The elevator door opens and you step in to find yourself face to face with the important person you’ve wanted to meet to discuss your promising idea. It’s the chance you wouldn’t want to miss. But that chance lasts only as long as the elevator ride. You have less than a minute to make an impression. Do you have an elevator speech ready?
What’s an elevator speech?
An elevator speech is any short speech that sells an idea, promotes a business, or markets an individual. It’s a short summary, or pitch, that quickly describes the value of a service, product, or organization. The term is a metaphor for unexpected access to someone to whom you’d like to sell an idea or proposal. It derives from the early days of the Internet boom when web development companies needed venture capital. Firms were swamped with applications for funding, and in many cases, the companies that won the cash were those whose reps had a simple pitch and could explain a business proposal in an elevator in the time it took to ride to their floor.
A great elevator speech describes and sells an idea in less than a minute. Of course, it’s not restricted to elevators. It comes in handy any time and anywhere you need to give a concise presentation to capture someone’s interest so you can move to the next step—a follow-up call, a referral, a meeting, or a partnership.
Why clinicians need an elevator speech
You need to be able to describe what you do, what you’re interested in doing, and how you can be a resource to someone. The ability to sum up a unique aspect of your service or expertise in a way that excites others is a fundamental skill. Doing this in a brief, persuasive manner is an asset for any professional. A good elevator speech should grab one’s attention in a few words and make that person want to know more about you. Here are examples where a good elevator speech would be helpful:
• Thomas goes to a recruitment fair hoping to get an interview at a certain hospital.
• Mary is finishing her master of science degree and is interested in a position in a new wound care clinic.
• Caroline has written a book on grant writing and would like to present her ideas at a conference.
• Brian is interested in research and would like to join the research team.
• Mindy is trying to expand her wound consultation business.
You can use an elevator speech when you want to grab someone’s attention at a meeting, convention, or other social situation. In such situations, people typically ask, “What do you do?” A well-planned elevator speech can make the listener’s ears perk up and want to know more.
How to prepare an elevator speech
Before you can write an elevator speech, you need to know yourself, what you can offer, what problems you can solve, and what benefits you can bring to the prospective contact. For example, you may be an expert in professional communication and know strategies you can teach other staff to promote a better workplace environment.
You also need to know your audience. Will you direct your pitch to an administrator, a unit manager, or staff? You’re more likely to succeed if your elevator speech is targeted to a specific audience and you adjust it to that audience. Try to prepare different pitches for different audiences; a generic pitch is almost certain to fail. (See Key elements of a good elevator speech by clicking the PDF icon above.)
In today’s busy world, clinicians must be able to communicate in a succinct, persuasive manner. Your elevator speech is your introduction to others. It has to be good. Keep practicing it and perfecting it so you can speak with poise and polish. The more often you give it, the better it will become. It’s a great way to put your best foot forward when you have only a small window of opportunity to make a good impression.
Sjodin T. Small Message, Big Impact: The Elevator Speech Effect. New York, NY: Portfolio; 2012. Sprung S, Giang V. 6 keys to delivering a powerful elevator pitch. Business Insider Web site. www .businessinsider.com/terri-sjodin-how-to-deliver- an-elevator-speech-2012-10. October 26, 2012. Accessed October 26, 2012.
Kathleen D. Pagana is a keynote speaker and professor emeritus at Lycoming College in Williamsport, Pennsylvania. She is the author of The Nurse’s Communication Advantage and The Nurse’s Etiquette Advantage. She is also the coauthor of Mosby’s Diagnostic and Laboratory Test Reference, 11th ed. To contact her, visit www.KathleenPagana.com.
The guidelines include recommendations for practice, education, policy, and future resource. Strategies for implementation are given, as well as several useful appendices, such as:
• Debridement Decision-Making Algorithm
• A Guide to Dressing Foot Wounds
• PEDIS: Diabetes Foot Ulcer Classification System
• Offloading Devices
• Optimal Treatment Modalities.
PREPARE is a useful and patient-friendly website designed to help prepare people to make complex medical decisions. The website was developed by clinical researchers from the San Francisco VA Medical Center; the University of California, San Francisco; and NCIRE—The Veterans Health Research Institute.
PREPARE uses videos to provide concrete examples of how to identify what is most important in life; how to communicate that with family, friends, and doctors; and how to make informed medical decisions when the time comes. Users can also download a PDF of a PREPARE pamphlet.
Free guides for infection prevention from APIC
Download two free implementation guides for infection prevention from the Association for Professionals in Infection Control and Epidemiology (APIC):
This revised guide contains strategies for prevention, considerations for specific patient populations, evolving practices, and how to incorporate current regulations.
Topics include:
• C. difficile in pediatrics and skilled nursing facilities
• pathogenesis and changing epidemiology of C. difficile infection diagnosis
• environmental control
• new and emerging technologies
• tools and examples to help apply preventative measures, such as hand hygiene monitoring, environmental cleaning, and isolation compliance.
This guide includes infection-prevention standards, regulations, and best practices, as well as instructions, examples, and tools to conduct surveillance and risk assessments.
One of the worst fears of a wound care clinician is inadvertently compressing a leg with critical limb ischemia—a condition marked by barely enough blood flow to sustain tissue life. Compression (as well as infection or injury) could lead to necrosis, the need for amputation, or even death. The gold standard of practice is to obtain an ankle-brachial index (ABI) before applying compression. However, recent research and expert opinion indicate an elevated or normal ABI is deceptive in patients with advanced diabetes. What’s worse, in the diabetic foot, skin may die from chronic capillary ischemia even when total blood perfusion is normal. For information on how to perform an ABI and interpret results, click on this link. (more…)
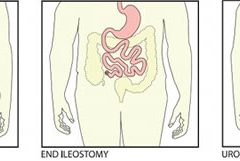
Most patients are distressed to learn they need ostomy surgery to divert stool, urine, or both. Adapting to ostomy surgery can be difficult at best, even with today’s advanced technology and the wide assortment of ostomy supplies available. While recovering from the surgery itself, patients must learn how to contain or control feces or urine and how to minimize odor—without feeling like a social outcast.
This article reviews three types of ostomy surgery—colostomy, ileostomy, and urostomy. Subsequent articles will discuss ostomy management and treatment of stomal and peristomal skin complications. (more…)
Here are resources that can help you in your busy clinical practice by giving you information quickly.
Pressure ulcer resources
Instead of searching through Google or another search engine for pressure ulcer resources, start with this comprehensive list on the Centers for Medicare & Medicaid Services website.
Examples of resources included are:
“Preventing pressure ulcers in hospitals: A toolkit for improving quality of care.” This toolkit from the Agency for Healthcare Research and Quality (AHRQ) is designed to help hospitals in implementing pressure ulcer prevention strategies.
“On-time pressure ulcer healing project.” Another AHRQ initiative, this resource is designed for those working in long-term care facilities.
“Pressure ulcer prevention.” This table from the Institute for Healthcare Improvement lists possible mentors you can work with in the area of ulcer prevention.
“Shawnee Medical Center wound care quick reference guide.” This is a handy one-page reference guide that includes photographs and recommendations.
“How-to guide: Prevent pressure ulcers—pediatric supplement.” This guide, tailored for pediatrics, describes key evidence-based care components for preventing pressure ulcers and describes how to implement these interventions.
You can also access case studies from a variety of facilities around the United States.
The National Lymphedema Network is a nonprofit organization founded in 1988 to provide education and other information to healthcare professionals and patients with lymphedema, as well as the general public. The site includes an explanation of lymphedema that may be helpful for you to use in teaching your patients. It also includes access to some of the articles from the newsletter LymphLink.
Many patients with chronic wounds have diabetes. To ensure those patients receive the best possible care, you can refer to the 2013 Standards of Medical Care in Diabetes from the American Diabetes Association, which were published in the January issue of Diabetes Care.
The journal provides a summary of the revisions and an executive summary of the standards related to each area, including diagnosis, testing, prevention, monitoring, and pharmacologic and nonpharmacologic management.
The guidelines include valuable information related to neuropathy screening and treatment and foot care. Recommendations for foot care include performing an annual comprehensive foot examination to identify risk factors predictive of ulcers and amputations. The foot examination should include inspection, assessment of foot pulses, and testing for loss of protective sensation.
Most of us have had days when we jump from meeting to meeting and at the end of the day wonder, “Did I get anything accomplished or am I more behind than ever?”
Many clinicians tell me that although their wound team meets regularly, the meetings aren’t meaningful enough, leaving the team still facing issues with their wound care program. As a consultant, when I review the wound team agenda, it’s typically missing one or more of four key ingredients:
appropriate member representation
proactive approach that highlights prevention
review of the plan of care and update of the medical record
review of supplies and products. Here’s a closer look at each of these ingredients.
Build a top team
Having the appropriate members on the wound care team is the first ingredient for success. A comprehensive, interdisciplinary team approach is the key to preventing skin breakdown and ensuring good clinical outcomes for residents with skin breakdown. Teams should include representation from nursing, dietary, and physical and occupational therapy, as well as a nurse practitioner or physician.
Nursing representation should include nurses from all three shifts and nursing assistants, who are too often missing from the team. Keep in mind that when it comes to preventing pressure ulcers, nursing assistants carry out most of interventions (for example, turning, incontinence management, heel lift). Even when a patient has a wound, the only intervention carried out by the nurses is the topical treatment; nursing assistants perform all other interventions necessary to ensure healing. Clinicians who empower nursing assistants to have a strong influence with the wound care team—and the program—tend to have very successful prevention programs and good clinical outcomes.
Think prevention
The second key ingredient is prevention. Most wound team meetings only discuss the patients with wounds, missing the bigger goal of preventing wounds in the first place. Once the patients with wounds are discussed, the team should review all high-risk patients to ensure proper preventative measures are in place and care planned. All patients should be quickly reviewed for evidence of:
decline or change in mobility and activity
new onset or change in continence status
decline in nutritional status
decline or change in cognition.
Any triggers in these areas should prompt a review of the plan of care to ensure they are being effectively addressed.
Review and update the plan
The third key ingredient for success is to use meeting time to review and update the plan of care. I’ve observed highly productive meetings and great discussions of the care the facility is providing. Then I review the medical record and discover that none of the interventions discussed are on the plan of care. Always review the patient’s plan of care to ensure it’s accurate, reflects all interventions, and is up to date. This will give you peace of mind that the medical record reflects all the good work you’re doing and helps make the team meetings feel productive.
Discuss products and supplies
The fourth key ingredient is to take the time to quickly discuss current wound care supplies and products with the team. Ask the team if the current supplies are user-friendly, are adequate, provide good outcomes, and are in good working condition.
Many times staff will not say how they’re struggling with, modifying, or not using something until they’re asked. Remember that the most expensive product is the one that doesn’t work or doesn’t get used.
A recipe for success
Using these four key ingredients will lead you to a successful wound team meeting—and a successful program. The mix may not solve your too-many-meetings days, but will give you peace of mind that at least one meeting is productive.
Jeri Lundgren is director of clinical services at Pathway Health in Minnesota. She has been specializing in wound prevention and management since 1990.
An Unna boot is a special dressing of inelastic gauze impregnated with zinc, glycerin, or calamine that becomes rigid when it dries. It is used for managing venous leg ulcers and lymphedema in patients who are ambulatory. When the patient walks, the rigid dressing restricts outward movement of the calf muscle, which directs the contraction force inward and improves the calf-muscle pumping action, thereby improving venous flow. An Unna boot does not provide compression and is contraindicated for arterial insufficiency. (more…)
Chronic venous insufficiency (CVI) is the most common cause of lower extremity wounds. The venous tree is defective, incapable of moving all the blood from the lower extremity back to the heart. This causes pooling of blood and intravascular fluid at the lowest gravitational point of the body—the ankle.
This article has two parts. Part 1 enhances your understanding of the disease and its clinical presentation. Part 2, which will appear in a later issue, explores the differential diagnosis of similar common diseases, the role that coexisting peripheral artery disease (PAD) may play, disease classification of venous insufficiency, and a general approach to therapy.
The most common form of lower extremity vascular disease, CVI affects 6 to 7 million people in the United States. Incidence increases with age and other risk factors. One study of 600 patients with CVI ulcers revealed that 50% had these ulcers for 7 to 9 months, 8% to 34% had them for more than 5 years, and 75% had recurrent ulcers.
Thrombotic complications of CVI include thrombophlebitis, which may range from superficial to extensive. If the thrombophlebitis extends up toward the common femoral vein leaving the leg, proximal ligation may be needed to prevent clot extension or embolization.
Understanding normal anatomy and physiology
Lower extremity veins flow horizontally from the superficial veins to the perforating veins and then into the deep veins. Normally, overall venous blood flows vertically against gravity from the foot and ankle upward toward the inferior vena cava (IVC). This antigravity flow toward the IVC results from muscular contraction around nonobstructed veins and one-way valves that close as blood passes them. These valves prevent abnormal backward blood flow toward the foot and ankle region.
The lower extremities have four types of veins. Superficial veins are located within the subcutaneous tissue between the dermis and muscular fascia. Examples are the greater and lesser (smaller) saphenous veins. Perforating veins connect the superficial veins to the deep veins of the leg. The deep veins are located below the muscular fascia. The communicating veins connect veins within the same system.
The greater saphenous vein is on the leg’s medial (inner) side. It originates from the dorsal veins on top of the foot and eventually drains into the common femoral vein in the groin region. By way of perforating veins, the greater saphenous vein drains into the deep venous system of both the calf and thigh.
The lesser saphenous vein is situated on the lateral (outer) side of the leg and originates from the lateral foot veins. As it ascends, it drains into the deep system at the popliteal vein behind the knee. Communicating veins connect the greater saphenous vein medially and the lesser saphenous vein laterally.
Intramuscular veins are the deep veins within the muscle itself, while the intermuscular veins are located between the muscle groups. The intermuscular veins are more important than other veins in development of chronic venous disease. Below the knee, the intermuscular veins are paired and take on the name of the artery they accompany—for example, paired anterior tibial, paired posterior tibial, and paired peroneal veins. Eventually, these veins form the popliteal vein behind the knee, which ultimately drains into the femoral vein of the groin.
As the common femoral vein travels below the inguinal ligament of the groin, it’s called the external iliac vein. Eventually, it becomes the common iliac vein, which drains directly into the IVC.
Pathophysiology
Abnormally elevated venous pressure stems from the leg’s inability to adequately drain blood from the leg toward the heart. Blood drainage from the leg requires the muscular pumping action of the leg onto the veins, which pump blood from the leg toward the heart as well as from the superficial veins toward the deep veins. Functioning one-way valves within the veins close when blood passes them, preventing blood from flowing backward toward the ankle. This process resembles what happens when you climb a ladder with intact rungs: As you step up from one rung to the next, you’re able to ascend.
CVI and the “broken rung” analogy
If the one-way valves are damaged or incompetent, the “broken rung” situation occurs. Think how hard it would be to climb a ladder with broken rungs: You might be able to ascend the ladder, but probably you would fall downward off the ladder due to the defective, broken rungs.
Normally, one-way valves ensure that blood flows from the lower leg toward the IVC and that the superficial venous system flows toward the deep venous system. The venous system must be patent (open) so blood flowing from the leg can flow upward toward the IVC. Blockage of a vein may result from an acute thrombosis (clot) in the superficial or deep systems. With time, blood may be rerouted around an obstructed vein. If the acute thrombosis involves one or more of the one-way valves, as the obstructing thrombosis opens up within the vein’s lumen, permanent valvular damage may occur, leading to post-thrombotic syndrome—a form of CVI.
CVI may result from an abnormality of any or all of the processes needed to drain blood from the leg—poor pumping action of the leg muscles, damage to the one-way valves, and blockage in the venous system. CVI commonly causes venous hypertension due to reversal of blood flow in the leg. Such abnormal flow may cause one or more of the following local effects:
leg swelling
tissue anoxia, inflammation, or necrosis
subcutaneous fibrosis
Compromised flow of venous blood or lymphatic fluid from the extremity.
“Water balloon” analogy
The effect of elevated venous pressure or hypertension is worst at the lowest gravitational point (around the ankle). Pooling of blood and intravascular fluid around the ankle causes a “water balloon” effect. A balloon inflated with water has a thin, easily traumatized wall. When it bursts, a large volume of fluid drains out. Due to its thicker wall, a collapsed balloon that contains less fluid is more difficult to break than one distended with water.
In a leg with CVI, subcutaneous fluid that builds up requires a weaker force to break the skin and ulcerate than does a nondistended leg with less fluid. This principle is the basis for compression therapy in treating and preventing CVI ulcers.
Effects of elevated venous pressure or hypertension
Increased pressure in the venous system causes:
abnormally high pressure in the superficial veins—60 to 90 mm Hg, compared to the normal pressure of 20 to 30 mm Hg
dilation and distortion of leg veins, because blood refluxes abnormally away from the heart and toward the lower leg and may move from the deep venous system into the superficial veins.
Abnormal vein swelling from elevated pressure in itself may impair an already abnormally functioning one-way valve. For instance, the valve may become more displaced due to the increase in intraluminal fluid, which may in turn worsen hypertension and cause an increase in leg swelling. Increased pressure from swollen veins also may dilate the capillary beds that drain into the veins; this may cause leakage of fluid and red blood cells from capillaries into the interstitial space, exacerbating leg swelling. Also, increased venous pressure may cause fibrinogen to leak from the intravascular plasma into the interstitial space. This leakage may create a fibrin cuff around the capillary bed, which may decrease the amount of oxygen entering the epidermis, increase tissue hypoxia, trigger leukocyte activation, increase capillary permeability, and cause local inflammation. These changes may lead to ulceration, lipodermatosclerosis, or both.
Visible changes may include dilated superficial veins, hemosiderin staining due to blood leakage from the venous tree, atrophie blanche, and lipodermatosclerosis. (See CVI glossary by clicking the PDF icon above.) Both atrophie blanche and lipodermatosclerosis result from local tissue scarring secondary to an inflammatory reaction of the leg distended with fluid.
Lipodermatosclerosis refers to scarring of subcutaneous tissue in severe venous insufficiency. Induration is associated with inflammation, which can cause the skin to bind to the subcutaneous tissue, causing narrowing of leg circumference. Lymphatic flow from the leg also may become compromised and inhibited in severe venous hypertension, causing additional leg swelling.
Patient history
In a patient with known or suspected CVI, a thorough history may lead to a working diagnosis. Be sure to ask the patient these questions:
Do you have pain?
Is your pain worse toward the end of the day?
Is the pain relieved with leg elevation at night?
Is it relieved with leg elevation during the day?
Do you have leg pain that awakens you at night?
How would you describe the pain?
Does the skin on your leg feel tight or irritated?
Have you noticed visible changes of your leg?
Do you have a leg ulcer?
Also determine if the patient has comorbidities that may exacerbate CVI, including PAD, renal failure, venous thrombosis, lymphedema, diabetes mellitus, heart failure, or malnutrition. (See CVI risk factors by clicking the PDF icon above .)
Common CVI symptoms
Approximately 20% of CVI patients have symptoms of the disease without physical findings. These symptoms may include:
tired, “heavy” legs that feel worse toward the end of the day
discomfort that worsens on standing
legs that feel best in the morning after sleeping or after the legs have been
elevated during the day.
Although patients may report leg discomfort, the history indicates that it doesn’t awaken them at night. Be aware that discomfort from CVI differs from that caused by PAD. With PAD, patients may report pain on exercise (claudication), pain with elevation (nocturnal pain), or constant pain (resting pain).
Signs of CVI (with or without ulcers) include:
leg swelling (seen in 25% to 75% of patients)
skin changes (such as hemosiderin staining or dermatitis)
telangiectasia, reticular veins, or both; while these are the most common signs, they represent an overall less severe finding
varicose veins with or without bleeding, occurring in one-third of patients with CVI.
Venous ulcers
Venous ulcers are the most common type of lower extremity ulcer. They’re commonly found on the medial aspect of the lower extremity, from the ankle to the more proximal calf area. Usually, they arise along the course of the greater saphenous vein, but also may be lateral and may occur at multiple locations. They aren’t found above the knee or on the forefoot. Venous ulcers are shallower than arterial ulcers and have considerable exudate consistent with drainage from a ruptured water balloon. They may extend completely around the leg.
CVI: From a heavy sensation to visible changes
In patients with CVI, blood flows within a lower extremity in an abnormal, reverse direction, causing build-up of blood and intravascular fluid around the ankle. Initially, this may cause only a sensation of heavy legs toward the end of the day, with no visible changes. Eventually, it may lead to venous ulcers or other visible changes. This abnormal blood flow results from dysfunction of the normal mechanisms that drain blood from the leg against gravity into the IVC.
Sardina D. Skin and Wound Management Course; Seminar Workbook. Wound Care Education Institute; 2011:92-112.
Donald A. Wollheim is a practicing wound care physician in southeastern Wisconsin. He also is an instructor for Wound Care Education Institute and Madison College. He serves on the Editorial Board for Wound Care Advisor.
If you’re keeping up on wound care, you know a lot of new things are coming to market with enough decent science behind them to make them reasonable options to consider in your practice. And as true-blooded Americans and citizens of the post-industrialized world, we want what’s newest, fastest, and best in class in everything. It’s just our nature.
But does it truly serve us to be eager to try new therapies even when the current treatment plan is successful? Perhaps. We know we must never close our eyes to new developments in our field that can lead to better outcomes. Knowing when and what to change can lead to better outcomes for the patient, the wound, and our collective pocketbook.
I’ve long maintained we can achieve excellent-quality wound care if we just stick to the basics the vast majority of the time. Why? Systemic, psychosocial, and local factors all affect wound healing—not just the dressing or cream. Our job is to provide the optimum environment possible for wound healing. That requires us to look at and support the whole body toward optimum health, not solely the wound.
The basics begin with identifying the cause of the wound and implementing interventions to reduce, control, or eliminate the cause. Next, we strive to manage local and psychosocial factors by choosing topical products that will maintain moisture balance, keep the wound warm, and protect it. If the wound doesn’t show progress toward healing within 2 weeks (or as expected, given the patient’s overall condition and ability to heal), we need to reevaluate the plan and begin making changes.
The best rule is to make one change at a time. That makes it much easier to determine what’s working and what isn’t. Once all the basics are in place and required changes have been made, if healing is still stalled or nonexistent, consider trying the available new products and specialty products.
Never close your clinical mind to advances in the field. To do that would be a disservice to your patients. But you should change the treatment plan only when a change is needed—not just for the sake of changing it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editor-in-Chief Wound Care Advisor
Cofounder, Wound Care Education Institute
Plainfield, Illinois
The number of people with diabetes who are meeting the ABC goals—hemoglobin A1C, blood pressure, and LDL cholesterol—has risen significantly in recent years, according to a study published by Diabetes Care. Patients meeting all three goals rose from about 2% in 1988 to about 19% in 2010.
Gains were made in each of the ABC goals, based on 2007 to 2010 data: 53% of patients met A1C goals, compared to 43% in 1988 to 1994 data; 51% met blood pressure goals, compared to 33%; and 56% met LDL goals, compared to 10%.
Younger people were less likely to meet A1C and cholesterol goals. Compared with non-
Hispanic whites, Mexican Americans were less likely to meet A1C and LDL goals and non-Hispanic blacks were less likely to meet blood pressure and LDL goals.
The researchers analyzed data from the National Health and Nutrition Examination Surveys from 1988–1994, 1999–2002, 2003–2006, and 2007–2010. Nearly 5,000 people age 20 or older participated.
Although progress had been made, the researchers conclude, “Despite significant improvement during the past decade, achieving the ABC goals remains suboptimal among adults with diabetes, particularly in some minority groups.”
Daily bathing with chlorhexidine-impregnated washcloths reduces infection risk
A study in The New England Journal of Medicine reports that daily bathing with chlorhexidine-impregnated washcloths reduces the risk of becoming infected with multidrug-resistant organisms and subsequent development of hospital-acquired bloodstream infections in intensive care unit patients.
“Effect of daily chlorhexidine bathing on hospital-acquired infection” included 7,727 patients in nine intensive care and bone marrow units in six hospitals. The units were randomly assigned to bathe patients with either no-rinse 2% chlorhexidine-impregnated washcloths or nonantimicrobial washcloths for 6 months; then, the units switched to the opposite product for 6 months.
The rate of infection with multidrug-resistant organisms was 23% lower in the chlorhexidine group and the rate of hospital-acquired bloodstream infection was 28% lower in the chlorhexidine group.
Patients tend not to wear custom-made footwear for preventing diabetic foot ulcers
Adherence to wearing prescription custom-made footwear was low among patients with diabetes, neuropathy, and a recently healed plantar foot ulcer, according to a study in Diabetes Care. The low adherence was particularly notable at home, where patients did the most walking.
Factors associated with higher adherence included lower body mass index, more severe foot deformity, and more appealing footwear.
Tedizolid works as well as linezolid in patients with acute bacterial skin infections
A JAMA study says that a 200-mg once-daily dose of oral tedizolid phosphate over 6 days was as effective as 600 mg of oral linezolid every 12 hours for 10 days in patients with acute bacterial skin and skin-structure infections, including cellulitis or erysipelas, major cutaneous abscesses, and wound infections.
A shorter course of tedizolid may be a “reasonable alternative” to linezolid for treating acute bacterial skin and skin-structure infections, the study concludes.
Water-based exercise improves ROM in patients with long-term arm lymphedema
A study of breast cancer survivors (median 10 years after surgery) with lymphedema found that a water-based exercise program improved shoulder range of motion (ROM).
The program consisted of at least twice-weekly water-based exercise for 8 weeks. At first, participants were supervised, but later they exercised independently. Although lymphedema status didn’t change, those who performed water-based exercise had an increase in ROM, showing improvement years after surgery.
Dehydrated amniotic membrane allograft possible option for treating chronic wounds
A dehydrated amniotic membrane allograft (EpiFix) was used to treat four patients whose wounds hadn’t closed after conservative and advanced measures and who had been referred for plastic procedures. A variety of wounds healed (located on the elbow, knee, hand, and ankle) after one to three applications of the amniotic material, which patients tolerated well. The wounds remained closed several months later.
Study casts doubt on MLD’s role in breast cancer–related lymphedema
A meta-analysis published in the World Journal of Surgical Oncology found the “current evidence” from randomized clinical trials “does not support” the use of manual lymphatic drainage (MLD) in preventing or treating lymphedema in patients with breast cancer.
The authors analyzed 10 randomized clinical trials with 566 patients.
CDC issues additional prevention steps for carbapenem-resistant Enterobacteriaceae
On Feb. 14, the Centers for Disease Control and Prevention (CDC) issued additional prevention steps for carbapenem-resistant Enterobacteriaceae (CRE). Increased reports of CRE prompted the action: Of the 37 unusual forms of CRE reported in the U.S., the last 15 have been reported since July 2012.
• When a CRE is identified in a patient with a history of an overnight stay in a healthcare facility (within the last 6 months) outside the U.S., send the isolate to a reference laboratory for confirmatory susceptibility testing and test to determine the carbapenem resistance mechanism.
• For patients admitted to healthcare facilities in the U.S. after recently being hospitalized (within the last 6 months) in countries outside the U.S., consider performing rectal screening cultures to detect CRE colonization, and place patients on contact precautions while awaiting the results.
Examples of Enterobacteriaceae include Klebsiella species and Escherichia coli. CRE are Enterobacteriaceae with high levels of resistance to antibiotics, including carbapenems. CRE infections most commonly occur among patients who are receiving antibiotics and significant medical treatment for other conditions.
At one time or another, all wound care professionals encounter a chronic wound, defined as a wound that fails to heal in an orderly and timely manner. Globally, about 67 million people (1% to 5% of the world’s population) suffer chronic wounds. In the United States, chronic wounds affect 6.5 million people and cost more than $25 billion annually to treat. (more…)
In a busy wound clinic, quick and accurate differential diagnosis of edema is essential to appropriate treatment or referral for comprehensive care. According to a 2010 article in American Family Physician, 80% of lower extremity ulcers result from chronic venous insufficiency (CVI). In 2007, the German Bonn Vein Study found 100% of participants with active venous ulcers also had a positive Stemmer’s sign, indicating lymphedema. (more…)