Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
Xerosis, an abnormal dryness of the skin, is one of the most common skin conditions among patients with type 2 diabetes. While assessing for predictors of foot lesions in patients with diabetes, the authors of one study found that 82.1% of these patients had skin with dryness, cracks, or fissures. An unpublished survey of 105 consecutive patients with diabetes revealed that 75% had clinical manifestations of dry skin. (more…)
The ability to understand or “read” lower-extremity redness in your patient is essential to determining its cause and providing effective treatment. Redness can occur in multiple conditions—hemosiderin staining, lipodermatosclerosis, venous dermatitis, chronic inflammation, cellulitis, and dependent rubor. This article provides clues to help you differentiate these conditions and identify the specific cause of your patient’s lower-extremity redness. (more…)
Each month, Apple Bites brings you a tool you can apply in your daily practice.
Description
A hydrocolloid dressing is a wafer type of dressing that contains gel-forming agents in an adhesive compound laminated onto a flexible, water-resistant outer layer. Some formulations contain an alginate to increase absorption capabilities. The wafers are self-adhering and available with or without an adhesive border and in various thicknesses and precut shapes for such body areas as the sacrum, elbows, and heels. Click here to see examples of
hydrocolloid dressings.
Staphylococcus aureus is one of the most feared human pathogens, causing a wide range of infections. Most wound care professionals can expect to frequently encounter patients with S. aureus infections. Soft-tissue infections caused by S. aureus include impetigo, cellulitis, and cutaneous abscesses, as well as such life-threatening processes as necrotizing fasciitis and pyomyositis (a hematogenous intramuscular abscess). Serious non-soft-tissue infections include septic arthritis, osteomyelitis, pneumonia, endocarditis, and sepsis.
Why is S. aureus such a nasty bug?
S. aureus produces various cellular and extracellular factors involved in the pathogenesis of infection. S. aureus protein A, an important surface protein, helps the organism resist phagocytosis. Also, S. aureus produces several cytotoxins and enzymes that contribute to infection spread and severity. In addition, some strains produce toxins (including toxic shock syndrome toxin-1) that function as superantigens—molecules that nonspecifically trigger release of large amounts of cytokines, leading to a sepsislike condition. Taken together, such factors combine to make S. aureus a dangerous pathogen.
MRSA emergence
When penicillin was introduced in the 1940s, virtually all S. aureus isolates were sensitive to that drug. But soon thereafter, S. aureus strains that produced a β-lactamase enzyme capable of inactivating penicillin became widespread. During the 1950s, outbreaks of penicillin-resistant S. aureus occurred in many U.S. hospitals. Introduction of penicillinase-resistant antibiotics, such as methicillin and oxacillin, temporarily restored the ability to treat all strains of this pathogen using penicillin antibiotics. The first strain of methicillin-resistant S. aureus (MRSA) was described in 1961 shortly after introduction of penicillinase-resistant antibiotics.
The mechanism of methicillin resistance involves a mutation in one of the bacterial cell-wall proteins to which penicillins must bind to kill the bacterium. This mutation renders the organism resistant to all penicillins and penems and almost all cephalosporins.
MRSA incidence has increased steadily to the point where it currently constitutes up to 60% of S. aureus isolates in many U.S. hospitals. These organisms commonly carry genetic material that makes them resistant to various non-β lactam antibiotics as well, leading some to suggest that the term MRSA should stand for multiply resistant S. aureus. S. aureus has continued to mutate in the face of persistent antibiotic pressure. Vancomycin-intermediate S. aureus (VISA) was described in 1997; vancomycin-resistant S. aureus (VRSA), in 2003. Fortunately, these two strains remain rare and haven’t become established pathogens. (See Strains of antibiotic-resistantS. aureus by clicking the PDF icon above.)
Healthcare- versus community-acquired MRSA
Although MRSA initially arose and spread within healthcare settings (chiefly acute-care hospitals), a community-based variant was described in 1998. Called community-
acquired MRSA (CA-MRSA), this variant differs from healthcare-associated MRSA (HCA-MRSA) in more ways than the acquisition site. CA-MRSA occurs predominately in otherwise healthy children and young adults.
It most commonly presents as recurrent cutaneous abscesses, although life-threatening infections (such as necrotizing fasciitis and pneumonia) also have occurred. The propensity to cause cutaneous abscesses isn’t fully understood but may relate partly to production of the Panton-Valentine toxin by many CA-MRSA isolates.
In contrast, HCA-MRSA afflicts mainly older patients, particularly those with chronic illnesses, including chronic wounds. It typically causes wound infections, urinary tract infections, pneumonia, and bacteremia.
Besides these epidemiologic and clinical differences, many CA-MRSA isolates derive from a single clone, known as clone USA 300, whereas HCA-MRSA is composed of multiple non-USA 300 clones. Finally, many CA-MRSA isolates are sensitive to non-β
lactam antibiotics, whereas most HCA-MRSA isolates resist multiple antibiotics. More recently, the distinction between CA-MRSA and HCA-MRSA has been blurred as evidence emerges that CA-MRSA now is being transmitted in healthcare settings as well as in the community.
S. aureus carrier state
Staphylococci are frequent colonizers of humans. Common colonization sites include the skin, anterior nares, axillae, and inguinal regions. Individuals can be colonized continuously or transiently, with nasal carriage rates varying from 20% to 40%. Most S. aureus infections result from the strain carried by the infected patient.
Three patterns of S. aureus carriage exist in humans:
• 20% of individuals are continuously colonized.
• 30% of individuals are intermittently colonized.
• 50% of individuals are never colonized.
The highest carriage rates occur in patients receiving frequent injections (such as insulin-dependent diabetics, hemodialysis patients, and I.V. drug users) and those with chronic skin conditions (for instance, psoriasis or eczema). In the general population, MRSA carriage rates have increased to 1% or 2%, with clinical consequences hinging on the colonizing strain (CA-MRSA versus HCA-MRSA) and host characteristics. The most consistent carriage site is the anterior nares, but many other sites may carry this pathogen, including the axillae, inguinal regions, and perirectal area.
MRSA treatment
Therapy for MRSA infection depends on the infection location and antibiotic sensitivity of the infecting strain.
• Cutaneous abscesses are treated by incision and drainage; antibiotics play a secondary role to adequate drainage.
• Therapy for necrotizing fasciitis caused by MRSA involves aggressive debridement with removal of all necrotic tissue, plus adequate antibiotic therapy. Typically, patients require serial debridement followed by subsequent careful wound care, often with eventual skin grafting.
• Pyomyositis treatment entails drainage of the muscle abscess (which sometimes can be done with percutaneous tube placement instead of open drainage), plus appropriate antibiotic therapy.
Vancomycin has been the mainstay of I.V. therapy for MRSA for decades, but some clinicians are concerned that its effectiveness may be declining due to slowly increasing minimum inhibitory concentrations (the minimum concentration of an
antibiotic needed to inhibit pathogen growth). Other parenteral options have emerged in the last few years. (See I.V. drugs used to treat MRSA by clicking the PDF icon above.) Several oral antibiotics also are available for MRSA treatment. (See Oral agents used to treat MRSA by clicking the PDF icon above.)
Knowing the antibiotic sensitivity pattern of the infecting MRSA strain is crucial to ensuring that the patient receives an appropriate antibiotic. Treatment duration for soft-
tissue infections usually ranges from 7 to 14 days, but bacteremia and bone or joint infections call for more prolonged therapy.
Efforts to eradicate MRSA carriage
Because the carrier state increases the risk of subsequent S. aureus infection, efforts have been made to eradicate carriage. Unfortunately, this has proven to be difficult. A commonly used regimen involves 5 days of twice-daily mupirocin nasal ointment with either chlorhexidine gluconate showers or immersion up to the neck in a dilute bleach solution. However, success in eliminating carriage is limited, although the bleach bath seems to improve eradication rates better than other modalities.
Controlling MRSA in hospitals
How best to control MRSA spread within hospitals is controversial. Some experts advocate an aggressive, “search and destroy” approach involving screening all patients for nasal carriage on admission and initiating contact precautions with subsequent decolonization efforts. Others focus on improving the overall level of hand hygiene and other general infection-control measures, arguing that nasal screening misses at least 20% of MRSA-colonized patients and thus gives an unwarranted sense of security.
Many hospitals use a mixed approach, screening patients suspected to be at high risk for MRSA carriage (such as those admitted from extended-care facilities or to the intensive care unit), while simultaneously trying to improve hand hygiene and general infection-control measures. Recent data suggest MRSA colonization and infection rates have stopped increasing and are beginning to decline.
MRSA is one of the most problematic pathogens encountered on a regular basis, and among the most dangerous pathogens we face. While some MRSA infections are relatively mild, many are serious or life-threatening. Severe soft-tissue infections, such as necrotizing fasciitis and pyomyositis, require surgical debridement or drainage, appropriate antibiotic therapy, and assistance from a wound-care professional to achieve optimal outcomes. n
Selected references
Calfee DP. The epidemiology, treatment and prevention of transmission of methicillin-resistant Staphylococcus aureus. J Infus Nurs. 2011 Nov-Dec;34(6):359-64.
DeLeo FR, Otto M, Kreiswirth BN, Chambers HF. Community-associated meticillin-resistant Staphylococcus aureus. Lancet. 2010 May 1;375(9725): 1557-68.
Ippolito G, Leone S, Lauria FN, et al. Methicillin-resistant Staphylococcus aureus: the superbug. Int J Infect Dis. 2010 Oct;14 Suppl 4:S7-11.
Landrum ML, Neumann C, Cook C, et al. Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010. JAMA. July 4;308:50-9.
Lee AS, Huttner B, Harbarth S. Control of methicillin-resistant Staphylococcus aureus. Infect Dis Clin North Am. 2011 Mar;25(1):155-79.
Moellering RC Jr. MRSA: the first half century. J Antimicrob Chemother. 2012 Jan;67(1):4-11.
Otter JA, French GL. Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection. J Hosp Infect. 2011 Nov:79(3):189-93.
Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant pneumococci, and vancomycin-resistant enterococci. Mayo Clin Proc. 2011 Dec;86(12):1230-43.
Simor AE. Staphylococcal decolonization: an effective strategy for prevention of infection? Lancet Infect Dis. 2011 Dec;11(12):952-62.
Joseph G. Garner is director of the infectious disease division and hospital epidemiologist at the Hospital of Central Connecticut and a professor of medicine at the University of Connecticut.
Hansen’s disease, also called leprosy, is treatable today – and that’s partly thanks to a curious tree and the work of a pioneering young scientist in the 1920s. Centuries prior to her discovery, sufferers had no remedy for leprosy’s debilitating symptoms or its social stigma.
This young scientist, Alice Ball, laid fundamental groundwork for the first effective leprosy treatment globally. But her legacy still prompts conversations about the marginalization of women and people of color in science today.
Alice Augusta Ball, born in Seattle, Washington, in 1892, became the first woman and first African American to earn a master’s degree in science from the College of Hawaii in 1915, after completing her studies in pharmaceutical chemistry the year prior.
After she finished her master’s degree, the college hired her as a research chemist and instructor, and she became the first African American with that title in the chemistry department.
Doctors now understand that leprosy, also called Hansen’s disease, is minimally contagious. But in 1865, the fear and stigma associated with leprosy led authorities in Hawaii to implement a mandatory segregation policy, which ultimately isolated those with the disease on a remote peninsula on the island of Molokai. In 1910, over 600 leprosy sufferers were living in Molokai.
Doctors had attempted to use nearly every remedy imaginable to treat leprosy, even experimenting with dangerous substances such as arsenicand strychnine. But the lone consistently effective treatment was chaulmoogra oil.
Chaulmoogra oil is derived from the seeds of the chaulmoogra tree. Health practitioners in India and Burma had been using this oil for centuries as a treatment for various skin diseases. But there were limitations with the treatment, and it had only marginal effects on leprosy.
The oil is very thick and sticky, which makes it hard to rub into the skin. The drug is also notoriously bitter, and patients who ingested it would often start vomiting. Some physicians experimented with injections of the oil, but this produced painful pustules.
Dr. Isabel Kerr, a European missionary, administering to a patient a chaulmoogra oil treatment in 1915, prior to the invention of the Ball Method. George McGlashan Kerr, CC BY
The Ball Method
If researchers could harness chaulmoogra’s curative potential without the nasty side effects, the tree’s seeds could revolutionize leprosy treatment. So, Hollmann turned to Ball. In a 1922 article, Hollmann documents how the 23-year-old Ball discovered how to chemically adapt chaulmoogra into an injection that had none of the side effects.
The Ball Method, as Hollmann called her discovery, transformed chaulmoogra oil into the most effective treatment for leprosy until the introduction of sulfones in the late 1940s.
In 1920, the Ball Method successfully treated 78 patients in Honolulu. A year later, it treated 94 more, with the Public Health Service noting that the morale of all the patients drastically improved. For the first time, there was hope for a cure.
Ball’s death meant she didn’t have the opportunity to publish her research. Arthur Dean, chair of the College of Hawaii’s chemistry department, took over the project.
Dean mass-produced the treatment and published a series of articles on chaulmoogra oil. He renamed Ball’s method the “Dean Method,” and he never credited Ball for her work.
Ball’s other colleagues did attempt to protect Ball’s legacy. A 1920 article in the Journal of the American Medical Association praises the Ball Method, while Hollmann clearly credits Ball in his own 1922 article.
Ball is described at length in a 1922 article in volume 15, issue 5, of Current History, an academic publication on international affairs. That feature is excerpted in a June 1941 issue of Carter G. Woodson’s “Negro History Bulletin,” referring to Ball’s achievement and untimely death.
Joseph Dutton, a well-regarded religious volunteer at the leprosy settlements on Molokai, further referenced Ball’s work in a 1932 memoir broadly published for a popular audience.
Historians such as Paul Wermager later prompted a modern reckoning with Ball’s poor treatment by Dean and others, ensuring that Ball received proper credit for her work. Following Wermager’s and others’ work, the University of Hawaii honored Ball in 2000 with a bronze plaque, affixed to the last remaining chaulmoogra tree on campus.
In 2019, the London School of Hygiene and Tropical Medicine added Ball’s name to the outside of its building. Ball’s story was even featured in a 2020 short film, “The Ball Method.”
The Ball Method represents both a scientific achievement and a history of marginalization. A young woman of color pioneered a medical treatment for a highly stigmatizing disease that disproportionately affected an already disenfranchised Indigenous population.
In 2022, then-Gov. David Ige declared Feb. 28 Alice Augusta Ball Day in Hawaii. It was only fitting that the ceremony took place on the Mānoa campus in the shade of the chaulmoogra tree.
Flesh-eating bacteria sounds like the premise of a bad horror movie, but it’s a growing – and potentially fatal – threat to people.
In September 2023, the Centers for Disease Control and Prevention issued a health advisory alerting doctors and public health officials of an increase in flesh-eating bacteria cases that can cause serious wound infections.
There are several types of bacteria that can infect open wounds and cause a rare condition called necrotizing fasciitis. These bacteria do not merely damage the surface of the skin – they release toxins that destroy the underlying tissue, including muscles, nerves and blood vessels. Once the bacteria reach the bloodstream, they gain ready access to additional tissues and organ systems. If left untreated, necrotizing fasciitis can be fatal, sometimes within 48 hours.
The bacterial species group A Streptococcus, or group A strep, is the most common culprit behind necrotizing fasciitis. But the CDC’s latest warning points to an additional suspect, a type of bacteria called Vibrio vulnificus. There are only 150 to 200 cases of Vibrio vulnificus in the U.S. each year, but the mortality rate is high, with 1 in 5 people succumbing to the infection.
How do you catch flesh-eating bacteria?
Vibrio vulnificus primarily lives in warm seawater but can also be found in brackish water – areas where the ocean mixes with freshwater. Most infections in the U.S. occur in the warmer months, between May and October. People who swim, fish or wade in these bodies of water can contract the bacteria through an open wound or sore.
Vibrio vulnificus can also get into seafood harvested from these waters, especially shellfish like oysters. Eating such foods raw or undercooked can lead to food poisoning, and handling them while having an open wound can provide an entry point for the bacteria to cause necrotizing fasciitis. In the U.S., Vibrio vulnificus is a leading cause of seafood-associated fatality.
Why are flesh-eating bacteria infections rising?
Vibrio vulnificus is found in warm coastal waters around the world. In the U.S., this includes southern Gulf Coast states. But rising ocean temperatures due to global warming are creating new habitats for this type of bacteria, which can now be found along the East Coast as far north as New York and Connecticut. A recent study noted that Vibrio vulnificus wound infections increased eightfold between 1988 and 2018 in the eastern U.S.
Climate change is also fueling stronger hurricanes and storm surges, which have been associated with spikes in flesh-eating bacteria infection cases.
Aside from increasing water temperatures, the number of people who are most vulnerable to severe infection, including those with diabetes and those taking medications that suppress immunity, is on the rise.
What are symptoms of necrotizing fasciitis? How is it treated?
Early symptoms of an infected wound include fever, redness, intense pain or swelling at the site of injury. If you have these symptoms, seek medical attention without delay. Necrotizing fasciitis can progress quickly, producing ulcers, blisters, skin discoloration and pus.
Treating flesh-eating bacteria is a race against time. Clinicians administer antibiotics directly into the bloodstream to kill the bacteria. In many cases, damaged tissue needs to be surgically removed to stop the rapid spread of the infection. This sometimes results in amputation of affected limbs.
Researchers are concerned that an increasing number of cases are becoming impossible to treat because Vibrio vulnificus has evolved resistance to certain antibiotics.
People who have a fresh cut, including a new piercing or tattoo, are advised to stay out of water that could be home to Vibrio vulnificus. Otherwise, the wound should be completely covered with a waterproof bandage.
People with an open wound should also avoid handling raw seafood or fish. Wounds that occur while fishing, preparing seafood or swimming should be washed immediately and thoroughly with soap and water.
Anyone can contract necrotizing fasciitis, but people with weakened immune systems are most susceptible to severe disease. This includes people taking immunosuppressive medications or those who have pre-existing conditions such as liver disease, cancer, HIV or diabetes.
It is important to bear in mind that necrotizing fasciitis presently remains very rare. But given its severity, it is beneficial to stay informed.
Debbie King barely gave it a second thought when she scraped her right shin climbing onto her friend’s pontoon for a day of boating in the Gulf of Mexico on Aug. 13.
Even though her friend immediately dressed the slight cut, her shin was red and sore when King awoke the next day. It must be a sunburn, she thought.
But three days later, the red and blistered area had grown. Her doctor took one look and sent King, 72, to the emergency room.
Doctors at HCA Florida Citrus Hospital in Inverness, Florida, rushed King into surgery after recognizing the infection as Vibrio vulnificus, a potentially fatal bacterium that kills healthy tissue around a wound. While King lay on the operating table, the surgeon told her husband she would likely die if they didn’t amputate.
Just four days after the scrape, King lost her leg then spent four days in intensive care.
“The flesh was gone; it was just bone,” she said of her leg.
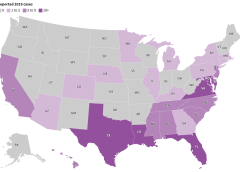
Cases of V. vulnificus are rare. Between 150 and 200 are reported to the Centers for Disease Control and Prevention every year, with about 20% resulting in death. Most are in states along the Gulf of Mexico, but, in 2019, 7% were on the Pacific Coast. Florida averages about 37 cases and 10 deaths a year.
But a rise in cases nationally and the spread of the disease to states farther north — into coastal communities in states such as Connecticut, New York, and North Carolina — have heightened concerns about the bacterium, which can result in amputations or extensive removal of tissue even in those who survive its infections. And warmer coastal waters caused by climate change, combined with a growing population of older adults, may result in infections doubling by 2060, a study in Scientific Reports warned earlier this year.
“Vibrio distributions are driven in large part by temperature,” said Tracy Mincer, an assistant professor at Florida Atlantic University. “The warmer waters are, the more favorable it is for them.”
The eastern United States has seen an eightfold increase in infections over a 30-year period through 2018 as the geographic range of infections shifted north by about 30 miles a year, according to the study, which was cited in a CDC health advisory last month.
The advisory was intended to make doctors more aware of the bacterium when treating infected wounds exposed to coastal waters. Infections can also arise from eating raw or undercooked seafood, particularly oysters, it warned. That can cause symptoms as common as diarrhea and as serious as bloodstream infections and severe blistered skin lesions.
New York and Connecticut this summer issued health warnings about the risk of infection as well. It’s not the first year either state has recorded cases.
“There’s very few cases but when they happen, they’re devastating,” said Paul A. Gulig, a professor in the Department of Molecular Genetics and Microbiology at the University of Florida College of Medicine.
‘An Accident of Nature’
Vibrio has more than 100 strains, including the bacterium that causes cholera, a disease that causes tens of thousands of deaths worldwide each year.
The V. vulnificus strain likes warm brackish waters close to shorelines where the salinity is not as high as in the open sea. Unlike some other Vibrio strains, it has no mechanism to spread between humans.
It’s found in oysters because the mollusks feed by filtering water, meaning the bacterium can become concentrated in oyster flesh. It can enter humans who swim in salty or brackish waters through the slightest cut in the skin. Infections are treated with antibiotics and, if needed, surgery.
“It’s almost an accident of nature,” Gulig said. “They have all these virulence factors that make them really destructive, but we’re not a part of this bug’s life cycle.”
Once inside the human body, the bacteria thrive.
Scientists don’t believe the bacteria eat flesh, despite how they’re often described. Rather, enzymes and toxins secreted by the bacterium as it multiplies break down the human tissue in the area below the skin, causing necrosis, or death of tissue cells.
The infection spreads like wildfire, Gulig said, making early detection critical.
“If you take a pen and mark where the edge of the redness is and then look at that two or four hours later, the redness would have moved,” Gulig said. “You can almost sit there and watch this spread.”
Researchers have conducted studies on the bacteria, but the small number of cases and deaths make it tough to secure funding, said Gulig. He said he switched his research focus to other areas because of the lack of money.
But growing interest in the bacteria has prompted talk about new research at his university’s Emerging Pathogens Institute.
Examining the bacteria’s genome sequence and comparing it with those of Vibrio strains that don’t attack human flesh could yield insights into potential drugs to interfere with that process, Gulig said.
Shock and Loss
Inside the operating room at HCA Florida Citrus, the only signs of King’s infection were on her shin. The surgeon opened that area and began cutting away a bright red mush of dead flesh.
Hoping to save as much of the leg as possible, the doctor first amputated below her knee.
But the bacteria had spread farther than doctors had hoped. A second amputation, this time 5 inches above the knee, had to be performed.
After surgery, King remained in critical care for four days with sepsis, a reaction to infection that can cause organs to fail.
Her son was there when she awakened. He was the one who told her she had lost her leg, but she was too woozy from medication to take it in.
It wasn’t until she was transferred to a rehab hospital in nearby Brooksville run by Encompass Health that the loss sank in.
A former radiation protection technician, King had always been self-reliant. The idea of needing a wheelchair, of being dependent on others — it felt like she had lost part of her identity.
One morning, she could just not stop crying. “It hit me like a ton of bricks,” she said.
Six different rehab staffers told her she needed to meet with the hospital’s consulting psychologist. She thought she didn’t need help, but she eventually gave in and met with Gerald Todoroff.
In four sessions with King, he said, he worked to redirect her perception of what happened. Amputation is not who you are but what you will learn to deal with, he told her. Your life can be as full as you wish.
“They were magic words that made me feel like a new person,” King said. “They went through me like music.”
Physical therapy moved her forward, too. She learned how to stand longer on her remaining leg, to use her wheelchair, and to maneuver in and out of a car.
Now, back in her Gulf Coast community of Homosassa, those skills have become routine. Her husband, Jim, a former oil company worker and carpenter, built an access ramp out of concrete and pressure-treated wood for their single-story home.
But she is determined to walk with the aid of a prosthetic leg. It’s the motivation for a one-hour regimen of physical therapy she does on her own every day in addition to twice-weekly sessions with a physical therapist.
Recovery still feels like a journey but one marked by progress. She has nicknamed her “stump” Peg. She’s now comfortable sharing before and after pictures of her leg.
And she’s made it her mission to talk about what happened so more people will learn about the danger.
“This is the most horrific thing that can happen to anybody,” she said. “But I’d sit back and think, ‘God put you here for a reason — you’ve got more things to do.’”
What to Know About ‘Flesh-Eating’ Bacterium Vibrio vulnificus
Infection Symptoms:
Diarrhea, often accompanied by stomach cramping, nausea, vomiting, and fever.
Wound infections cause redness, pain, swelling, warmth, discoloration, and discharge. They may spread to the rest of the body and cause fever.
Bloodstream infections cause fever, chills, dangerously low blood pressure, and blistering skin lesions.
To Protect Against Vibrio Infections:
Stay out of saltwater or brackish water if you have a wound or a recent surgery, piercing, or tattoo.
Cover wounds with a waterproof bandage if they could come into contact with seawater or raw or undercooked seafood and its juices.
Wash wounds and cuts thoroughly with soap and water after contact with saltwater, brackish water, raw seafood, or its juices.
Who Is Most at Risk:
Anyone can get a wound infection. People with liver disease, cancer, or diabetes, and those over 40 or with weakened immune systems, are more likely to get an infection and have severe complications.
This article was produced in partnership with the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
The Indications and Contraindications for Collagen
What a Wound Wants and Needs; and Why
Considerations of Collagen in Treating & Healing Wounds
Our Speaker: Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).
As a visionary and entrepreneur in the field of mobile medicine, she has operated mobile wound care practices nationwide for many years. She enjoys educating on the art and science of wound healing and how practical solutions apply to healthcare professionals today. Martha enjoys being a positive change in healthcare impacting clients suffering from wounds and skin issues of all etiologies.
Submit below to view the Webinar and download Slidedeck
*By accessing this webinar you are opting in to receiving information from Healthcom Media and Affiliates. Or the details, including your email address/mobile number, may be used to keep you informed about future products and services.
The microbiome is known to play a major role in gut health, but what about our skin? Billions of bacteria reside there, and the probiotic types may hold great potential to prevent infections during wound healing.
Our skin provides a natural barrier to the environment. This is crucial for our health, as skin protects us from invasive pathogens such as bacteria and viruses. (more…)
Physicians evaluate new device to test for cervical cancer. Comparison of Tissue Yield Using Frictional Fabric Brush Versus Sharp Curettage For Endocervical Curettage.
Women undergoing cervical biopsies might have lower odds of repeat tests with a rotating fabric brush than a sharp instrument because the soft device may capture more cells for analysis, a recent study suggests. Furthermore, biopsies with the softer tool may be less painful, researchers say. Cervical biopsies sometimes fail to collect enough cells from the cervix to accurately test for cancer, in which case another biopsy is needed. (more…)
Investigators at the University of California in San Francisco are recruiting people with MS for an international study of the gut microbiome – the population of bacteria in the gut – in MS. They are seeking people with primary progressive MS nationwide (there is no need for onsite visits), as well as people with any other type of MS who can make a one-time visit to San Francisco, New York, Boston or Pittsburgh. The overall purpose of these studies is to investigate the potential role of gut bacteria in MS.
Scientists Focus on Gut Flora for Future Treatments of Autoimmune Diseases
For surgical collaboration; rural telemedicine, nurses and doctors at Hospitals use Google Glass. Indianapolis-based Hodei Technology is bringing Glass to hospitals in two different ways: as a tool for surgeons to teach, communicate, and collaborate (via a product called Ikasi) and, via a product called Gemini, as a new kind of telemedicine, which CEO Guy Mascaro describes as “first person point-of-view telepresence”.
A lot of people think Google Glass, the tech company’s experiment with augmented reality and wearable computing, died when the Glass Explorer program closed up shop in 2015. In fact, the technology has continued to find a home with enterprise applications, particularly in healthcare. (more…)






 Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).
Martha R. Kelso, RN, LNC, HBOT, is the founder and Chief Executive Officer of Wound Care Plus, LLC (WCP).


