I remain absolutely amazed that there are so many people doing the same thing and yet doing it so completely different. Depending on where a patient’s wound care and orders originate from, the care I try to translate from that starting point is always a combination of dressing regimens worthy of computer code in their simplicity. The only thing usually missing is the diagnosis. It’s as though they come from an identical planet in an alternate universe.
The issue is that there is the complete dissociation of what is done for a given wound care problem in one practice setting versus another. Having stayed as far away from hospital-based wound care as possible, I continue to be amazed by hospital wound teams touting their expertise while using two to three times a day dressing changes and therapies that are the antithesis of any identifiable evidence. They actually expect entities receiving their cases (including home healthcare agencies, LTAC, skilled facilities, and others) to copy the identical care scenario regardless of their widely variable situations. In fact, the only constant is the patient and his or her condition. (more…)
Chronic venous leg ulcers (CVLUs) affect nearly 2.2 million Americans annually, including an estimated 3.6% of people over the age of 65. Given that CVLU risk increases with age, the global incidence is predicted to escalate dramatically because of the growing population of older adults. Annual CVLU treatment-related costs to the U.S. healthcare system alone are upwards of $3.5 billion, which are directly related to long healing times and recurrence rates of over 50%.
CVLUs are not only challenging and costly to treat, but the associated morbidity significantly reduces quality of life. That makes it critical for clinicians to choose evidence-based treatment strategies to achieve maximum healing outcomes and minimize recurrence rates of these common debilitating conditions. These strategies, which include compression therapy, specialized dressings, topical and oral medications, and surgery, are used to reduce edema, facilitate healing, and avert recurrence. (more…)
Skin substitutes (also called tissuebased products and dermal replacements) are a boon to chronic wound management when traditional therapies have failed. When selecting skin substitutes for their formularies, wound care professionals have many product options—and many decisions to make.
Repair of skin defects has been a pressing concern for centuries. As early as the 15th century BC, Egyptian physicians chronicled procedures and herbal treatments to heal wounds, including xenografts (skin from another species). The practice of applying allografts (human cadaver skin) to wounds was first documented in 1503. In 1871, autologous skin grafting (skin harvested from the the person with the wound) was tried. Next came epithelial- cell seeding, which involves scraping off the superficial epithelium of healthy skin and transplanting the cells onto the wound. (more…)
Electrical stimulation and pressure ulcer healing in SCI patients A systematic review of eight clinical trials of 517 patients with spinal cord injury (SCI) and at least one pressure ulcer indicates that electrical stimulation increases the healing rate of pressure ulcers. Wounds with electrodes overlaying the wound bed seem to have faster pressureulcer healing than wounds with electrodes placed on intact skin around the ulcer.
As a wound care specialist, you have learned about many skin conditions, some so unusual and rare that you probably thought you would never observe them. I’ve been a nurse for 38 years, with the last 10 years in wound care, and that’s certainly what I thought. But I was wrong. Let me tell you about my challenging patient with…
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when…
Electrical stimulation and pressure ulcer healing in SCI patients A systematic review of eight clinical trials of 517 patients with spinal cord injury (SCI) and at least one pressure ulcer indicates that electrical stimulation increases the healing rate of pressure ulcers. Wounds with electrodes overlaying the wound bed seem to have faster pressureulcer healing than wounds with electrodes placed on intact skin around the ulcer.
Here is a round-up of resources that you may find helpful in your practice. New illustrations for pressure-injury staging The National Pressure Ulcer Advisory Panel (NPUAP) has released new illustrations of pressure injury stages. You can download the illustrations, which include normal Caucasian and non-Caucasian skin illustrations for reference. There is no charge for the illustrations as long as they are being used for educational purposes, but donations to…
By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here’s an overview of cutaneous candidiasis. Cutaneous candidiasis is an infection of the skin caused by the yeast Candida albicans or other Candida species. Here’s a snapshot of this condition.
Topical application of silver nitrate is often used in wound care to help remove and debride hypergranulation tissue or calloused rolled edges in wounds or ulcerations. It’s also an effective agent to cauterize bleeding in wounds. Silver nitrate is a highly caustic material, so it must be used with caution to prevent damage to healthy tissues.
For an ostomy pouching system to adhere properly, the skin around the stoma must be dry and intact. Otherwise, peristomal skin problems and skin breakdown around the stoma may occur. In fact, these problems are the most common complications of surgical stomas. They can worsen the patient’s pain and discomfort, diminish quality of life, delay rehabilitation, increase use of ostomy supplies, and raise healthcare costs. Peristomal skin problems also perpetuate a…
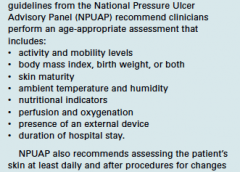
By Jeri Lundgren, BSN, RN, PHN, CWS, CWCN Many factors can contribute to the formation of a pressure ulcer, but it’s rare that one develops in an active, mobile patient. As the National Pressure Ulcer Advisory Panel 2014 guidelines state, “Pressure ulcers cannot form without loading, or pressure on the tissue. Extended periods of lying or sitting on a particular…
Imagine watching your skin tear, bleed, and turn purple. Imagine, too, the pain and disfigurement you’d feel. What if you had to live through this experience repeatedly? That’s what many elderly people go through, suffering with skin tears through no fault of their own. Some go on to develop complications. A skin tear is a traumatic wound caused by shear, friction, or blunt-force trauma that results in a partial-…
This issue marks the fourth anniversary of the “Best of the Best” issue of Wound Care Advisor, the official journal of the National Alliance of Wound Care and Ostomy. Fittingly, it comes during an Olympics year. Since 1904, the Olympics have awarded gold medals to athletes whose performance makes them the “best of the best.” This year, we’re proud to present our own “Best…
By Roxana Reyna, BSN, RNC-NIC, WCC, CWOCN As wound care clinicians, we are trained—and expected—to help heal wounds in patients of any age and to achieve positive outcomes. Basic wound-healing principles apply to all patients, whatever their age or size. The specific anatomy and physiology of vulnerable pediatric patients, however, requires detailed wound care. Unfortunately, little evidence-based research exists to…
Diabetic foot ulcers stem from multiple factors, including peripheral neuropathy, high plantar pressures, decreased vascularity, and impaired wound healing. Contributing significantly to morbidity, they may cause limb loss and death. (See Foot ulcers and diabetes.) Initially, hydrocolloid dressings were developed to function as part of the stomal flange. Based on their success in protecting peristomal skin, they were introduced gradually…
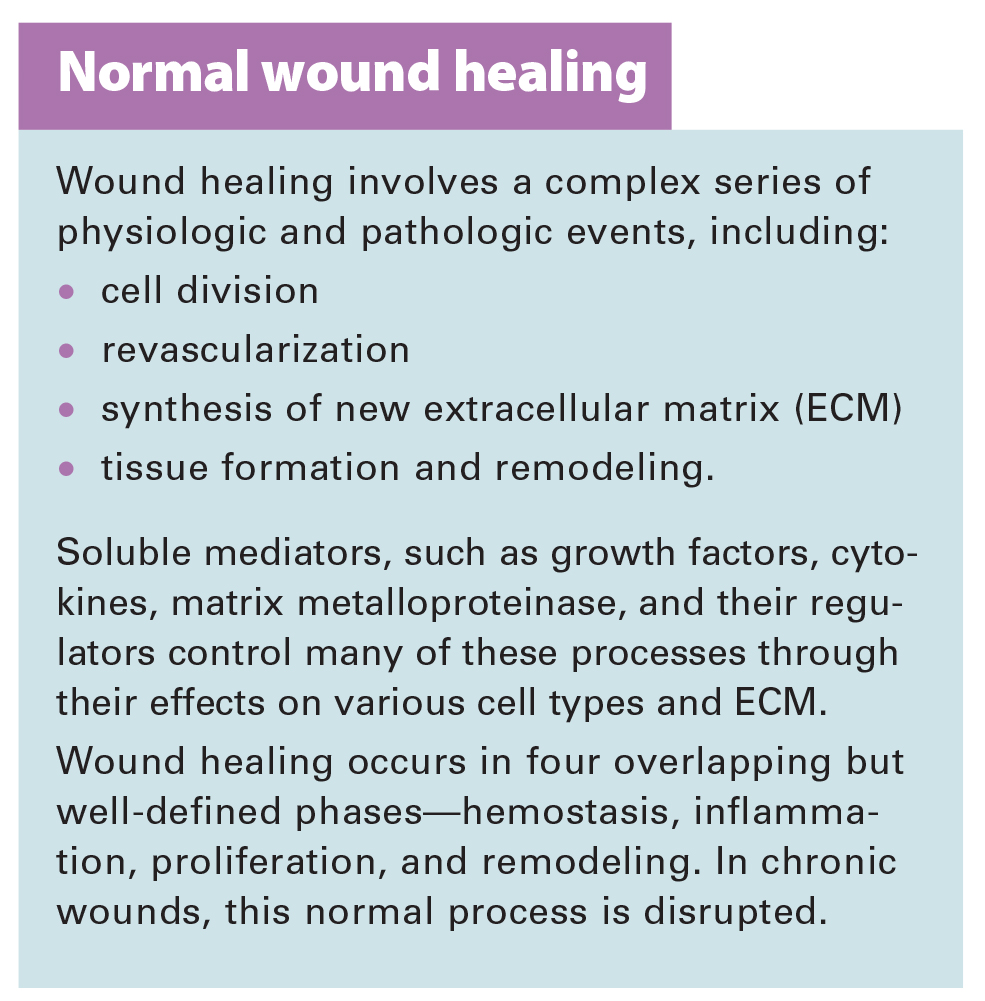
The goal of wound-bed preparation is to create a stable, well-vascularized environment that aids healing of chronic wounds. Without proper preparation, even the most expensive wound-care products and devices are unlikely to produce positive outcomes.
To best prepare the wound bed, you need to understand wound healing physiology and wound care basics, as well as how to evaluate the patient’s overall health and manage wounds that don’t respond to treatment. (See Normal wound healing.)(more…)
Negative pressure wound therapy (NPWT) uses negative pressure to draw wound edges together, remove edema and infectious material, and promote perfusion and granulation tissue development. The tissue stretch and compression created by negative pressure during NPWT promotes tissue perfusion and granulation tissue development through angiogenesis, cellular proliferation, fibroblast migration, increased production of wound healing proteins, and reduction of wound area. NPWT has been used to improve healing in a variety of wounds, including traumatic injuries, surgical wounds, pressure ulcers, diabetic foot ulcers, and venous stasis ulcers. (more…)
At the 2015 Wild on Wounds conference, the interactive workshop “Are You Ready for an Outpatient Reimbursement Challenge?” featured a lively discussion among participants about 25 real-life reimbursement scenarios. Here are the top 10 questions the attendees asked, with the answers I provided.
Q Why is it necessary for qualified healthcare professionals (QHPs) such as physicians, podiatrists, nurse practitioners, physician assistants, and clinical nurse specialists to identify the place of service where they provide wound care services and to correctly state the place of service on their claim forms?
We all lead busy lives, with demanding work schedules and home responsibilities that can thwart our best intentions. Although we know it’s our responsibility to stay abreast of changes in our field, we may feel overwhelmed when we try to make that happen. Keeping clinicians up-to-date on clinical knowledge is one of the main goals of the Wild On Wounds…
As a wound care specialist, you have learned about many skin conditions, some so unusual and rare that you probably thought you would never observe them. I’ve been a nurse for 38 years, with the last 10 years in wound care, and that’s certainly what I thought. But I was wrong. Let me tell you about my challenging patient with…
Value of systematic reviews and meta-analyses in wound care “Systematic reviews and meta-analyses—literature-based recommendations for evaluating strengths, weaknesses, and clinical value,” in Ostomy Wound Management, discusses evidence-based practice and how systematic reviews (SRs) and meta-analyses (MAs) can help improve management of wound care patients. The authors of the article explain evidence-based practice and provide useful definitions for key terms. They…
Start the New Year off right by checking out these resources. Pressure ulcer prevention education Access the following education resources from Wounds International: The webinar “Real-world solutions for pressure ulcer prevention: Optimising the role of support surfaces” includes: • an overview of the issue of pressure ulcers • what to consider when choosing a support surface • how to operationalize…
A fundamental rule of wound care is to treat the “whole” patient, not just the “hole” in the patient. To do this, we need to focus on a holistic approach to healing, which means evaluating everything that’s going on with the patient—from nutrition, underlying diseases, and medications to activity level, social interactions, and even sleep patterns. We know that as…
Developing a pressure ulcer can cause the patient pain, lead to social isolation, result in reduced mobility, and can even be fatal. According to the Agency for Healthcare Research and Quality, estimated costs for each pressure ulcer range from $37,800 to $70,000, and the total annual cost of pressure ulcers in the United States is an estimated $11 billion. Nurses…
Each issue, Apple Bites brings you a tool you can apply in your daily practice. Here are examples of medications that can affect wound healing. Assessment and care planning for wound healing should include a thorough review of the individual’s current medications to identify those that may affect healing outcomes. Clinicians must then weigh the risks and benefits of continuing…
Diabetic foot ulcers stem from multiple factors, including peripheral neuropathy, high plantar pressures, decreased vascularity, and impaired wound healing. Contributing significantly to morbidity, they may cause limb loss and death. (See Foot ulcers and diabetes.) Initially, hydrocolloid dressings were developed to function as part of the stomal flange. Based on their success in protecting peristomal skin, they were introduced gradually…
Immobility affects all our body systems, including our skin. According to the National Pressure Ulcer Advisory Panel, many contributing factors are associated with the formation of a pressure ulcer, with impaired mobility leading the list. So what can clinicians do to prevent harm caused by immobility? One often-overlooked strategy is a restorative nursing program. (See About restorative nursing.) Moving up…
Being positive in a negative situation is not naïve. It’s leadership. — Ralph S. Marston, Jr., author and publisher of The Daily Motivator website Clinicians may encounter many challenges and stressors in the workplace—long hours, rotating shifts, inadequate staffing, poor teamwork, and pressure to achieve higher performance levels in an emotionally and physically demanding field. But hope exists. Positive psychology…
At the 2015 Wild on Wounds conference, the interactive workshop “Are You Ready for an Outpatient Reimbursement Challenge?” featured a lively discussion among participants about 25 real-life reimbursement scenarios. Here are the top 10 questions the attendees asked, with the answers I provided. Q Why is it necessary for qualified healthcare professionals (QHPs) such as physicians, podiatrists, nurse practitioners,…
According to the National Cancer Institute, an estimated 1.6 million new cases of cancer will have been diagnosed in the United States in 2015. During the course of their disease, most cancer patients receive radiation therapy.
Delivering high energy in the form of waves or particles, radiation therapy alters the DNA of cancer cells, causing their death. Radiation can be administered either externally or internally (through materials placed into the body). It’s given in fraction doses, with the total recommended dose divided into daily amounts. Treatment, including the total dose, is determined on an individual basis.
Although improvements have been made in delivery of radiation therapy, approximately 95% of patients who receive it experience a skin reaction. What’s more, radiation therapy commonly is given concurrently with chemotherapy or targeted therapy to improve survival, which increases the toxicity risk. (more…)
As full-thickness wounds heal, they begin to fill in from the bottom upward with granulation tissue. At the same time, wound edges contract and pull together, with movement of epithelial tissue toward the center of the wound (contraction). These epithelial cells, arising from either the wound margins or residual dermal epithelial appendages within the wound bed, begin to migrate in leapfrog or train fashion across the wound bed. Horizontal movement stops when cells meet (contact inhibition). The ideal wound edge is attached to and flush with the wound bed, moist and open with the epithelial rim thin, and pale pink to translucent. (more…)
Nearly all clinicians know exercise is good for our physical and mental health. But incorporating it into our busy lives can be a challenge. The only types of exercise some clinicians have time for are working long shifts, juggling life’s demands, balancing the books, jumping on the bandwagon, climbing the ladder of success, and skipping meals.
Clinicians are in a unique position to help patients change their behavior to improve their health. Ironically, the first behavior clinicians need to change is to work toward improving our own exercise habits. (more…)
Optimizing nutritional status is a key strategy both in preventing and managing pressure ulcers. In patients across all care settings, compromised nutrition— as from poor intake, undesired weight loss, and malnutrition—increases the risk of pressure ulcers. It contributes to altered immune function, impaired collagen synthesis, and decreased tensile strength. In many cases, malnutrition also contributes to wound chronicity and increases the risk for delayed and impaired wound healing. In patients with chronic wounds, such as pressure ulcers, a chronic inflammatory state can induce catabolic metabolism, malnutrition, and dehydration. (more…)


























{kind=link}