremity amputations.
Macrovascular complications in patients with foot ulcers were associated with higher spending, and these complications in patients with amputations were more common in regions with higher mortality rates.
Rates of hospital admission were associated with higher spending and increased mortality rates for patients with foot ulcers and amputations.
“Geographic variation in Medicare spending and mortality rates for diabetic patients with foot ulcers and amputations is associated with regional differences in the utilization of inpatient services and the prevalence of macrovascular complications,” the study concludes.
Patients who develop pressure ulcers in hospital more likely to die
Medicare patients who develop pressure ulcers in the hospital are more likely to die during the hospital stay, have longer lengths of stay, and to be readmitted within 30 days after discharge, according to a study of 51,842 patients in the Journal of the American Geriatrics Society.
“Hospital-acquired pressure ulcers: results from the National Medicare Patient Safety Monitoring System Study” found that 4.5% of patients developed at least one new pressure ulcer during their hospitalization. Length of stay averaged 4.8 days for patients who didn’t develop a pressure ulcer, compared to 11.2 days for those with a new pressure ulcer.
Patients with diabetic foot ulcers may have higher risk of death
Patients with diabetes who have foot ulcers have a higher risk of cardiovascular disease and mortality, according to a meta-analysis in Diabetologia.
“The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis” notes that the more frequent occurrence of cardiovascular disease only partly explains the increased mortality rate. Other explanations may include the more advanced stage of diabetes associated with those who had foot ulcers.
A Drugs.com article about the study reported that “analysis of data from more than 17,000 diabetes patients in eight studies found that the more than 3,000 patients with a history of foot ulcers had an extra 58 deaths per 1,000 people each year than those without foot ulcers.”
The study authors emphasize the importance of screening patients with diabetes for foot ulcers so intervention can begin early, as well as lowering cardiovascular risk factors.
Access patient information on foot care from the American Diabetes Association.
Nurse’s innovation for ostomy patients could improve quality of life
An oncology nurse in Australia has developed StomaLife, an alternative to ostomy bags.
StomaLife is a ceramic appliance that eliminates the need for an ostomy bag. According to the StomaLife website, the appliance uses a magnetic implant technology that provides a “pushing force” from within the body outward in order to keep the site intact, while a second part is placed on the stoma site. A cotton gauze pad is used between the skin and the appliance to keep the site separated and to provide air circulation to the surrounding skin.
“The benefits of StomaLife to ostomy patients are continence all day, reduced skin irritation and infection, odour and sound control, leak prevention, waste material flow control and on-demand gas release,” says Saied Sabeti.
StomaLife still needs to be tested and is not yet being produced.
New laser-activated bio-adhesive polymer aims to replace sutures
The Journal of Visualized Experiments, a peer-reviewed video journal, has published “A chitosan based, laser activated thin film surgical adhesive, ‘SurgiLux’: preparation and demonstration.”
SurgiLux is a laser-activated, bio-adhesive polymer that is chitosan-based. Chitosan is a polymer derived from chitin, which is found in fungal cell walls or in exoskeletons of crustaceans and insects. This molecular component allows SurgiLux to form low-energy bonds between the polymer and the desired tissue when it absorbs light.
The technology may be able to replace traditional sutures in the clinical setting. SurgiLux polymer can achieve a uniform seal when activated by a laser and has antimicrobial properties, which help prevent a wound from becoming infected. It also maintains a barrier between the tissue and its surroundings.
SurgiLux has been tested both in vitro and in vivo on a variety of tissues, including nerve, intestine, dura mater, and cornea.
Palliative care raises patient satisfaction and reduces costs
Kaiser Permanente’s home-based palliative care program increased patient satisfaction and decreased emergency department visits, inpatient admissions, and costs, according to an innovation profile in the Agency for Healthcare Research and Quality’s Innovations Exchange.
“In-home palliative care allows more patients to die at home, leading to higher satisfaction and lower acute care utilization and costs” notes that the program uses an interdisciplinary team of providers to manage symptoms and pain, provide emotional and spiritual support, and educate patients and family members on an ongoing basis about changes in the patient’s condition.
Other components of the program include a 24-hour nurse call center, biweekly team meetings, and bereavement services to the family after the patient dies.
More research needed to determine efficacy of maggot debridement therapy
“The efficacy of maggot debridement therapy (MDT)—a review of comparative clinical trials” concludes that “poor quality of the data used for evaluating the efficacy of MDT highlights the need for more and better designed investigations.”
The authors of the article in International Wound Journal reviewed three randomized clinical trials and five nonrandomized clinical trials evaluating the efficacy of sterile Lucilia sericata applied on ulcers.
The studies found that MDT was “significantly more effective than hydrogel or a mixture of conventional therapy modalities, including hydrocolloid, hydrogel and saline moistened gauze,” but the designs of the study were “suboptimal.”
Use tool to select correct antimicrobial dressing
“Ensuring that the correct antimicrobial dressing is selected,” in Wounds International, emphasizes that dressing selection should be based on assessment of the microbial burden in the wound, the wound type, and the location and condition of the wound.
The article includes a checklist that may be helpful for deciding on the level of bacterial burden in a wound. The checklist is used to determine four levels of risk—colonized: at risk; localized infection; spreading infection; and systemic infection. Each level has a corresponding definition.
A table of antimicrobial dressings reviews the antimicrobial agent and dressing form, and the article ends with a case study.
Editor’s note: Part 1 of this series, published in the September-October issue, discussed lymphedema pathology and diagnosis. This article, Part 2, covers treatment.
Traditional treatment approaches
Traditionally, lymphedema treatment has been approached without a clear understanding of the underlying structure and function of lymphatic tissues. Ineffective traditional treatments include elevation, elastic garments, pneumatic pumps, surgery, diuretics, and benzopyrones (such as warfarin). Because many traditional treatments are still overused and some may be appropriate for limited use, it’s important for clinicians to understand these approaches.
Elevation
As a sole therapy for lymphedema, elevation of the affected part provides only short-lived results. Ever-increasing macromolecular wastes retain water against the effects of gravity. Increased interstitial colloid osmotic pressure must be addressed by interventions targeted at improving lymphatic function—not just a position change. Otherwise, lymphedema will progress. Furthermore, elevation alone is impractical, promotes deconditioning, and alters lifestyle for prolonged periods.
Elastic garments
Elastic garments prove inadequate because they attempt to treat lymphedema with compression alone. Medically correct garments are engineered with thoughtful attention to high-quality textiles and offer gradient support, which promotes proximal flow. However, without precise tissue stimulation leading to improved lymphangioactivity (lymph-vessel pulsation), macromolecular wastes can’t be removed.
Interstitial pressure increases caused by compression garments impede further fluid accumulation. When these garments are removed, the spontaneous girth increase causes an imprecise fit, and the garment rapidly leads to a countertherapeutic effect. Furthermore, compression garments don’t combat the osmotic forces generated by ever-increasing interstitial wastes. Except in patients diagnosed with stage 0 or stage 1 lymphedema, disease progression involving metaplasia ensues. Although elastic compression garments are a cornerstone of long-term management, they shouldn’t be used as a stand-alone treatment.
Pneumatic compression pump
Formerly, the pneumatic compression pump (PCP) was considered the standard of care for lymphedema. However, when inflated, the pump doesn’t increase the frequency of lymph-vessel contraction or enhance lymph capillary absorption. What’s more, accelerated fibrosis development and rapid tissue refilling occur when a PCP is removed. Also, PCP use disregards the ipsilateral territory of the excised regional nodes, effectively dumping fluid from the leg into the trunk. A PCP is appropriate only when nothing else is available, as it may worsen the patient’s condition.
Surgery
Surgical approaches to treating lymphedema involve either excisional (debulking) or microsurgical techniques. The most extensive surgical technique, the radical Charles procedure, completely debulks all involved tissue down to the muscle fascia. Split-thickness grafts are then harvested from excised skin and donor sites, and applied to the fascia to achieve so-called limb reduction.
Most debulking procedures have been applied to lower-extremity lymphedema and offer poor cosmetic results. Less radical surgeries favor long incisions, preserving the skin but excising subcutaneous edematous portions to reduce girth. Although less cosmetically alarming, these procedures effectively amputate the subcutaneous space where lymph vessels reside. Other surgical approaches are beyond the scope of this article.
Generally, surgery isn’t a good approach for any patient, as it’s linked to significant morbidity, such as skin necrosis, infection, and sensory changes. In the future, less invasive procedures may be available that yield significant improvement without these adverse effects.
Diuretics
Although diuretics are prescribed appropriately to address water-rich edemas of venous origin, they disregard the fact that lymphedema is a protein-rich edema. Long-term, high-dose diuretic therapy leads to treatment-resistant limbs, similar to those that have received intensive pneumatic compression.
Benzopyrones
Benzopyrones such as warfarin decrease swelling by combating protein accumulation in fluid. Such drugs have undergone clinical trials abroad. Their mechanism is to promote macrophage migration into interstitial fluid, as well as subsequent proteolysis. Due to significant risk of liver damage or failure, benzopyrones haven’t been approved for treating lymphedema.
Complete decongestive therapy: The current treatment approach
Currently, the gold standard for lymphedema treatment is complete decongestive therapy (CDT). Michael Foeldi and Etelka Foeldi, who originated this method, discovered a unique symbiotic relationship among five distinct modalities that addresses the challenges of lymphedema treatment. In 1989, CDT was brought to the United States by Robert Lerner and has become the mainstay of lymphedema treatment here.
CDT is a two-phase approach involving an intensive clinical effort followed by a semi-intensive home-care program geared toward autonomous management, stabilization, and continual improvement. It involves manual lymph drainage (MLD), compression bandaging, exercise, skin and nail hygiene, and self-care education. (See Phases of complete decongestive therapy by clicking the PDF icon above.)
Manual lymph drainage
A type of soft-tissue mobilization, MLD provides skin traction, stimulating superficial lymph vessels and nodes. Lymph capillaries contain large inter-endothelial inlets called swinging tips, akin to overlapping shingles. Each overlapping cell is tethered to the interstitial matrix by anchoring filaments, so that fluid increases cause immediate distention and lymph inflow. Manual skin traction using MLD promotes greater lymph fluid uptake by stretching these filamentous structures, opening the swinging tips.
MLD also provides extrinsic stimulation of the lymphangion (the segment of a lymph vessel between a distal and proximal valve), drawing fluid into the system at the capillary level and promoting flow at the vessel level toward regional lymph nodes. Usually, these segments contract and relax in a rhythmic fashion six times per minute. MLD triples this output to 18 or 20 times per minute, greatly enhancing systemic transport.
MLD requires intensive daily treatment sessions to strengthen collateral flow as a pathway to circumventing surgical or developmental lymphatic disruption. Treatment strategies further recruit more deeply situated lymphatics such as the thoracic duct, as well as lumbar trunks that empty at the juncture of the internal jugular and subclavian veins to improve global uptake. MLD thus stimulates deeper vessel angioactivity to help drain the superficial vessels that drain toward them.
Compression bandaging
Compression bandaging provides tissue support after MLD to prevent reflux, slow new fluid formation, and mechanically soften fibrotic areas. Bandaging techniques provide a high working pressure to harness the muscle and joint pumps as a propellant for lymph while resisting retrograde flow created by gravity and centrifugal forces during movement. Pure cotton materials coupled with specialized padding create a soft, castlike environment, which confines swollen tissues without constriction. By relying on high working pressure and low resting pressures to decrease limb swelling, this strategy achieves greater control over intensity (level of compression/pressure exerted), with little to no soft-tissue injury or discomfort.
The patient wears this bulky inelastic complex after each MLD treatment until the next day’s session to ensure limb-volume reduction in a stable, linear fashion. Once a plateau is reached, tissue stabilization and self-care education are the goals of additional sessions.
Exercise
Exercise always must be done with adequate support to counteract fluid formation. During the intensive CDT phase, limbs are bandaged to provide complete around-the-clock containment. Gentle exercises encourage blood flow into the muscle; during muscle contraction, this creates a favorable internal pressure that effectively squeezes the subcutaneous space between the bandage wall and muscle. Because every bandage strives to provide a gradient of support, fluid tends to drain proximally to the bandage—in most cases, to the trunk.
Skin and nail hygiene
Without intact, well-hydrated skin, cellulitic infections occur in many lymphedema patients whose immune response has been diminished by regional lymphadenectomy or inherited deficiencies. To prevent infection caused by avoidable external events, patients receive clear guidelines to reinforce appropriate behavior. As most cellulitis results from resident skin pathogens (streptococci and staphylococci), maintaining a low skin pH helps control colonization. Ways to avoid recurrent infections include maintaining an acid mantle on the skin using low-pH-formulated lotions and avoiding injury from daily tasks that may scratch, puncture, burn, or abrade the skin. Patients should receive lists of self-care precautions at the time of treatment.
Self-care education
Because lymphedema is a chronic condition, patients must receive self-care education for daily management to avoid lymphedema destabilization, which can lead to tissue saturation and subsequent skin changes. Therapists must provide patients with appropriate self-care tools and knowledge to maintain adequate treatment results. Teaching topics include how to apply and remove compression garments and bandages and how to exercise safely, preserve skin integrity, monitor for infection, and respond appropriately to infection and significant changes in limb mobility.
An underrecognized and mistreated problem
Lymphedema remains an underrecognized and mistreated condition, even though CDT yields safe, reliable results. Early detection, accurate staging, proper diagnosis, and appropriate treatment can slow the inevitable progression of lymphedema. Wound care specialists should adapt wound therapy to address not just the wound but the edematous environment responsible for delayed wound resolution.
Selected references
Al-Niaimi F, Cox N. Cellulitis and lymphedema: a vicious cycle. J Lymphoedema. 2009;4:38-42.
Browse N, Burnand KG, Mortimer PS. Diseases of the Lymphatics. London: Hodder Arnold; 2003.
Casley-Smith JR, Casley-Smith JR. Modern Treatment for Lymphoedema. 5th ed. The Lymphoedema Association of Australia; 1997.
Cooper R, White R. Cutaneous infections in lymphoedema. J Lymphoedema. 2009:4:44-8.
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema. Consensus Document of the International Society of Lymphology. Lymphology. 2009 Jun;42(2):51-60.
Leduc A, Bastin R, Bourgeois P. Lymphatic reabsorption of proteins and pressotherapies. Progress in Lymphology XI. 1988:591-2.
National Lymphedema Network Medical Advisory Committee. Position Statement: Lymphedema Risk Reduction Practices. Revised May 2012. http://www.lymphnet.org/pdfDocs/nlnriskreduction.pdf. Accessed September 5, 2012.
Pappas CJ, O’Donnell TF Jr. Long-term results of compression treatment for lymphedema. J Vasc Surg. 1992 Oct;16(4):555-62.
Whittlinger H. Textbook of Dr. Vodder’s Manual Lymphatic Drainage. Vol 1. 7th ed. New York, NY: Thieme; 2003.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Staphylococcus aureus is one of the most feared human pathogens, causing a wide range of infections. Most wound care professionals can expect to frequently encounter patients with S. aureus infections. Soft-tissue infections caused by S. aureus include impetigo, cellulitis, and cutaneous abscesses, as well as such life-threatening processes as necrotizing fasciitis and pyomyositis (a hematogenous intramuscular abscess). Serious non-soft-tissue infections include septic arthritis, osteomyelitis, pneumonia, endocarditis, and sepsis.
Why is S. aureus such a nasty bug?
S. aureus produces various cellular and extracellular factors involved in the pathogenesis of infection. S. aureus protein A, an important surface protein, helps the organism resist phagocytosis. Also, S. aureus produces several cytotoxins and enzymes that contribute to infection spread and severity. In addition, some strains produce toxins (including toxic shock syndrome toxin-1) that function as superantigens—molecules that nonspecifically trigger release of large amounts of cytokines, leading to a sepsislike condition. Taken together, such factors combine to make S. aureus a dangerous pathogen.
MRSA emergence
When penicillin was introduced in the 1940s, virtually all S. aureus isolates were sensitive to that drug. But soon thereafter, S. aureus strains that produced a β-lactamase enzyme capable of inactivating penicillin became widespread. During the 1950s, outbreaks of penicillin-resistant S. aureus occurred in many U.S. hospitals. Introduction of penicillinase-resistant antibiotics, such as methicillin and oxacillin, temporarily restored the ability to treat all strains of this pathogen using penicillin antibiotics. The first strain of methicillin-resistant S. aureus (MRSA) was described in 1961 shortly after introduction of penicillinase-resistant antibiotics.
The mechanism of methicillin resistance involves a mutation in one of the bacterial cell-wall proteins to which penicillins must bind to kill the bacterium. This mutation renders the organism resistant to all penicillins and penems and almost all cephalosporins.
MRSA incidence has increased steadily to the point where it currently constitutes up to 60% of S. aureus isolates in many U.S. hospitals. These organisms commonly carry genetic material that makes them resistant to various non-β lactam antibiotics as well, leading some to suggest that the term MRSA should stand for multiply resistant S. aureus. S. aureus has continued to mutate in the face of persistent antibiotic pressure. Vancomycin-intermediate S. aureus (VISA) was described in 1997; vancomycin-resistant S. aureus (VRSA), in 2003. Fortunately, these two strains remain rare and haven’t become established pathogens. (See Strains of antibiotic-resistantS. aureus by clicking the PDF icon above.)
Healthcare- versus community-acquired MRSA
Although MRSA initially arose and spread within healthcare settings (chiefly acute-care hospitals), a community-based variant was described in 1998. Called community-
acquired MRSA (CA-MRSA), this variant differs from healthcare-associated MRSA (HCA-MRSA) in more ways than the acquisition site. CA-MRSA occurs predominately in otherwise healthy children and young adults.
It most commonly presents as recurrent cutaneous abscesses, although life-threatening infections (such as necrotizing fasciitis and pneumonia) also have occurred. The propensity to cause cutaneous abscesses isn’t fully understood but may relate partly to production of the Panton-Valentine toxin by many CA-MRSA isolates.
In contrast, HCA-MRSA afflicts mainly older patients, particularly those with chronic illnesses, including chronic wounds. It typically causes wound infections, urinary tract infections, pneumonia, and bacteremia.
Besides these epidemiologic and clinical differences, many CA-MRSA isolates derive from a single clone, known as clone USA 300, whereas HCA-MRSA is composed of multiple non-USA 300 clones. Finally, many CA-MRSA isolates are sensitive to non-β
lactam antibiotics, whereas most HCA-MRSA isolates resist multiple antibiotics. More recently, the distinction between CA-MRSA and HCA-MRSA has been blurred as evidence emerges that CA-MRSA now is being transmitted in healthcare settings as well as in the community.
S. aureus carrier state
Staphylococci are frequent colonizers of humans. Common colonization sites include the skin, anterior nares, axillae, and inguinal regions. Individuals can be colonized continuously or transiently, with nasal carriage rates varying from 20% to 40%. Most S. aureus infections result from the strain carried by the infected patient.
Three patterns of S. aureus carriage exist in humans:
• 20% of individuals are continuously colonized.
• 30% of individuals are intermittently colonized.
• 50% of individuals are never colonized.
The highest carriage rates occur in patients receiving frequent injections (such as insulin-dependent diabetics, hemodialysis patients, and I.V. drug users) and those with chronic skin conditions (for instance, psoriasis or eczema). In the general population, MRSA carriage rates have increased to 1% or 2%, with clinical consequences hinging on the colonizing strain (CA-MRSA versus HCA-MRSA) and host characteristics. The most consistent carriage site is the anterior nares, but many other sites may carry this pathogen, including the axillae, inguinal regions, and perirectal area.
MRSA treatment
Therapy for MRSA infection depends on the infection location and antibiotic sensitivity of the infecting strain.
• Cutaneous abscesses are treated by incision and drainage; antibiotics play a secondary role to adequate drainage.
• Therapy for necrotizing fasciitis caused by MRSA involves aggressive debridement with removal of all necrotic tissue, plus adequate antibiotic therapy. Typically, patients require serial debridement followed by subsequent careful wound care, often with eventual skin grafting.
• Pyomyositis treatment entails drainage of the muscle abscess (which sometimes can be done with percutaneous tube placement instead of open drainage), plus appropriate antibiotic therapy.
Vancomycin has been the mainstay of I.V. therapy for MRSA for decades, but some clinicians are concerned that its effectiveness may be declining due to slowly increasing minimum inhibitory concentrations (the minimum concentration of an
antibiotic needed to inhibit pathogen growth). Other parenteral options have emerged in the last few years. (See I.V. drugs used to treat MRSA by clicking the PDF icon above.) Several oral antibiotics also are available for MRSA treatment. (See Oral agents used to treat MRSA by clicking the PDF icon above.)
Knowing the antibiotic sensitivity pattern of the infecting MRSA strain is crucial to ensuring that the patient receives an appropriate antibiotic. Treatment duration for soft-
tissue infections usually ranges from 7 to 14 days, but bacteremia and bone or joint infections call for more prolonged therapy.
Efforts to eradicate MRSA carriage
Because the carrier state increases the risk of subsequent S. aureus infection, efforts have been made to eradicate carriage. Unfortunately, this has proven to be difficult. A commonly used regimen involves 5 days of twice-daily mupirocin nasal ointment with either chlorhexidine gluconate showers or immersion up to the neck in a dilute bleach solution. However, success in eliminating carriage is limited, although the bleach bath seems to improve eradication rates better than other modalities.
Controlling MRSA in hospitals
How best to control MRSA spread within hospitals is controversial. Some experts advocate an aggressive, “search and destroy” approach involving screening all patients for nasal carriage on admission and initiating contact precautions with subsequent decolonization efforts. Others focus on improving the overall level of hand hygiene and other general infection-control measures, arguing that nasal screening misses at least 20% of MRSA-colonized patients and thus gives an unwarranted sense of security.
Many hospitals use a mixed approach, screening patients suspected to be at high risk for MRSA carriage (such as those admitted from extended-care facilities or to the intensive care unit), while simultaneously trying to improve hand hygiene and general infection-control measures. Recent data suggest MRSA colonization and infection rates have stopped increasing and are beginning to decline.
MRSA is one of the most problematic pathogens encountered on a regular basis, and among the most dangerous pathogens we face. While some MRSA infections are relatively mild, many are serious or life-threatening. Severe soft-tissue infections, such as necrotizing fasciitis and pyomyositis, require surgical debridement or drainage, appropriate antibiotic therapy, and assistance from a wound-care professional to achieve optimal outcomes. n
Selected references
Calfee DP. The epidemiology, treatment and prevention of transmission of methicillin-resistant Staphylococcus aureus. J Infus Nurs. 2011 Nov-Dec;34(6):359-64.
DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010 May 1;375(9725): 1557-68.
Ippolito G, Leone S, Lauria FN, et al. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010 Oct;14 Suppl 4:S7-11.
Landrum ML, Neumann C, Cook C, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010. JAMA. July 4;308:50-9.
Lee AS, Huttner B, Harbarth S. Control of methicillin-resistant Staphylococcus aureus. Infect Dis Clin North Am. 2011 Mar;25(1):155-79.
Moellering RC Jr. MRSA: the first half century. J Antimicrob Chemother. 2012 Jan;67(1):4-11.
Otter JA, French GL. Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection. J Hosp Infect. 2011 Nov:79(3):189-93.
Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant pneumococci, and vancomycin-resistant enterococci. Mayo Clin Proc. 2011 Dec;86(12):1230-43.
Simor AE. Staphylococcal decolonization: an effective strategy for prevention of infection? Lancet Infect Dis. 2011 Dec;11(12):952-62.
Joseph G. Garner is director of the infectious disease division and hospital epidemiologist at the Hospital of Central Connecticut and a professor of medicine at the University of Connecticut.
Lymphedema is characterized by regional immune dysfunction, distorted limb contours, and such skin changes as papillomas, hyperkeratosis, and increased girth. The condition may involve the limbs, face, neck, trunk, and external genitals; its effects may include psychological distress. For optimal patient management, clinicians must understand what causes lymphedema and how it’s diagnosed and treated.
This two-part series provides an overview of lymphedema. Part 1 covers etiology, pathology, and diagnosis. Part 2, which will appear in the November-
December issue, will focus on treatment.
Causes of lymphedema
Lymphedema occurs when protein-rich fluid accumulates in the interstitium due to impaired lymphatic function. Proteins, other macromolecular wastes, and water constitute lymphatic loads. These wastes rely on specially structured absorptive and transport structures in peripheral regions for their return to central circulation.
When lymph stasis prevails, inflammatory processes and lymphostatic fibrosis trigger tissue-density changes, further entrapping superficial vessels and accelerating mechanical insufficiency. (See Physiologic changes caused by lymphatic disruption by clicking the PDF icon above.)
Classifying lymphedema
Lymphedema can be primary or secondary. Primary lymphedema either is congenital (present at birth) or arises around puberty. In the vast majority of cases, it is associated with structural changes in the lymphatic system and isn’t associated with another disease or condition. Most structural changes (87%) manifest before age 35 and cause hypoplasia of vessels and nodes. Syndromes involving hyperplasia, node fibrosis, or aplasia also may occur, although they’re much less common. Dysplasia (either hypoplasia, hyperplasia, or aplasia) predisposes drainage regions to inadequate lymph collection, resulting in edema and secondary tissue changes, such as chronic inflammation and reactive fibrosis. Genetic variability in lymphatic constitution may explain why seemingly similar patients receiving the same surgical protocol have different lymphedema risks over time. Secondary lymphedema stems from a significant insult to lymphatic tissues, as from lymphadenectomy, radiation therapy, trauma, infection, or cancer. It commonly results from direct trauma to regional nodes or vessel structures. Slow degradation of lymphatic function also occurs when adjacent tissues (such as superficial and deep veins) become diseased, when cellulitis occurs, or when accumulations
of adipose or radiation fibrosis mechanical-ly disrupt drainage of skin lymphatics.
Lymphedema stages
Lymphedema progresses in stages, which involve secondary connective-tissue disease combined with disturbed fluid update and transport. These conditions cause a universal and classic clinical picture.
• Stage 0 (latency stage) is marked by reduced transport capacity and functional reserve. The patient has no visible or palpable edema, but has such subjective complaints as heaviness, tightness, and waterlogged sensations.
• In Stage 1 edema (reversible lymphedema), edema decreases with elevation. Pitting edema is present, but fibrosis is absent.
• During Stage 2 (spontaneously irreversible lymphedema), lymphedema doesn’t resolve entirely, although it may fluctuate. Pitting is more pronounced and fibrosis is present.
• Stage 3 (lymphostatic elephantiasis) is marked by dermal hardening, nonpitting edema, papillomas, hyperkeratosis, and in some cases, extreme girth.
Assessment and diagnosis
Diagnosing lymphedema can be challenging because edema may be associated with other diseases and disorders. For a summary of signs and symptoms, see Clinical findings in lymphedema by clicking the PDF icon above.
Discomfort and skin appearance
Lymphedema rarely causes pain because the skin accommodates gradual, insidious fluid accumulation. However, secondary orthopedic discomfort may result from increased weight of the affected limb due to deconditioning or decreased range of motion.
Because lymphedema usually progresses slowly, gravity and centrifugal forces pull fluids toward distal limb areas, causing an entrenched, stubborn pitting edema. Later, further valvular incompetence contributes to worsening distal edema in the fingers, toes, and dorsal regions of the hand and foot. Prominent lower-extremity structures, such as the malleolus, patella, tibia, anterior tibialis tendon, and Achilles tendon, become progressively less distinct. This creates a columnar limb appearance; the swollen limb has the same girth from distal to proximal aspects, unlike the natural cone shape of a normal limb.
Lymphatic failure doesn’t tax the venous system, so skin color remains normal. Blood supply remains patent, helping to prevent secondary ulcers.
Severity
Lymphedema severity correlates directly with such factors as onset of the condition and extent of cancer therapy, if given (number of nodes resected, number of positive nodes, and use of radiotherapy). Lymphedema may worsen with a greater number of infection episodes, weight gain, injury, diuretics, limb disuse, pneumatic compression therapy (when used for pure lymphedema), and ill-fitting compression garments. The single most important contributor to increasing lymphedema severity is lack of patient education, which can result in improper treatment or none at all.
Opportunistic infections
Lymphedema causes regional immune suppression and leads to an increase in opportunistic infections such as cellulitis. As skin integrity suffers, scaling and dryness allow resident skin pathogens (such as streptococci and staphylococci) to gain access through the defective skin barrier into protein-rich interstitial fluid, creating a medium favorable to bacterial colonization. Lymphocyte migration decreases, and dissected or irradiated nodal sites are slow to detect invaders. Furthermore, stagnant lymph promotes further delays in the immune response. Patients with opportunistic infections may exhibit high fever, local erythema, regional hypersensitivity or acute pain, flulike symptoms, and rapidly advancing “map-like” borders in the skin.
Differential diagnosis
Several methods can aid differential diagnosis. Clinical findings. Lymphedema can be diagnosed from patient history, physical examination, palpation, and inspection. Trauma to lymph nodes (each of which governs a distinct body region) decreases the transport capacity of lymph formed in that region, in turn causing local swelling (lymphedema). Trauma to the axillary or inguinal lymph nodes, which exist on both the left and right of the body and in both the upper and lower regions, predisposes these quadrants to swelling. Therefore, if lymph nodes on only one side are damaged, lymphedema occurs only on that side of the body. Using the universal characteristics cited above as a guide, while ruling out cancer recurrence, acute deep vein thrombosis, or plasma protein abnormalities, yields sufficient data to form a diagnosis. Imaging. Lymphography involves subcutaneous injection of a lymph vessel–
specific dye (Patent Blue V), followed by X-ray. Although it provides high-resolution images of lymphatic structures, this technique is invasive, painful, damaging to lymphatics, and potentially lethal—and therefore is no longer recommended.
Lymphangioscintigraphy (LAS) uses interdigital subcutaneous injection of protein-labeled radioisotopes, followed by
imaging at specific intervals to gather information about uptake and transport time. Images are hazy and false-negatives are common, so well-trained radiotherapists familiar with lymphology and lymphedema should administer and interpret the test. Also, experts don’t agree on standard criteria for LAS administration, so measures may not be similarly conclusive. Limb-measuring instruments and methods. Serial measurement of affected limb circumference using a standard garment tape measure is the most widely accessible approach. Intra-rater reliability is comparable to that of currently used tools; however, these methods can’t be used for early detection, for screening, or when various raters are used to assess the same patient. Circumferences are measured at four points and are considered positive if a distance of 2 cm or more separates the involved from uninvolved extremity in comparison. Water displacement techniques for limb-volume calculation, although accurate, are impractical in most clinical settings and rarely used.
Various devices have been used to obtain measurements. For instance, the Perometer® uses optoelectronic volumetry. By scanning the limb with infrared beams circumferentially, the device accurately records girth at 4-mm intervals along the limb length and transmits these measurements to a computer. The Perometer is used mainly in the research setting. Preoperative and postoperative measurements at intervals can detect lymphedema early.
Impedimed XCA® uses bioelectrical
impedance to calculate ratios of intracellular to extracellular fluid. A weak electrical current is passed through affected and unaffected limbs, allowing comparison of results. Impedance is lower in edematous tissue, supporting an accurate diagnosis.
Next step: Treatment
Once a diagnosis is made, the next step is treatment. Part 2 of this series covers lymphedema treatment.
Selected references
Foeldi M. Foeldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. 3rd ed. St. Louis, MO: Mosby; 2012.
Kubik S, Manestar M. Anatomy of the lymph capillaries and precollectors of the skin. In: Bollinger A, Partsch H, Wolfe JHN, eds. The Initial Lymphatics. Stuttgart: Thieme-Verlag; 1985:66-74.
Lee B, Andrade M, Bergan J, et al. Diagnosis and treatment of primary lymphedema. Consensus document of the International Union of Phlebology (IUP)—2009. Int Angiol. 2010 Oct;29(5):454-70.
Lerner R. Chronic lymphedema. In: Prasad H, Olsen ER, Sumpio BE, Chang JB, eds. Textbook of Angiology. Springer; 2000.
Mayrovitz HN. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology. 2009 June;42(2):88-98
Pecking AP, Alberini JL, Wartski M, et al. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): toward a comprehensive staging. Lymphology. 2008 Mar;41(1):1-10.
Stanton AW, Northfield JW, Holroyd, B, et al. Validation of an optoelectronic volumeter (Perometer). Lymphology. 1997 June;30(2):77-97
Weissleder H, Schuchhardt C. Lymphedema: Diagnosis and Therapy. 4th ed. Viavital Verlag GmbH; 2007.
Steve Norton is cofounder of Lymphedema & Wound Care Education and executive director of the Norton School of Lymphatic Therapy in Matawan, New Jersey.
Necrotizing fasciitis (NF) results from an infection that attacks the fascia and subcutaneous tissues. The primary bacterial etiology is group A streptococcus, a facultative anaerobic bacterium. However, other bacteria may contribute. Sometimes called the “flesh-eating” disease because of the potentially devastating effect on the afflicted patient, NF can be monomicrobial or polymicrobial.
The four typical settings for NF are:
surgical bowel or abdominal trauma surgery
pressure ulcer and perianal abscess
injection sites (especially in drug users)
Bartholin abscess or minor vulvovaginal infection.
Because of the rapid course and ravaging nature of acute NF, clinicians must maintain a high index of suspicion if the patient has suggestive signs and symptoms. In 1990, puppeteer Jim Henson (best known for creating the Muppets) died from NF. At that time, little was known about the progression of group A streptococcal infection.
The disease can quickly cause death, so starting immediate treatment is even more crucial than confirming the diagnosis. Once the disease is suspected, antibiotics must be given immediately and the patient must be prepared for surgery at once. NF spreads rapidly, capable of progressing from a small lesion to death in days to weeks. Thus, delayed diagnosis increases the risk of death. Lack of knowledge about the disease and inability to recognize it promptly are the main reasons many victims die. This article can improve your knowledge base.
Overview
NF was discovered in 1871 by Joseph Jones, a Confederate Army surgeon. At that time, it was called hemolytic streptococcal gangrene, nonclostridial gas gangrene, nonclostridial crepitant cellulitis, necrotizing or gangrenous erysipelas, necrotizing cellulitis, bacterial synergistic gangrene, or synergistic necrotizing cellulitis.
NF involves the fascia, muscle compartments, or both. It can affect not only the muscle fascia but the superficial fascia. NF and cellulitis differ in the amount of tissue involved and extent of tissue involvement.
The most common areas of infection are the abdominal wall, perineum, and extremities. When NF affects the perineum and scrotum, it’s called Fournier gangrene, after the French dermatologist and virologist Alfred Jean Fournier.
The most common causes are trauma, surgery, and insect bites. The disease can affect persons of any age. Such comorbidities as diabetes, chronic renal failure, immunosuppressive therapy, hypertension, obesity, and malnutrition increase susceptibility.
Pathophysiology
NF falls into four classifications based on wound microbiology. Type 1, the most common, involves polymicrobial bacteria. Type 2 results from trauma and is associated with comorbidities. Type 3, rare in this country, stems from gram-negative marine bacteria. Type 4 is a fungal infection occurring mostly in immunocompromised persons. (See Comparing types of necrotizing fasciitis by clicking the PDF icon above.)
Disease progression
The four types of NF progress in a similar way. Bacteria secrete pyrogenic exotoxin A, which stimulates cytokines. These cytokines damage the endothelial lining; fluid then leaks into the extravascular space.
M proteins in streptococci and β-hemolytic streptococci exacerbate the immune reaction by inhibiting phagocytosis of polymorphonuclear leukocytes and normal neutrophil chemotaxis. As the immune reaction increases, blood vessels dilate, allowing toxins to leak through vessel walls, which in turn decreases blood flow. As the cascade continues, hypoxic conditions cause facultative aerobic organisms to grow and become anaerobic. These bacteria exacerbate destruction of surrounding cells and lead to release of carbon dioxide, water, hydrogen, nitrogen, hydrogen sulfide, and methane. As the infection continues to progress, toxins spread throughout the bloodstream and the patient becomes septic.
Assessment
Obtain the patient’s medical history and description of the wound. Determine when the changes first appeared and whether the affected area seemed to get worse recently.
In all NF types, patients commonly present with a small, painful area (possibly with entry marks) but no other signs or symptoms. The wound may appear as a bulla, cellulitis, or dermatitis, representing an infection developing in underlying tissues. The skin may have a wooden-hard feel as the infection progresses to the subcutaneous space and causes necrosis. The wound becomes discolored and necrotic; drainage is rare until surgical debridement begins. The patient quickly develops fever, chills, nausea, and vomiting. As NF progresses, bullae become dark purple with darkened edges; the patient grows disoriented and lethargic, and organ failure and respiratory failure
ensue. Without treatment, the patient dies.
Diagnosis
Diagnostic tests usually include magnetic resonance imaging, complete blood count with differential, comprehensive metabolic panel, and cultures. (See Diagnostic findings in necrotizing fasciitis by clicking the PDF icon above.)
Treatment
Immediate surgical debridement and broad-spectrum antibiotics are needed to stop the immune response to infection. Clindamycin, gentamicin, penicillin, or metronidazole may be given alone or in combination until culture results are available. Supportive care includes total parenteral nutrition for nutritional support, I.V. fluids, and oxygen. Limb amputation should be done only as a last resort.
Surgical debridement involves penetrating deep into the fascia and removing all necrotic tissue. After the first debridement, release of “dishwater fluid” may occur.
Administering hyperbaric oxygen therapy (HBOT) after the first debridement increases tissue oxygenation, thus reducing tissue destruction by anaerobic bacteria. During HBOT (usually given as a 90-minute treatment), the patient breathes 100% oxygen in an environment of increasing atmospheric pressure.
HBOT should be given in conjunction with surgical debridement (usually after each debridement) and should continue until necrotic tissue ceases and cell destruction stops. HBOT also promotes collagen synthesis and neoangiogenesis (new blood vessel growth), which boosts blood supply and oxygen to tissues.
Adverse effects of HBOT include ear pain, oxygen toxicity, and seizures. Ear pain can be minimized by swallowing or yawning. If the patient continues to have ear pain, ear tubes may be inserted by an otolaryngologist. During HBOT, air breaks (intervals of breathing room air) are important in controlling oxygen toxicity (the main cause of seizures).
Throughout the HBOT treatment period, wound dressings must be simple. Well-moistened gauze dressings and an abdominal pad provide good support. Once necrotic destruction occurs, dressings depend on wound size and the need to fill cavities. The patient may require a diverting colostomy, depending on wound
location and the amount of uncontrolled diarrhea. Blood glucose levels must be monitored before and after HBOT, as this treatment affects blood glucose.
Supportive care and follow-up treatment
During initial treatment, patients need supportive care and monitoring. Once they’re out of danger, begin teaching them how to prevent NF recurrences. Advise them to control blood glucose levels, keeping the glycated hemoglobin (HbA1c) level to 7% or less. Caution patients to keep needles capped until use and not to reuse needles. Instruct them to clean the skin thoroughly before blood glucose testing or insulin injection, and to use alcohol pads to clean the area afterward.
Before discharge, help arrange the patient’s aftercare, including home health care for wound management and teaching, social services to promote adjustment to lifestyle changes and financial concerns, and physical therapy to help rebuild strength and promote the return to optimal physical health. One helpful patient resource is the National Necrotizing Fasciitis Foundation. The Centers for Disease Control and Prevention section on necrotizing fasciitis includes “Common sense and great wound care are the best ways to prevent a bacterial skin infection.”
The life-threatening nature of NF, scarring caused by the disease, and in some cases the need for limb amputation can alter the patient’s attitude and viewpoint, so be sure to take a holistic approach when dealing with the patient and family. Today, NF has a much better survival rate than 2 decades ago when Jim Henson died. In my practice, I’ve seen four NF cases. Thanks to early identification, good wound care, and HBOT, these patients suffered only minimal damage.
Selected references
Boyer A, Vargas F, Coste F, et al. Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management. Intensive Care Med. 2009;35(5):847-853. doi:10.1007/s00134-008-1373-4.
Cain S. Necrotizing fasciitis: recognition and care. Practice Nurs. 2010;21(6):297-302.
Centers for Disease Control and Prevention. Notes from the field: fatal fungal soft-tissue infections after a tornado—Joplin, Missouri, 2011. MMWR. 2011;60(29):992.
Chamber AC, Leaper DJ. Role of oxygen in wound healing: a review of evidence. J Wound Care. 2011; 20(4):160-164.
Christophoros K, Achilleas K, Vasilia D, et al. Postraumatic zygomycotic necrotizing abdominal wall fasciitis with intraabdominal invasion in a non immunosuppressed patient. Internet J Surg. 2007;11(1). doi:10.5580/17a8.
Ecker K-W, Baars A, Topfer J, Frank J. Necrotizing fasciitis of the perineum and the abdominal wall-surgical approach. Europ J Trauma Emerg Surg. 2008;
34(3):219-228. doi:10.1007/s00068-008-8072-2.
Hunter J, Quarterman C, Waseem M, Wills A. Diagnosis and management of necrotizing fasciitis. Br J Hosp Med. 2011;72(7):391-395.
Magel DC. The nurse’s role in managing necrotizing fasciitis. AORN J. 2008;88(6):977-982.
Phanzu MD, Bafende AE, Imposo BB, Meyers WM, Portaels F. Under treated necrotizing fasciitis masquerading as ulcerated edematous Mycobacterium ulcerans infection (Buruli ulcer). Am J Trop Med Hyg. 2012;82(3):478-481.
Ruth-Sahd LA, Gonzales M. Multiple dimensions of caring for a patient with acute necrotizing fasciitis. Dimens Crit Care Nurs. 2006;25(1):15-21.
Stevens DL, Bisno AL, Chambers HF, et al; Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41(10):1373-1406.
Su YC, Chen HW, Hong YC, Chen CT, et al. Laboratory risk indicator for necrotizing fasciitis score and the outcomes. ANZ J Surg. 2008;78(11):968-972.
Taviloglu K, Yanar H. Necrotizing fasciitis: strategies for diagnosis and management. World J Emerg Surg. 2007;2:19.
Lydia Meyers is a medical reviewer for National Government Services in Castleton, Indiana, and a clinical liaison at CTI Nutrition in Indianapolis. She has 11 years of wound care experience in nursing homes, wound clinics, and home health.
The guideline updates IDSA’s 2004 diabetic foot infections guideline. It focuses on appropriate therapy, including debridement of dead tissue, appropriate antibiotic therapy, removing pressure on the wound, and assessing (and potentially improving) blood flow to the foot. The guideline also provides suggestions regarding when and how long antibiotics should be administered for soft-tissue and bone infections.
When diagnosing a diabetic patient with foot infection, the guideline recommends clinicians evaluate the patient at three levels—the patient as a whole, the affected foot or limb, and the infected wound. The guideline also provides advice on when and how to culture diabetic foot wounds.
Access a podcast on the guideline, which is available in a smartphone format and as a pocket-size quick-reference edition.
Combining bariatric surgery with medical therapy improves glycemic control
In obese patients with uncontrolled type 2 diabetes, bariatric surgery and 12 months of medical therapy significantly improved glycemic control compared to those who received only medical therapy, according to a study in The New England Journal of Medicine. “Bariatric surgery versus intensive medical therapy in obese patients with diabetes” was a randomized, nonblinded, single-center trial that included 150 patients in three groups: medical therapy only, medical therapy and Roux-en-Y gastric bypass, and medical therapy and sleeve gastrectomy.
Although glycemic control improved for all three groups, those who received bariatric surgery had better control. Use of drugs to lower glucose, lipid, and blood-pressure levels decreased significantly after both surgical procedures but increased in patients receiving medical therapy only. No deaths or life-threatening complications occurred.
HHS launches web-based tool for tracking healthcare performance
The U.S. Department of Health and Human Services (HHS) has launched a web-based tool for monitoring the performance of the healthcare system. The Health System Measurement Project gives providers and the public the ability to examine datasets from across the federal government that span specific topic areas, such as access to care, vulnerable populations, prevention, and quality. Users can also view indicators by population characteristics, such as age, sex, income level, insurance coverage, and geography.
PEG tubes may increase risk of new pressure ulcers
According to a study published in Archives of Internal Medicine, percutaneous endoscopic gastrostomy (PEG) tubes may increase the risk of pressure ulcers in nursing home patients with advanced cognitive impairment.
Researchers found that hospitalized patients who receive a PEG tube were 2.27 times more likely to develop a new pressure ulcer and those with a pressure ulcer were less likely to have it heal when they had a PEG tube. “Our findings regarding the risk of developing new stage 2 or higher pressure ulcers suggest that PEG feeding tubes are not beneficial, but in fact they may potentially harm patients,” conclude the researchers in “Feeding tubes and the prevention or healing of pressure ulcers.”
AHRQ provides QI toolkit for hospitals
The Agency for Healthcare Research and Quality (AHRQ) offers a toolkit designed to help hospitals understand AHRQ’s quality indicators (QIs). “AHRQ Quality Indicators™ Toolkit for Hospitals” includes steps for improvement, how to sustain change, and different tools for different audiences. Clinicians can also access audio interviews that provide information on how to use the tools and engage stakeholders and staff in QI efforts, and a recording of a webinar on the toolkit.
Silk fibers may be future resource for bone and tissue repair
Researchers at Tufts University have developed the first all-polymeric bone scaffold material that is fully biodegradable and capable of providing significant mechanical support during repair. The material could improve the way bones and tissues are repaired after an accident or following disease effects.
The new technology uses micron-size silk fibers to reinforce a silk matrix, much as steel rebar reinforces concrete. The study, “High-strength silk protein scaffolds for bone repair,” published in Proceedings of the National Academy of Sciences, found that the scaffold material is significantly less strong than normal bone, but it may play a role as a temporary biodegradable support for the patient’s cells to grow.
International guidelines for silver dressings in wounds released
A meeting of an international group of experts, convened by Wounds International, met in December 2011 to compile the consensus guidelines, which describe the patients who are most likely to benefit from silver dressings and how to use the dressings appropriately.
The guidelines recommend that silver dressings be used “in the context of accepted standard wound care for infected wounds or wounds that are at high risk of infection or reinfection.” Another recommendation is to use silver dressings for 2 weeks, then evaluate the wound, patient, and management approach before deciding whether to continue using the dressing or if a more aggressive intervention such as antibiotics would be better.
Cell therapy may benefit patients with lower extremity CLI
Injections of ixmyelocel-T in patients with lower extremity critical limb ischemia (CLI) who aren’t candidates for revascularization can prolong the time until treatment failure, according to a study in Molecular Therapy. Time to treatment failure was defined as major amputation, all-cause mortality, doubling of total wound surface area from baseline, or de novo gangrene. The double-blind, placebo-controlled RESTORE-CLI trial found that the adverse event rates were similar in the two groups.
New skin patch destroys skin cancer cells
A new skin patch destroyed facial basal cell carcinoma cells in 80% of patients, according to a study reported at the Society of Nuclear Medicine’s 2012 Annual Meeting.
Each of the 10 patients with facial basal cell carcinoma received a custom-made and fully sealed phosphorus-32 skin patch, a radiation spot-treatment in the form of a patch. Each patient was treated for 3 hours on the first day; the patches were reapplied on the fourth and seventh days after the first treatment for another 3 hours each. Three years after treatment, 8 of 10 patients were cancer-free.
The patients had lesions near the eyes, the nose, and forehead—areas more difficult to operate on, especially if skin grafting is needed later.
Small study links lymphedema to obesity
The average body-mass index (BMI) in obese patients with lymphedema was significantly greater than BMIs of obese patients without lymphedema, according to correspondence in The New England Journal of Medicine. The authors conclude, “Our findings suggest that obesity…may be a cause of lower-extremity lymphedema.”
“Lower-Extremity Lymphedema and Elevated Body-Mass Index” included 15 obese patients with bilateral lower-extremity enlargement who were referred to the authors’ center. Of the 15, five were diagnosed with lymphedema by lymphoscintigraphy.
Study finds ultrasound therapy improves venous ulcer healing
In a study of 10 venous ulcers not responding to treatment, the use of noncontact ultrasound significantly reduced the wound area over 4 weeks of treatment.
It has been unclear exactly how ultrasound achieves its positive results. The
authors of “A prospective pilot study of ultrasound therapy effectiveness in refractory venous leg ulcers,” an article published online on February 1 by the International Wound Journal, found that patients treated with ultrasound and compression therapy had reduced inflammatory cytokines and bacterial counts, but the reduction wasn’t statistically significant.
The study found another important benefit for patients-reduced pain.
Serum albumin is not a goodindicator of nutritional status
Traditionally the standard of practice for wound care patients has been to review albumin blood levels as a measure of nutritional status and the effect of nutritional interventions. But as noted in The Role of Nutrition in Pressure Ulcer Prevention and Treatment: National Pressure Ulcer Advisory Panel White Paper, recent studies show that hepatic proteins (albumin, transthyretin, and transferrin) correlate with the severity of an underlying disease, not nutritional status. Moreover, many factors can alter albumin levels even when protein intake is adequate, including infection, acute stress, surgery, cortisone excess, and hydration status.
For these reasons, the National Pressure Ulcer Advisory Panel (NPUAP) and the Academy of Nutrition and Dietetics (previously known as The American Dietetic Association) recommend against using serum proteins as a nutritional assessment tool. Evaluation of lab values is just one part of the nutritional assessment process and should be considered along with other factors such as ensuring that the patient receives what is prescribed; daily food/fluid intake; changes in weight status, diagnosis, and medications; and clinical improvement in the wound.
The mean number of serious comorbid conditions was 1.8.
The most common comorbid conditions were obesity/overweight (71.3%), cardiovascular or peripheral vascular disease (51.3%), and diabetes (46.8%).
Nearly two-thirds (65.8%) of wounds healed, with an average healing time
of 15 weeks.
In half of the wounds that healed, patients received only moist wound care and no advanced therapeutics.
The mean cost for wound healing was $3,927.
The authors of the article, published in March’s Wounds, analyzed 5,240 patients with 7,099 wounds in 59 hospital-based outpatient wound centers in 18 states over 5 years.
LOI index comparable to ABI for assessing PAD in patients with type 2 diabetes
The pilot study “Lanarkshire Oximetry Index as a diagnostic tool for peripheral arterial disease in type 2 diabetes,” published in Angiology, compared the gold standard ankle brachial index (ABI) to the Lanarkshire Oximetry Index (LOI) in 161 patients with type 2 diabetes. Researchers assessed the patients for peripheral artery disease (PAD, defined as ABI < 0.9) using both ABI and LOI.
Using a LOI cut-off value of 0.9., the sensitivity and specificity for PAD were 93.3% and 89.1%, respectively. The study concluded that LOI is a “potentially useful alternative diagnostic test for PAD” in patients with type 2 diabetes.
LOI is a noninvasive procedure similar to ABI; both indices indicate whether it’s safe to apply compression to the limb of a patient who has lower leg ulceration or venous hypertension. With LOI, a pulse oximeter is used in place of a hand-held Doppler to determine the index.
Start planning for World Diabetes Day
It’s not too early to begin planning for World Diabetes Day, November 14. Started by the World Health Organization (WHO) and the International Diabetes Federation (IDF), the day is designed to raise global awareness of diabetes.
Access materials, including posters, a campaign book, and the Word Diabetes Day Logo, from IDF’s website, which also has activity ideas.
WHO estimates that more than 346 million people worldwide have diabetes, and the number is expected to double by 2030. World Diabetes Day is celebrated on November 14 to mark the birthday of Frederick Banting who, along with Charles Best, was instrumental in the discovery of insulin in 1922.
Guidelines for PAD in patients with diabetes and foot ulceration published
February’s issue of Diabetes/Metabolism Research and Reviews includes “Specific guidelines for the diagnosis and treatment of peripheral arterial disease in a patient with diabetes and ulceration of the foot 2011,” which is based on two companion International Working Group on the Diabetic foot papers. The guidelines state that if a patient’s PAD is impairing wound healing, revascularization through bypass or endovascular technique must be considered except in a few cases such as severely frail patients. Limb salvage rates after revascularization procedures are about 80-85%, and there is ulcer healing in > 60% at 12 months.
Other points of particular interest to wound care professionals:
Patients with PAD and a foot infection are at high risk for major limb amputation, so should be treated as a “medical emergency”, preferably within 24 hours.
Half of patients with diabetes, a foot ulcer, and PAD die within 5 years because of higher cardiovascular morbidity and mortality. Cardiovascular risk management should include “support for cessation of smoking, treatment of hypertension, and prescription of a statin as well as low-dose aspirin or clopidrogel.